You might also like
- Estrés Crónico, Obesidad Visceral. Kyrou y TsigosDocument7 pagesEstrés Crónico, Obesidad Visceral. Kyrou y TsigosBenja MorenoNo ratings yet
- Interaction Between The Circadian Clock and Chronic StressDocument14 pagesInteraction Between The Circadian Clock and Chronic Stressmcruz16No ratings yet
- Tsigos - Stress, Endocrine Physiology and Pathophysiology PDFDocument46 pagesTsigos - Stress, Endocrine Physiology and Pathophysiology PDFTrigonggoNo ratings yet
- Metabolic Response to Critical Illness: A Narrative ReviewDocument10 pagesMetabolic Response to Critical Illness: A Narrative ReviewNguyen van ChienNo ratings yet
- Hypothalamic-Pituitary-Adrenal Axis, Neuroendocrine Factors and StressDocument7 pagesHypothalamic-Pituitary-Adrenal Axis, Neuroendocrine Factors and Stresssarysulastio100% (1)
- 1 s2.0 S0959438899800166 MainDocument7 pages1 s2.0 S0959438899800166 MainEzgi ÖzbahçeliNo ratings yet
- HHS Public Access: Regulation of The Hypothalamic-Pituitary-Adrenocortical Stress ResponseDocument40 pagesHHS Public Access: Regulation of The Hypothalamic-Pituitary-Adrenocortical Stress ResponseSueNo ratings yet
- Stress and The HPA Axis: Balancing Homeostasis and FertilityDocument15 pagesStress and The HPA Axis: Balancing Homeostasis and Fertilitykazuto kirigayaNo ratings yet
- Chen Et Al., 2015. Models and Methods To Investigate Acute Stress Responses in CattleDocument28 pagesChen Et Al., 2015. Models and Methods To Investigate Acute Stress Responses in CattleAnahi MedinaNo ratings yet
- Stress &healthDocument18 pagesStress &healthsatmayaniNo ratings yet
- Stress Hormones and Inmune SystemDocument11 pagesStress Hormones and Inmune SystemRocío Donaire CortésNo ratings yet
- Paredes2013 - Cortisol The Villain in Metabolic SyndromeDocument9 pagesParedes2013 - Cortisol The Villain in Metabolic SyndromePaulo CesarNo ratings yet
- Metabolic Response to Critical Illness: A Review of Pathophysiology and ManagementDocument10 pagesMetabolic Response to Critical Illness: A Review of Pathophysiology and ManagementValentina bustamanteNo ratings yet
- Stress and The Gastrointestinal Tract: ReviewDocument8 pagesStress and The Gastrointestinal Tract: ReviewsufaNo ratings yet
- Hubungan Stres, Imun Dan SAR PDFDocument5 pagesHubungan Stres, Imun Dan SAR PDFdrgzanadaulNo ratings yet
- A Healthy Body in A Healthy Mind and Vice VersaDocument5 pagesA Healthy Body in A Healthy Mind and Vice VersaMelany Martinez ThomasNo ratings yet
- Respuesta Humana Al EstresDocument10 pagesRespuesta Humana Al EstresmorbreirNo ratings yet
- tmp33F4 TMPDocument7 pagestmp33F4 TMPFrontiersNo ratings yet
- Stress Induced Immunosupression and Physical PerformanceDocument4 pagesStress Induced Immunosupression and Physical PerformanceJoão OliveiraNo ratings yet
- Anesthesia, Analgesia, and The Surgical Stress ResponseDocument8 pagesAnesthesia, Analgesia, and The Surgical Stress Responsejannatin aliya indrinaNo ratings yet
- Physiology & Behavior: SciencedirectDocument11 pagesPhysiology & Behavior: SciencedirectMarcell MolnárNo ratings yet
- El Efecto de la dieta sobre los niveles de cortisolDocument9 pagesEl Efecto de la dieta sobre los niveles de cortisolmededep273No ratings yet
- Mcewen & Seeman Allostatic LoadDocument18 pagesMcewen & Seeman Allostatic LoadAlexei70No ratings yet
- Adrenal Fatigue: Enhancing Quality of Life For Patients With A Functional DisorderDocument6 pagesAdrenal Fatigue: Enhancing Quality of Life For Patients With A Functional Disordercraig10140% (1)
- HHS Public Access: Chronopharmacology of GlucocorticoidsDocument43 pagesHHS Public Access: Chronopharmacology of GlucocorticoidsCami Elena100% (1)
- Respuesta Metabolica Al Trauma Cap 1 FonsecaDocument6 pagesRespuesta Metabolica Al Trauma Cap 1 FonsecaJulio Magaña QuiñonesNo ratings yet
