You might also like
- Philippine Veterans ID Application RequirementsDocument2 pagesPhilippine Veterans ID Application RequirementsBohol FSEO Annex100% (1)
- Bio-Data of Foreign Domestic Worker (FDWDocument4 pagesBio-Data of Foreign Domestic Worker (FDWAndika Luhur PambudiNo ratings yet
- Homeroom Guidance Module 2Document2 pagesHomeroom Guidance Module 2Rd DavidNo ratings yet
- NCIP COC Form 1Document2 pagesNCIP COC Form 1Pelonio Eusebio100% (7)
- Revitalized Homeroom Guidance Program For Grade 10Document1 pageRevitalized Homeroom Guidance Program For Grade 10RON D.C.No ratings yet
- Eccd Front PageDocument1 pageEccd Front PageOFW SF100% (2)
- Membership Rank Worksheet BSPDocument4 pagesMembership Rank Worksheet BSPethanix100% (1)
- Math With TosDocument9 pagesMath With Tos'Dilenma KukurikuNo ratings yet
- CEAP App Form-1 PDFDocument1 pageCEAP App Form-1 PDFNeirish fainsanNo ratings yet
- Promissory Note: Iloilo Doctors' CollegeDocument1 pagePromissory Note: Iloilo Doctors' CollegeJon DoeNo ratings yet
- Book ReportDocument4 pagesBook ReportRicky Martin0% (1)
- Genealogy Form New 2021Document2 pagesGenealogy Form New 2021Jowena BaliuagNo ratings yet
- Learning Strand I - EnglishDocument29 pagesLearning Strand I - EnglishMaricel MaapoyNo ratings yet
- Customer Satisfaction On QRZ Family RestaurantDocument1 pageCustomer Satisfaction On QRZ Family RestaurantAries Roy Saplagio AungonNo ratings yet
- Biodata Format For JobDocument1 pageBiodata Format For JobFairoza Fidelyn Villaruz50% (2)
- Equivalents Record Form: I. Educational Attainment & Civil Service EligibilityDocument2 pagesEquivalents Record Form: I. Educational Attainment & Civil Service EligibilityGrace StraceNo ratings yet
- Individual Inventory Form Personalbackground: Binmaley Catholic School, Inc. Binmaley, PangasinanDocument3 pagesIndividual Inventory Form Personalbackground: Binmaley Catholic School, Inc. Binmaley, PangasinanroseNo ratings yet
- Art Competition GuidelinesDocument5 pagesArt Competition Guidelinesmarie chanNo ratings yet
- Grade 11 ABM and STEM ExamDocument9 pagesGrade 11 ABM and STEM ExamkeyedNo ratings yet
- EfhfghgDocument1 pageEfhfghgSora100% (1)
- Alumni Membership FormDocument1 pageAlumni Membership FormAsjad JamshedNo ratings yet
- Lani Scholarship Application FormDocument2 pagesLani Scholarship Application FormKrisherica PelleteroNo ratings yet
- Color Fun Run ConsentDocument2 pagesColor Fun Run ConsentLeslie Joy YataNo ratings yet
- 10.2 Null-Alternative Hypothesis WSDocument2 pages10.2 Null-Alternative Hypothesis WSFidya GumilarNo ratings yet
- Sari Sari Store InventoryDocument122 pagesSari Sari Store InventoryLilybeth AseritNo ratings yet
- Notre Dame of Trece Martires: Tel. No 046-4192484Document1 pageNotre Dame of Trece Martires: Tel. No 046-4192484Irene Dulay100% (3)
- PGCHS Adopt a Barangay ProgramDocument6 pagesPGCHS Adopt a Barangay Programrichele valenciaNo ratings yet
- Medical Certificate 2010 PalaroDocument4 pagesMedical Certificate 2010 Palarogeard27No ratings yet
- Medical Certificate 2010 Palaro 1Document1 pageMedical Certificate 2010 Palaro 1Anbu Clint Jarantilla MonsantoNo ratings yet
- TUPC Admission Test ApplicationDocument2 pagesTUPC Admission Test ApplicationSherwin Cuento100% (6)
- Situation AnalysisDocument8 pagesSituation AnalysisKeena Joy Awisan - Pinas100% (1)
- SALN Form 2015-FillableDocument2 pagesSALN Form 2015-Fillableleur_ecks100% (5)
