You might also like
- Anatomic Reconstruction of The Anterior Cruciate Ligament of The Knee With or Without Reconstruction of The Anterolateral Ligament: A Meta-AnalysisDocument11 pagesAnatomic Reconstruction of The Anterior Cruciate Ligament of The Knee With or Without Reconstruction of The Anterolateral Ligament: A Meta-AnalysisOthoniel RamirezNo ratings yet
- RTR Efectos de La Liberacion Del TorniqueteDocument9 pagesRTR Efectos de La Liberacion Del TorniqueteorthopaedicsUV martNo ratings yet
- Watermark 7Document14 pagesWatermark 7PKM BANGSRI INo ratings yet
- BMAC, MSC For Knee OsteoarthritisDocument11 pagesBMAC, MSC For Knee OsteoarthritisMrinalini SinghNo ratings yet
- Allograft Vs Autograft 2022Document11 pagesAllograft Vs Autograft 2022Ahmed MortadaNo ratings yet
- Bankart VS Tratamiento ConservadorDocument7 pagesBankart VS Tratamiento ConservadorMaría IsabelNo ratings yet
- 1 s2.0 S0883540320304605 MainDocument4 pages1 s2.0 S0883540320304605 MainSavNo ratings yet
- Clinical Outcomes and Osteoarthritis at Very Long-Term Follow-Up After ACL ReconstructionDocument13 pagesClinical Outcomes and Osteoarthritis at Very Long-Term Follow-Up After ACL ReconstructionrandocalNo ratings yet
- Unicompartmental Knee Arthroplasty Vs Total Knee Arthroplasty - 2022 - ArthropDocument6 pagesUnicompartmental Knee Arthroplasty Vs Total Knee Arthroplasty - 2022 - ArthropSanty OktavianiNo ratings yet
- The Impact of The COVID-19 Pandemic On Hip and Knee Arthroplasty: A Systematic ReviewDocument10 pagesThe Impact of The COVID-19 Pandemic On Hip and Knee Arthroplasty: A Systematic ReviewLasa SiahaanNo ratings yet
- UntitledDocument28 pagesUntitledOmar BellachiNo ratings yet
- 1807 5932 Clin 71 02 110 PDFDocument4 pages1807 5932 Clin 71 02 110 PDFkinecamposNo ratings yet
- JCM 10 01853Document16 pagesJCM 10 01853Katrina Mae FajardoNo ratings yet
- Relationship Between Timing of Anterior Cruciate Ligament Reconstruction and Chondral InjuriesDocument12 pagesRelationship Between Timing of Anterior Cruciate Ligament Reconstruction and Chondral InjuriesMaría IsabelNo ratings yet
- Orthobiologic Injections For Treating DegenerativeDocument7 pagesOrthobiologic Injections For Treating DegenerativeNacho TorreroNo ratings yet
- KJP 34 4 487Document14 pagesKJP 34 4 487Abante_gammaNo ratings yet
- Chinese Translation and Validation of The Oxford Knee - 2017 - Hong Kong PhysioDocument4 pagesChinese Translation and Validation of The Oxford Knee - 2017 - Hong Kong PhysioAnuj ShandilyaNo ratings yet
- Reabilitação Após Tratamento Cirúrgico de Rupturas e Rupturas Do Tendão Fibular.Document10 pagesReabilitação Após Tratamento Cirúrgico de Rupturas e Rupturas Do Tendão Fibular.Thiago Penna ChavesNo ratings yet
- 1 s2.0 S0972978X20303822 MainDocument7 pages1 s2.0 S0972978X20303822 MainDita AldiniNo ratings yet
- Journal of Orthopaedics: Dominic T. Mathis, Leif Lohrer, Felix Amsler, Michael T. HirschmannDocument7 pagesJournal of Orthopaedics: Dominic T. Mathis, Leif Lohrer, Felix Amsler, Michael T. HirschmannDita AldiniNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- A Systematic Review and Meta Analysis of Arthroscopic Meniscus Repair in Young Patients: Comparison of All Inside and Inside Out Suture TechniquesDocument11 pagesA Systematic Review and Meta Analysis of Arthroscopic Meniscus Repair in Young Patients: Comparison of All Inside and Inside Out Suture TechniquesJeremyNo ratings yet
- Pelvic BinderDocument9 pagesPelvic BinderLuisNo ratings yet
- Efficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisDocument10 pagesEfficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisChangjing ZhangNo ratings yet
- A Systematic Review of Bracing Following Reconstruction of The ACLDocument10 pagesA Systematic Review of Bracing Following Reconstruction of The ACLDanar AdhimuktiNo ratings yet
- 2015 Article 158Document9 pages2015 Article 158ss huNo ratings yet
- Efficacy of Adductor Canal Block in Total Knee Arthroplasty: A Systematic ReviewDocument10 pagesEfficacy of Adductor Canal Block in Total Knee Arthroplasty: A Systematic ReviewHalim SudonoNo ratings yet