- 3 - Maccari, S. - 2014Document17 pages3 - Maccari, S. - 2014João PedroNo ratings yet
- Metabolic Response to TraumaDocument8 pagesMetabolic Response to TraumaNeiana CarolinaNo ratings yet
- La Respuesta Metabolica y Endocrina Al Trauma 2023Document5 pagesLa Respuesta Metabolica y Endocrina Al Trauma 2023marisol ocampoNo ratings yet
- Stress Alters Gut Microbiome Impacting Mental HealthDocument6 pagesStress Alters Gut Microbiome Impacting Mental HealthLori EsbeltoNo ratings yet
- Glaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionDocument9 pagesGlaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionFranco Paolo Maray-GhigliottoNo ratings yet
- Jais e Bruning (2017) Hypothalamic Inflammation in Obesity and Metabolic DiseaseDocument10 pagesJais e Bruning (2017) Hypothalamic Inflammation in Obesity and Metabolic DiseaseAna Flávia SordiNo ratings yet
- The Effect of Diet Components On The Level of CortDocument9 pagesThe Effect of Diet Components On The Level of CortAmada Flores RubioNo ratings yet
- 1 PDFDocument11 pages1 PDFJoeljar Enciso SaraviaNo ratings yet
- Nej MR A 1905136Document11 pagesNej MR A 1905136carlosalayon2No ratings yet
- J BBR 2021 113410Document12 pagesJ BBR 2021 113410VALERIA VERANO ASIAINNo ratings yet
- Physiology of Stress, Anxiety, and its DiagnosisDocument12 pagesPhysiology of Stress, Anxiety, and its DiagnosisMohamad Arbian KarimNo ratings yet
- Psychological Stress On ImmunityDocument14 pagesPsychological Stress On Immunityyuliana fatmalaNo ratings yet
- Peran Jam Sirkadian Dalam Mengatur Fungsi SelDocument22 pagesPeran Jam Sirkadian Dalam Mengatur Fungsi SelAldi SanusiNo ratings yet
- Vaneck2004 Perceivedstressandsalivarycortisol 1Document8 pagesVaneck2004 Perceivedstressandsalivarycortisol 1adde midian putra chafidNo ratings yet
- Stress and ImmunityDocument18 pagesStress and ImmunityplancheNo ratings yet
- Systemic Response To InjuryDocument4 pagesSystemic Response To InjuryDoc Prince CaballeroNo ratings yet
- Stress and ImmunityDocument5 pagesStress and ImmunitymadeNo ratings yet
- Notes Stress Adaptation PDFDocument19 pagesNotes Stress Adaptation PDFAnil PatelNo ratings yet
- Impacts of StressDocument7 pagesImpacts of StressMovie CentralNo ratings yet
- Acta Physiologica - 2018 - Persson - Circadian RhythmsDocument2 pagesActa Physiologica - 2018 - Persson - Circadian Rhythmsamyralmr112No ratings yet
- General Adaptation Syndrome TheoriesDocument4 pagesGeneral Adaptation Syndrome TheoriesHema JothyNo ratings yet
- CHROUSOS, George 2009 - Stress and Disorders of The Stress SystemDocument8 pagesCHROUSOS, George 2009 - Stress and Disorders of The Stress SystemRafael MagalhãesNo ratings yet
- Mechanisms of Stress in The Brain: ReviewDocument11 pagesMechanisms of Stress in The Brain: ReviewVissente TapiaNo ratings yet
- Ayuno IntermitenteDocument11 pagesAyuno IntermitenteNancyRojo3gmail.comNo ratings yet
- The Metabolic and Endocrine Response To TraumaDocument4 pagesThe Metabolic and Endocrine Response To TraumaSalvador Jimenez MagosNo ratings yet
- Stress-Related Changes in Oesophageal PermeabilityDocument4 pagesStress-Related Changes in Oesophageal PermeabilitySibro MilsiNo ratings yet
- Homeostasis 2Document15 pagesHomeostasis 2Luis MangelNo ratings yet
- The Role of Stress in Gastrointestinal DisordersDocument10 pagesThe Role of Stress in Gastrointestinal DisordersEstefanía Páez CoyNo ratings yet
- Corticosteroid Adverse Effects - StatPearls - NCBI BookshelfDocument12 pagesCorticosteroid Adverse Effects - StatPearls - NCBI Bookshelfantonio.mastrangelo.999No ratings yet
- The Potential Action of Ssris in The Treatment of Skin Diseases Including Atopic Dermatitis and Slow Healing WoundsDocument9 pagesThe Potential Action of Ssris in The Treatment of Skin Diseases Including Atopic Dermatitis and Slow Healing WoundsJosé Luis MacedoNo ratings yet