- Kultura at Tradisyon NG Mga IgorotDocument8 pagesKultura at Tradisyon NG Mga IgorotMelanie Joy QuiambaoNo ratings yet
- Survey Questionnaire For Parental Attachment and AutonomyDocument1 pageSurvey Questionnaire For Parental Attachment and AutonomyPhoebe BartNo ratings yet
- Template For Grade 8 Modulo ArtDocument2 pagesTemplate For Grade 8 Modulo ArtVisitacion Hannah Mae AquinoNo ratings yet
- R E N E W A L F O R M: "Tulong Pang-Edukasyon para Sa Bulakenyo"Document2 pagesR E N E W A L F O R M: "Tulong Pang-Edukasyon para Sa Bulakenyo"T VinassaurNo ratings yet
- Sample CV Format For ResearchDocument3 pagesSample CV Format For ResearchCarbelyn BarteNo ratings yet
- LeizmeritzJabonita - CARIBBEAN Reaction Paper COOPDocument2 pagesLeizmeritzJabonita - CARIBBEAN Reaction Paper COOPno no100% (2)
- Annex C Authority To Transfer Accountability For Schools HeadsDocument1 pageAnnex C Authority To Transfer Accountability For Schools HeadsRichelle PascorNo ratings yet
- Individual Dental Health RecordDocument2 pagesIndividual Dental Health RecordCes ReyesNo ratings yet
- Philippine Folk Dance History PDFDocument2 pagesPhilippine Folk Dance History PDFJohn Paul Ta Pham80% (5)
- Flipbook RubricDocument1 pageFlipbook Rubricsewai79100% (3)
- Bench YellDocument2 pagesBench YellMaria Cristina LandinginNo ratings yet
- Scholarship Form (Iskolar Ni Gob)Document1 pageScholarship Form (Iskolar Ni Gob)cedricXXXNo ratings yet
- Lesson 25 Advocacy Campaign ForDocument22 pagesLesson 25 Advocacy Campaign ForJade Pascual0% (1)
- NCAE Type Exam - 2010-2011Document3 pagesNCAE Type Exam - 2010-2011Joseph Cloyd L. Lamberte69% (16)
- Sin Kinasiged, KinasantomDocument5 pagesSin Kinasiged, KinasantomELVIE100% (1)
- Application Form For PCET For SY 2023-2024Document1 pageApplication Form For PCET For SY 2023-2024Faye EbuenNo ratings yet
- English 5-Q4-L6 ModuleDocument15 pagesEnglish 5-Q4-L6 ModuleElaine Joyce Garcia100% (1)
- Cebu Normal University: College Online Applicant Profile SheetDocument1 pageCebu Normal University: College Online Applicant Profile SheetKyllua Theoty Entendez DesolocNo ratings yet
- Chapter TestmeasureofvariationDocument7 pagesChapter Testmeasureofvariationedniel maratasNo ratings yet
- Grade 5 q1 Math Las 1Document1 pageGrade 5 q1 Math Las 1Gene0813No ratings yet
- Eyes Nose Ears Skin TongueDocument18 pagesEyes Nose Ears Skin TongueAngelica BananiaNo ratings yet
- Extremely Satisfied - Moderately SatiesfiedDocument2 pagesExtremely Satisfied - Moderately SatiesfiedThunlynnshein Berjamin0% (2)
- K To 12 Graduates: Pursuing Dreams and Fostering Resilience in The Face of AdversityDocument1 pageK To 12 Graduates: Pursuing Dreams and Fostering Resilience in The Face of AdversityQueen SabarezaNo ratings yet
- NASWEIDocument8 pagesNASWEIRoldan CarpisanoNo ratings yet
- Activity 2 Tools of AstronomyDocument5 pagesActivity 2 Tools of AstronomyWeljun Gallardo100% (1)
- 1-MA Energy ResourcesDocument8 pages1-MA Energy Resources09joaquin.arcasNo ratings yet
- Annex C Application Form and Checklist of RequirementsDocument4 pagesAnnex C Application Form and Checklist of RequirementsEdz BossNo ratings yet
- OB Endorsement Format CS FINALDocument4 pagesOB Endorsement Format CS FINALvannieloveNo ratings yet
- Gwyn Research Chap 1Document43 pagesGwyn Research Chap 1Paulo Justin Tabangcora OropillaNo ratings yet
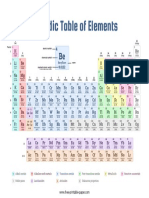
- Periodic Table Color CodedDocument1 pagePeriodic Table Color CodedETHAN HENG ZENG AN MoeNo ratings yet