- The Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewDocument7 pagesThe Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewIJAR JOURNALNo ratings yet
- ACL Tibial Fixation MedthodsDocument8 pagesACL Tibial Fixation MedthodsCleff FlowersNo ratings yet
- Ergo - Ergonomics and GI Endoscopy - ASGE2009Document9 pagesErgo - Ergonomics and GI Endoscopy - ASGE2009rodrigocpnovaisNo ratings yet
- Sagittal Condylar Inclination and Transversal Condylar Inclination in Different Skeletal ClassesDocument13 pagesSagittal Condylar Inclination and Transversal Condylar Inclination in Different Skeletal ClassesRicardo AugustoNo ratings yet
- Effective Use of Viscosupplementation After Knee Arthroscopy: Experience From A Working GroupDocument10 pagesEffective Use of Viscosupplementation After Knee Arthroscopy: Experience From A Working GroupIJAR JOURNALNo ratings yet
- Af 75Document13 pagesAf 75Ola ZahraNo ratings yet
- Hook Plate Fixation For Acute Unstable Distal Clavicle Fracture: A Systematic Review and Meta-AnalysisDocument6 pagesHook Plate Fixation For Acute Unstable Distal Clavicle Fracture: A Systematic Review and Meta-AnalysisFillipe AgraNo ratings yet
- 2017 Paravertebral Block en Pediatrics BJADocument8 pages2017 Paravertebral Block en Pediatrics BJAAlejandra SanchezNo ratings yet
- 66 JPR D 20 00262Document10 pages66 JPR D 20 00262snkidNo ratings yet
- 2309499017754106Document9 pages2309499017754106harumNo ratings yet
- Van Midden Dorp 2013Document14 pagesVan Midden Dorp 2013Raveli KalvinNo ratings yet
- (2023) Effects of Running On The Development of Knee OsteoarthritisDocument6 pages(2023) Effects of Running On The Development of Knee Osteoarthritiscalixto1995No ratings yet
- Adjunct Analgesia Reduces Pain and Opioid Consumption After Hip ArthrosDocument14 pagesAdjunct Analgesia Reduces Pain and Opioid Consumption After Hip ArthrosFelipeSanzanaNo ratings yet
- A Scoping Review of The Proximal Humerus Fracture LiteratureDocument10 pagesA Scoping Review of The Proximal Humerus Fracture LiteratureIin Novita SariNo ratings yet
- Treatment Modalities For Hip and Knee Osteoarthritis: A Systematic Review of SafetyDocument12 pagesTreatment Modalities For Hip and Knee Osteoarthritis: A Systematic Review of SafetyIlham RaymanaNo ratings yet
- Comparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture SurgeryDocument12 pagesComparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture Surgeryangelama1783riosNo ratings yet
- Complications and Downsides of The Robotic Total Knee Arthroplasty: A Systematic ReviewDocument15 pagesComplications and Downsides of The Robotic Total Knee Arthroplasty: A Systematic Reviewmamyeu1801No ratings yet
- Rajiv Gandhi University of Health Sciences Bengaluru, Karnataka Proforma For Registration of Subjects For DissertationDocument10 pagesRajiv Gandhi University of Health Sciences Bengaluru, Karnataka Proforma For Registration of Subjects For DissertationRachnaNo ratings yet
- Integrated Review WeeblyDocument10 pagesIntegrated Review Weeblyapi-401390929No ratings yet
- Early Versus Delayed Passive Range of Motion Exercise For Arthroscopic Rotator Cuff RepairDocument9 pagesEarly Versus Delayed Passive Range of Motion Exercise For Arthroscopic Rotator Cuff RepairJane Elisabeth WauranNo ratings yet
- Nakata 2021Document15 pagesNakata 2021FlaviusNo ratings yet
- Comparing Unilateral and Bilateral Total Knee Replacement Based On The Functional ApproachDocument7 pagesComparing Unilateral and Bilateral Total Knee Replacement Based On The Functional ApproachIlham Amal MNo ratings yet
- 1 s2.0 S1015958421001019 MainDocument9 pages1 s2.0 S1015958421001019 MaincderosasNo ratings yet
- Vertical Stability of Different OrthognathicDocument10 pagesVertical Stability of Different OrthognathicRohini TondaNo ratings yet
- Patient-Related Risk Factors Associated With Less Favourable Outcomes Following Hip ArthrosDocument10 pagesPatient-Related Risk Factors Associated With Less Favourable Outcomes Following Hip ArthrosAhmad PradhanaNo ratings yet
- Siman2017 ORTOPEDIADocument6 pagesSiman2017 ORTOPEDIAOrto MespNo ratings yet
- Literature Review Endoscopic Techniques For Spinal Oncology: A SystematicDocument8 pagesLiterature Review Endoscopic Techniques For Spinal Oncology: A SystematicAhana MukherjeeNo ratings yet
