You might also like
- NCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDocument5 pagesNCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDud AccNo ratings yet
- Obstetric Assessment ToolDocument5 pagesObstetric Assessment ToolDudil GoatNo ratings yet
- Example of A Psychosocial Assessment PDFDocument8 pagesExample of A Psychosocial Assessment PDFMichael Alima100% (1)
- Clinical Clerkship Survival Guide: USF Morsani College of Medicine Class of 2020Document56 pagesClinical Clerkship Survival Guide: USF Morsani College of Medicine Class of 2020Lawangeenz40% (5)
- Certificate of ConfinementDocument1 pageCertificate of Confinementsonya100% (2)
- Medical CertificateDocument1 pageMedical CertificateCherry-Anne LetiNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 Palarogtunida100% (1)
- Certificate of ConfinementDocument1 pageCertificate of Confinementcath riguerNo ratings yet
- Palaro 2009 Medical CertificateDocument1 pagePalaro 2009 Medical CertificateHari Ng Sablay100% (1)
- Body Mass Index Form Medical Exam CoqcDocument1 pageBody Mass Index Form Medical Exam CoqcPaulo Justin Tabangcora OropillaNo ratings yet
- Ophthalmological Society of Bangladesh (OSB)Document44 pagesOphthalmological Society of Bangladesh (OSB)george samNo ratings yet
- Doctors Order FormDocument1 pageDoctors Order FormsaguliteNo ratings yet
- Admission Notes (Fdar)Document2 pagesAdmission Notes (Fdar)Ysabela Kim Raz CarboNo ratings yet
- Assessment Form: Cebu Normal UniversityDocument8 pagesAssessment Form: Cebu Normal UniversityLauren JalandoniNo ratings yet
- Physical Assessment Form (Adult)Document7 pagesPhysical Assessment Form (Adult)Mart Juaresa YambaoNo ratings yet
- MedicalCertificate (Regular)Document1 pageMedicalCertificate (Regular)Gilbert Guzman TurarayNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanTrisha Selga SanciangcoNo ratings yet
- Clinic 5Document1 pageClinic 5nandyanuaNo ratings yet
- Nursing Care Plan: Identified Problem: Nursing DiagnosisDocument2 pagesNursing Care Plan: Identified Problem: Nursing DiagnosisJohn Pearl FernandezNo ratings yet
- Nursing Care Plan: Identified Problem: Nursing DiagnosisDocument2 pagesNursing Care Plan: Identified Problem: Nursing DiagnosisChristine Pialan SalimbagatNo ratings yet
- Drug Study FormatDocument3 pagesDrug Study FormatMary ChriciaNo ratings yet
- OB Endorsement Format CS FINALDocument4 pagesOB Endorsement Format CS FINALvannieloveNo ratings yet
- School-Based Immunization Masterlist of Learners GradeDocument9 pagesSchool-Based Immunization Masterlist of Learners GradeRamuel Edrian Tugade PelayoNo ratings yet
- History and Physical ExaminationDocument7 pagesHistory and Physical ExaminationCHYNNA ALBERTNo ratings yet
- Rle WorksheetDocument8 pagesRle WorksheetLiza AingelicaNo ratings yet
- PRC FormDocument6 pagesPRC FormTony EvanNo ratings yet
- NCP, DTR, HTP and Play TherapyDocument4 pagesNCP, DTR, HTP and Play TherapyQuiannë Delos ReyesNo ratings yet
- AUC Health ClearanceDocument2 pagesAUC Health ClearanceNatasha ReddyNo ratings yet
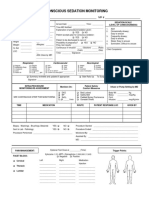
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Rle WorksheetDocument9 pagesRle WorksheetLiza AingelicaNo ratings yet
- Tanzania Baselinesynthetic - AnneDocument45 pagesTanzania Baselinesynthetic - AnneanneNo ratings yet