- Img20230108 09075012Document1 pageImg20230108 09075012Paulo Justin Tabangcora OropillaNo ratings yet
- LeadershipbDocument27 pagesLeadershipbPaulo Justin Tabangcora OropillaNo ratings yet
- Soco Investigation On Ballistics Examination: Group 1Document12 pagesSoco Investigation On Ballistics Examination: Group 1Paulo Justin Tabangcora OropillaNo ratings yet
- Lecture On EvidenceDocument85 pagesLecture On EvidencePaulo Justin Tabangcora OropillaNo ratings yet
- Grade 5 DLP Q3 English Part 5Document6 pagesGrade 5 DLP Q3 English Part 5LEONARDO JR ENRIQUEZNo ratings yet
- Pre Board CJURIS 1 PROF RONIE SABINODocument18 pagesPre Board CJURIS 1 PROF RONIE SABINOPaulo Justin Tabangcora OropillaNo ratings yet
- Orca Share Media1679585095874 7044690485968676549Document1 pageOrca Share Media1679585095874 7044690485968676549Paulo Justin Tabangcora OropillaNo ratings yet
- Major Classification Fingerprint ActivityDocument1 pageMajor Classification Fingerprint ActivityPaulo Justin Tabangcora OropillaNo ratings yet
- Draw The Following Methods of Crime Scene Search: Name: Year and Set: Cdi ActivityDocument3 pagesDraw The Following Methods of Crime Scene Search: Name: Year and Set: Cdi ActivityPaulo Justin Tabangcora OropillaNo ratings yet
- Joint Affidavit of ArrestDocument2 pagesJoint Affidavit of ArrestPaulo Justin Tabangcora OropillaNo ratings yet
- Img20230108 08241894Document1 pageImg20230108 08241894Paulo Justin Tabangcora OropillaNo ratings yet
- Forensic 2 Activity 9Document2 pagesForensic 2 Activity 9Paulo Justin Tabangcora OropillaNo ratings yet
- Dental ExamDocument25 pagesDental ExamPaulo Justin Tabangcora OropillaNo ratings yet
- Criminal Profiling 1Document18 pagesCriminal Profiling 1Paulo Justin Tabangcora OropillaNo ratings yet
- Antimony: A Metal Used in Grid Battery StorageDocument1 pageAntimony: A Metal Used in Grid Battery StoragePaulo Justin Tabangcora OropillaNo ratings yet
- Science 5Document1 pageScience 5Paulo Justin Tabangcora OropillaNo ratings yet
- Itr (A4 Band)Document1 pageItr (A4 Band)Paulo Justin Tabangcora OropillaNo ratings yet
- Nerve Cells 2Document22 pagesNerve Cells 2Paulo Justin Tabangcora OropillaNo ratings yet
- Handwriting AnalysisDocument15 pagesHandwriting AnalysisPaulo Justin Tabangcora OropillaNo ratings yet
- Science 4Document1 pageScience 4Paulo Justin Tabangcora OropillaNo ratings yet
- PhotoscapeDocument1 pagePhotoscapePaulo Justin Tabangcora OropillaNo ratings yet
- MallorcadsadsadDocument2 pagesMallorcadsadsadPaulo Justin Tabangcora OropillaNo ratings yet
- Pre Board CJURISDocument15 pagesPre Board CJURISAlemar Emiliano100% (1)
- Modus OperandiDocument5 pagesModus OperandiPaulo Justin Tabangcora OropillaNo ratings yet
- TungstenDocument1 pageTungstenPaulo Justin Tabangcora OropillaNo ratings yet
- Science 3Document1 pageScience 3Paulo Justin Tabangcora OropillaNo ratings yet
- CLJ4 ModuleDocument11 pagesCLJ4 ModulePaulo Justin Tabangcora OropillaNo ratings yet
- Mallorca 1Document6 pagesMallorca 1Paulo Justin Tabangcora OropillaNo ratings yet
- School Form 8 SF8 Learners Basic Health Nutritional ReportDocument28 pagesSchool Form 8 SF8 Learners Basic Health Nutritional ReportNeriefe BatoNo ratings yet
- Keto Cycle - Insights For SynthesisDocument44 pagesKeto Cycle - Insights For Synthesisdarko surviveovicNo ratings yet
- Lipsitt Weight Nutrition ObesityDocument13 pagesLipsitt Weight Nutrition ObesityJanwyne NgNo ratings yet
- Nutritional Status RecordDocument10 pagesNutritional Status RecordMary Cris SerratoNo ratings yet