- Kraus 2021Document7 pagesKraus 2021翁嘉聰No ratings yet
- Joint Report On Terminology For Surgical Procedures To Treat Pelvic Organ ProlapseDocument35 pagesJoint Report On Terminology For Surgical Procedures To Treat Pelvic Organ ProlapseCarla Dela CruzNo ratings yet
- Biomedicines 12 00705 1Document13 pagesBiomedicines 12 00705 1jamel-shamsNo ratings yet
- Lau 2021Document7 pagesLau 2021Aaron BNo ratings yet
- Evaluación Clínica y Funcional Del HombroDocument9 pagesEvaluación Clínica y Funcional Del HombroLuis Eduardo Cabezas MirandaNo ratings yet
- End of Life and DementiaDocument5 pagesEnd of Life and DementiaBlaize JonesNo ratings yet
- Math Practice Problems Group 3Document2 pagesMath Practice Problems Group 3Lukman Nal 26No ratings yet
- HLFM - Li Xuan ClaraDocument54 pagesHLFM - Li Xuan ClaraClara LiNo ratings yet
- hw320 Unit 9 Final Project Lisa Tulka Deroche hw499 Unit 5 AssignmnetDocument15 pageshw320 Unit 9 Final Project Lisa Tulka Deroche hw499 Unit 5 Assignmnetapi-687900322No ratings yet
- Plastic Surgery Logbook Batch A - EditedDocument11 pagesPlastic Surgery Logbook Batch A - EditedRidham RanaNo ratings yet
- Use Case Diagram:: AdminDocument8 pagesUse Case Diagram:: AdminnehadhamechaNo ratings yet
- 200808end of Life CareDocument77 pages200808end of Life CarePaijo SusenoNo ratings yet
- DR Anum Junaid: ObjectiveDocument2 pagesDR Anum Junaid: ObjectiveMisbhasaeedaNo ratings yet
- Peds ?Document51 pagesPeds ?gissy0522No ratings yet
- Report of Medicare Multispeciality Hospital and Trauma CentreDocument5 pagesReport of Medicare Multispeciality Hospital and Trauma CentremuskanNo ratings yet
- Phrma Seniority List 01Document38 pagesPhrma Seniority List 01vasan980100% (1)
- Feasibility StudyDocument27 pagesFeasibility Studyapi-297065332100% (2)
- Effectiveness of Breast Massage On Expression of Breast Milk Among Mothers of Neonates Admitted in Neonatal Intensive Care UnitDocument5 pagesEffectiveness of Breast Massage On Expression of Breast Milk Among Mothers of Neonates Admitted in Neonatal Intensive Care UnitMuhammad SawalNo ratings yet
- Daftar ObatDocument3 pagesDaftar ObatKlinik Darul FalahNo ratings yet
- Philhealth Pre-Auth CataractDocument6 pagesPhilhealth Pre-Auth Cataractwmarasigan2610No ratings yet
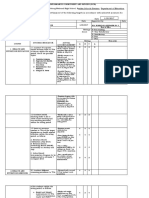
- Rubrics NCP NCM 103 SL Funda VSDocument1 pageRubrics NCP NCM 103 SL Funda VSJohn TacordaJrNo ratings yet
- Tamiflu PDFDocument28 pagesTamiflu PDFSopheak NGNo ratings yet
- The Michigan Nursing Home Abuse and Neglect HandbookDocument58 pagesThe Michigan Nursing Home Abuse and Neglect HandbookBuckfire & Buckfire PCNo ratings yet
- Pediatrics Objective Type Questions and Answers - All Medical Questions and AnswersDocument4 pagesPediatrics Objective Type Questions and Answers - All Medical Questions and AnswersAbdul Ghaffar AbdullahNo ratings yet
- Oet Speakingr PDFDocument133 pagesOet Speakingr PDFAlphonsa Thomas100% (1)
- A Bridge To Self Healing - Philippine Institute of Naturopathic Sciences (PINS) LaunchedDocument8 pagesA Bridge To Self Healing - Philippine Institute of Naturopathic Sciences (PINS) LaunchedAre Pee EtcNo ratings yet
- Manual Medical Records NabhDocument21 pagesManual Medical Records NabhSadaf SadafNo ratings yet
- Pharma - Week 2 (Introduction)Document2 pagesPharma - Week 2 (Introduction)MIKAELA DAVIDNo ratings yet
- Special Leave Benefits For Women PDFDocument2 pagesSpecial Leave Benefits For Women PDFJoan CarigaNo ratings yet
- Mba HR (Employee Motivation)Document68 pagesMba HR (Employee Motivation)Om PrakashNo ratings yet
- TMF HospitalDocument1 pageTMF Hospitalsurya syndicateNo ratings yet
- Jen Ipcr 1st QuarterDocument4 pagesJen Ipcr 1st QuarterJairolla ObayNo ratings yet
- A Case Report On Benign Prostatic Hyperplasia With Homeopathic RemediesDocument6 pagesA Case Report On Benign Prostatic Hyperplasia With Homeopathic RemediesBaru Chandrasekhar RaoNo ratings yet
- PRE OP ChecklistDocument1 pagePRE OP ChecklistDR.No ratings yet
- Outsourcing Security Case StudyDocument13 pagesOutsourcing Security Case StudyismakieNo ratings yet