- Community Nursing Care PlanDocument3 pagesCommunity Nursing Care PlanLeyland Mojeca de GuzmanNo ratings yet
- BHW Monthly ReportDocument2 pagesBHW Monthly Reportsucuanojoan199No ratings yet
- Athlete Medical Certificate InvitationalDocument1 pageAthlete Medical Certificate InvitationalRo Fai DaNo ratings yet
- 2020 - MedicalCertificate (SCOUTS)Document1 page2020 - MedicalCertificate (SCOUTS)Dennmark IgutNo ratings yet
- 032 - Pain Flow SheetDocument8 pages032 - Pain Flow Sheetعبدالله الرعويNo ratings yet
- Kutis Kilatis FormDocument5 pagesKutis Kilatis Formsan dugoNo ratings yet
- Anadjah Ebrahim MCDocument1 pageAnadjah Ebrahim MCMusaiden EbrahimNo ratings yet
- ReferenceDocument2 pagesReferenceVelNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateJM Llameg IINo ratings yet
- Live @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsDocument5 pagesLive @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsJoy SalvadorNo ratings yet
- Referral Forms Referral Forms: - DAY CARE Center - DAY CARE CENTERDocument1 pageReferral Forms Referral Forms: - DAY CARE Center - DAY CARE CENTERMonteza Dela SernaNo ratings yet
- (Name of Student) (Name of Student)Document1 page(Name of Student) (Name of Student)Flor TriaNo ratings yet
- Assessment - NursingDocument8 pagesAssessment - NursingRenee StewartNo ratings yet
- NURSING CARE PLAN TemplateDocument2 pagesNURSING CARE PLAN TemplateK.A.ANo ratings yet
- Nursing Care Plan: Adventist University of The PhilippinesDocument10 pagesNursing Care Plan: Adventist University of The PhilippinesMilcah BartolomeNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroAllen EndayaNo ratings yet
- OCSA Clinical Student Health FormDocument2 pagesOCSA Clinical Student Health Formimdaking123No ratings yet
- Barangay Assisted Booking Form: CODE: D1ADocument4 pagesBarangay Assisted Booking Form: CODE: D1AChristine May CagaraNo ratings yet
- Counselor Intern Eval PacketDocument9 pagesCounselor Intern Eval PacketCathyNo ratings yet
- Application For Leave of AbsenceDocument1 pageApplication For Leave of AbsenceRoi Vince PiliNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateAnujNo ratings yet
- SBI - Masterlist - Blank FormsDocument19 pagesSBI - Masterlist - Blank FormsCasey NonNo ratings yet
- Guided Notes (WK 5)Document5 pagesGuided Notes (WK 5)Thanh ThảoNo ratings yet
- Lonzaga Assessment PDFDocument7 pagesLonzaga Assessment PDFNiño Naryana Luke PanchoNo ratings yet
- Nursing Care Plan FormatDocument1 pageNursing Care Plan FormatRose Camille Delos Santos DatuinNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanAirglow GNo ratings yet
- Family Nursing Care PlanDocument4 pagesFamily Nursing Care PlanAngela CudiaNo ratings yet
- Interventions Cheat SheetDocument3 pagesInterventions Cheat Sheetejama.johnsonNo ratings yet
- Apta Eval-Fax Version Asapt 2007Document4 pagesApta Eval-Fax Version Asapt 2007Abdur RasyidNo ratings yet
- CV Template For Any Type of JobDocument1 pageCV Template For Any Type of JobM Sufiyan AliNo ratings yet
- The Beginning of The COVID19 Outbreak in MalaysiaDocument2 pagesThe Beginning of The COVID19 Outbreak in MalaysiaBellaNo ratings yet
- Curriculum Vitae: Experience Summary: Ancy T CheriyanDocument3 pagesCurriculum Vitae: Experience Summary: Ancy T CheriyanGloria JaisonNo ratings yet