- StressDocument8 pagesStressVatsala MirnaaliniNo ratings yet
- Cell Biology Assays: Essential MethodsFrom EverandCell Biology Assays: Essential MethodsFanny JaulinNo ratings yet
- Simply Supported Beam ReactionsDocument4 pagesSimply Supported Beam ReactionsRushi TutorNo ratings yet
- Detailed Lesson Plan Boyle's LawDocument9 pagesDetailed Lesson Plan Boyle's LawTeacher Derick Daet86% (7)
- Airway Management in The Critically Ill: ReviewDocument9 pagesAirway Management in The Critically Ill: ReviewQuarmina HesseNo ratings yet
- Zooniverse Book 2022Document28 pagesZooniverse Book 2022Dr Pankaj DhussaNo ratings yet
- A Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiDocument7 pagesA Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiShabir AhmadNo ratings yet
- Measurement of Level in A Tank Using Capacitive Type Level ProbeDocument13 pagesMeasurement of Level in A Tank Using Capacitive Type Level ProbeChandra Sekar100% (1)
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsnonzero15No ratings yet
- Idioms and Phrases MCQs - English Grammar For Competitive ExamsDocument6 pagesIdioms and Phrases MCQs - English Grammar For Competitive ExamsgeologistlakhanNo ratings yet
- Engineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignDocument28 pagesEngineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignMehdi NouriNo ratings yet
- Impex Kitchen Appliances PDFDocument4 pagesImpex Kitchen Appliances PDFqwqw11No ratings yet
- #10 VHB SGT-APT Design SummaryDocument2 pages#10 VHB SGT-APT Design SummarySenthil KumarNo ratings yet
- Fire Crunch. M 08 Bushfire Attack Level BAL FZ TestedDocument3 pagesFire Crunch. M 08 Bushfire Attack Level BAL FZ TestedTimaiagNo ratings yet
- Determining The Thickness of Glass in Airport Traffic Control Tower CabsDocument17 pagesDetermining The Thickness of Glass in Airport Traffic Control Tower CabsAdán Cogley CantoNo ratings yet
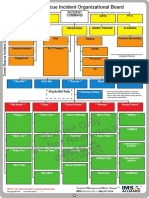
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- Monthly Fire Extinguisher Inspection ChecklistDocument2 pagesMonthly Fire Extinguisher Inspection ChecklistisaacbombayNo ratings yet
- Enzyme ActivityDocument3 pagesEnzyme ActivityNabindra Ruwali100% (2)
- Dip HenyDocument60 pagesDip HenyJinn Tanakrit HansuranantNo ratings yet
- Transcript Ken Robinson 2010 NewDocument34 pagesTranscript Ken Robinson 2010 NewCarmen Maria FluturaşNo ratings yet
- Fetal and Placental Development - FETAL Sac, Umbilical Cord .Abnormalities of PlacentaDocument150 pagesFetal and Placental Development - FETAL Sac, Umbilical Cord .Abnormalities of PlacentaKripa SusanNo ratings yet
- The Affinity Laws of Centrifugal PumpsDocument5 pagesThe Affinity Laws of Centrifugal Pumpssba98No ratings yet
- Training ManualDocument41 pagesTraining Manualemiliow_1100% (3)
- Melese Hotel ST ReportDocument74 pagesMelese Hotel ST ReportKidist MollaNo ratings yet
- Rotating Sharp Shooting Multi Target Mechanism Improves Military AimDocument13 pagesRotating Sharp Shooting Multi Target Mechanism Improves Military AimVishal GNo ratings yet
- LUKAS Product Information-2Document2 pagesLUKAS Product Information-2Flavian ZfmNo ratings yet
- Friends of Hursley School: Late Summer NewsletterDocument6 pagesFriends of Hursley School: Late Summer Newsletterapi-25947758No ratings yet
- Imsa Catalog Imsa CatDocument16 pagesImsa Catalog Imsa CatDaniel TelloNo ratings yet
- Ic M802 UDocument79 pagesIc M802 Uharis_fikriNo ratings yet
- Slovakia C1 TestDocument7 pagesSlovakia C1 TestĐăng LêNo ratings yet
- Subjects Verbs PrepositionsDocument11 pagesSubjects Verbs Prepositionsგუგა ნოსელიძეNo ratings yet
- Solitaire Premier - Presentation (Small File)Document18 pagesSolitaire Premier - Presentation (Small File)Shrikant BadheNo ratings yet