- Alin Popescu Despre Cum Sa SlabestiDocument4 pagesAlin Popescu Despre Cum Sa SlabestiMihaela Banica0% (1)
- BMI Classification WhoDocument1 pageBMI Classification WhoMuhammad AkrimNo ratings yet
- Physical Fitness Test Category 1Document6 pagesPhysical Fitness Test Category 1Kaye Marie SalcedoNo ratings yet
- Ngoaingu24H.Vn 1: Chinh PH C Kì Thi THPT QG Cùng V I Cô Mai Phương T I Website Ngoaingu24h.vn!Document3 pagesNgoaingu24H.Vn 1: Chinh PH C Kì Thi THPT QG Cùng V I Cô Mai Phương T I Website Ngoaingu24h.vn!Mon MonNo ratings yet
- NCM 1o5 NCPDocument2 pagesNCM 1o5 NCPlouise beaNo ratings yet
- Obesity Prevention and ManagementDocument2 pagesObesity Prevention and ManagementElcana OtekiNo ratings yet
- Fitness Training Program: Program Start Date Client's Information Warm-UpDocument2 pagesFitness Training Program: Program Start Date Client's Information Warm-UpSpitfire 721No ratings yet
- Body Mass Index (Bmi) Grade Levels: TotalDocument2 pagesBody Mass Index (Bmi) Grade Levels: TotalCarinaCornelioArnocoNo ratings yet
- Eating and Exercise ActivityDocument3 pagesEating and Exercise Activitywalter jesusNo ratings yet
- BMR 1369.3 BMI: Pengiraan Basal Metabolic Rate (BMR) Bagi PerempuanDocument4 pagesBMR 1369.3 BMI: Pengiraan Basal Metabolic Rate (BMR) Bagi PerempuanIzzati LauNo ratings yet
- Calculations - Lecture 1 - TuesdayDocument15 pagesCalculations - Lecture 1 - TuesdayWania ShahidNo ratings yet
- SBFP Form 1: Master List Beneficiaries For School-Based Feeding Program (SBFP)Document13 pagesSBFP Form 1: Master List Beneficiaries For School-Based Feeding Program (SBFP)Sha SadangsalNo ratings yet
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Document1 pageDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)demmieNo ratings yet
- Biggest Loser Guidelines 4Document7 pagesBiggest Loser Guidelines 4Kuma TamersNo ratings yet
- EDITABLE School Form 8 SF8 Learners Basic Health Nutritional ReportDocument17 pagesEDITABLE School Form 8 SF8 Learners Basic Health Nutritional ReportSherelyn Labrado LucasNo ratings yet
- Growth Charts WHO & IAPDocument63 pagesGrowth Charts WHO & IAPGovindan MayavanNo ratings yet
- Summary 2019Document1 pageSummary 2019Laarni Imo IlaganNo ratings yet
- Master List Beneficiaries For School-Based Feeding Program (SBFP)Document11 pagesMaster List Beneficiaries For School-Based Feeding Program (SBFP)Crystal CallanoNo ratings yet
- Childhood Obesity in The United StatesDocument7 pagesChildhood Obesity in The United Statesapi-356392582No ratings yet
- Importance of Apple DietDocument2 pagesImportance of Apple DietRuqia KhanNo ratings yet
- Tackling Obesity in The Western WorldDocument7 pagesTackling Obesity in The Western WorldLê Hoàng HiệpNo ratings yet
- Name: Kiano E. Santos Section & Schedule: AE-204/9:10a-11:10a M Physical Fitness Test InputDocument5 pagesName: Kiano E. Santos Section & Schedule: AE-204/9:10a-11:10a M Physical Fitness Test InputKiano SantosNo ratings yet
- 2020 Q2 SMEA Report for St. Mary's College of BoronganDocument49 pages2020 Q2 SMEA Report for St. Mary's College of Boronganacademic coordinatorNo ratings yet
- Nutritional Status Report 2012-2013Document3 pagesNutritional Status Report 2012-2013Vanessa Anderson Smith100% (2)
- How Much Should I Weigh For My Height and Age BMI Calculator and ChaDocument1 pageHow Much Should I Weigh For My Height and Age BMI Calculator and Cha'ЂолеМмл'No ratings yet
- KesihatanDocument20 pagesKesihatandalysa100% (1)