- Hbsag Form New 2021Document1 pageHbsag Form New 2021GCMDHNo ratings yet
- Standard Operating Procedure Checklist To Prevent Covid19 For Warangal Project SiteDocument1 pageStandard Operating Procedure Checklist To Prevent Covid19 For Warangal Project SiteImranuddin SyedNo ratings yet
- PTS Bahasa Inggris XDocument3 pagesPTS Bahasa Inggris XDesy PutriNo ratings yet
- A Virtual Hospital Pharmacy Inventory: An Approach To Support Unexpected DemandDocument5 pagesA Virtual Hospital Pharmacy Inventory: An Approach To Support Unexpected DemandrahmatNo ratings yet
- ADL Online ReportsDocument1 pageADL Online ReportsEASILY SUCCESSNo ratings yet
- PCSO Malasakit Centers Asof20220421Document5 pagesPCSO Malasakit Centers Asof20220421carlo laguraNo ratings yet
- Adults Perspectives On Cultural, Social and Professional Support in Palliative CareDocument8 pagesAdults Perspectives On Cultural, Social and Professional Support in Palliative CareFatimah FajarNo ratings yet
- Video Case - Laying Out Arnold Palmer Hospital's New Facility 1Document2 pagesVideo Case - Laying Out Arnold Palmer Hospital's New Facility 1Carolina ChitivaNo ratings yet
- Patient Satisfaction With Nursing Care in Ethiopia: A Systematic Review and Meta-AnalysisDocument12 pagesPatient Satisfaction With Nursing Care in Ethiopia: A Systematic Review and Meta-AnalysisgiviNo ratings yet
- Sic 235Document2 pagesSic 235Belal AhmedNo ratings yet
- Care Delivery ModelDocument5 pagesCare Delivery Modelapi-351096424No ratings yet
- Flow Diagram: SHOULDICE HOSPITAL - Simplified ProcessDocument1 pageFlow Diagram: SHOULDICE HOSPITAL - Simplified ProcessJeffery KaoNo ratings yet
- 0 - Proposal 2.4Document29 pages0 - Proposal 2.4Limie LimieNo ratings yet
- Affidavit of Undertaking - ValezaDocument2 pagesAffidavit of Undertaking - ValezaRelina ArellanoNo ratings yet
- Denah Rumah Sakit - 9 LantaiDocument8 pagesDenah Rumah Sakit - 9 LantaiNawan ArdiantNo ratings yet
- Quality of Hospital Services PDFDocument6 pagesQuality of Hospital Services PDFEkramul HaqueNo ratings yet
- Organograma HospitalDocument3 pagesOrganograma HospitalRodolfo RodriguesNo ratings yet
- Ac 02 Nov 22 Dec 312023 Unilever Philippines Principals AffiliatedDocument286 pagesAc 02 Nov 22 Dec 312023 Unilever Philippines Principals AffiliatedSusan ValloyasNo ratings yet
- ABC Blood Letting InvitationDocument2 pagesABC Blood Letting InvitationKeeshia Tenise BadillesNo ratings yet
- Reconstruction and Rehabilitation in Head and Neck Cancer 2019Document365 pagesReconstruction and Rehabilitation in Head and Neck Cancer 2019Omar VillamizarNo ratings yet
- Quezon City University 673 Quirino Highway, San Bartolome, Novaliches, Quezon City, PhilippinesDocument6 pagesQuezon City University 673 Quirino Highway, San Bartolome, Novaliches, Quezon City, Philippinesshayn delapenaNo ratings yet
- Individual Performance Commitment and Review (Ipcr) : Abbey Jane D. BaluyutDocument2 pagesIndividual Performance Commitment and Review (Ipcr) : Abbey Jane D. BaluyutJericko MandapNo ratings yet
- Rev Plans For 20eb0110 - Provincial HospitalDocument20 pagesRev Plans For 20eb0110 - Provincial HospitalElvin AsanasNo ratings yet
- NHM Ec 120923Document9 pagesNHM Ec 120923Ashish PatelNo ratings yet
- Bahasa InggrisDocument3 pagesBahasa InggrisKhlsy RayaNo ratings yet