You might also like
- The Stress-Free Guide to Parenting a Child With ADHD: Effective and Proven Strategies for Alleviating Anxiety and Forming Strong Bonds Without the HassleFrom EverandThe Stress-Free Guide to Parenting a Child With ADHD: Effective and Proven Strategies for Alleviating Anxiety and Forming Strong Bonds Without the HassleNo ratings yet
- Motor Claim Form DetailsDocument6 pagesMotor Claim Form Detailsabhishek mishraNo ratings yet
- Hacking for Beginners: Comprehensive Guide on Hacking Websites, Smartphones, Wireless Networks, Conducting Social Engineering, Performing a Penetration Test, and Securing Your Network (2022)From EverandHacking for Beginners: Comprehensive Guide on Hacking Websites, Smartphones, Wireless Networks, Conducting Social Engineering, Performing a Penetration Test, and Securing Your Network (2022)No ratings yet
- PL FormDocument1 pagePL FormAnonymous F0AqjkNo ratings yet
- Motor Claim Form DetailsDocument5 pagesMotor Claim Form DetailsRandy OrtonNo ratings yet
- Motor Trade (Road Risks) Insurance Policy Claim FormDocument5 pagesMotor Trade (Road Risks) Insurance Policy Claim FormphilipjohnlunaNo ratings yet
- Completete SET OF HR FORMSDocument9 pagesCompletete SET OF HR FORMSALEXANDER DIMAFELIX JR.No ratings yet
- Application FormDocument2 pagesApplication FormJuan LucioNo ratings yet
- GZU Postgraduate Application FormDocument6 pagesGZU Postgraduate Application FormRamin Le MiexNo ratings yet
- Sample PlanDocument7 pagesSample Planapi-3801982100% (1)
- Application For Program EntryDocument6 pagesApplication For Program EntryAngela FrizellNo ratings yet
- Supplier QuestionnaireDocument4 pagesSupplier QuestionnairedorisNo ratings yet
- SEED Application FormDocument4 pagesSEED Application FormTeasha Nika PetersNo ratings yet
- FORM ACCIDENT - English ImperialDocument2 pagesFORM ACCIDENT - English ImperialJose E RafolsNo ratings yet
- Application For Overhead/Hoist Crane Installation: Department of Labor and EmploymentDocument1 pageApplication For Overhead/Hoist Crane Installation: Department of Labor and EmploymentErika Cadawan100% (1)
- OTGCI Truckers Accreditation Form 2019 PDFDocument3 pagesOTGCI Truckers Accreditation Form 2019 PDFOmar FrianezaNo ratings yet
- Franchise Application Form 2021Document8 pagesFranchise Application Form 2021Jean Lois Condeza GelmoNo ratings yet
- IIETM Application FormDocument8 pagesIIETM Application FormPaarNo ratings yet
- Record of Employment and Security Declaration Form: Attach PhotoDocument3 pagesRecord of Employment and Security Declaration Form: Attach PhotoleoosteauaNo ratings yet
- Philsteel Holdings Corp.: Philsteel Tower, 140 Amorsolo ST., Legaspi Village Makati CityDocument2 pagesPhilsteel Holdings Corp.: Philsteel Tower, 140 Amorsolo ST., Legaspi Village Makati CityShainaNo ratings yet
- Intake SheetDocument2 pagesIntake SheetMole san zeravlaNo ratings yet
- AEP Application FormDocument2 pagesAEP Application FormRenadelyn GombaNo ratings yet
- Form Employment TerminationDocument2 pagesForm Employment TerminationMark VeederNo ratings yet
- Personnel Information Sheet (New) PDFDocument5 pagesPersonnel Information Sheet (New) PDFLoo PeaNo ratings yet
- 002-Recruitment Requisition Form - Rev - 01Document1 page002-Recruitment Requisition Form - Rev - 01ARIF WINARDINo ratings yet
- Labor Certification WorksheetDocument7 pagesLabor Certification WorksheetJoyxfulNo ratings yet
- Installation Floater: Applicant InformationDocument2 pagesInstallation Floater: Applicant InformationAra AgopianNo ratings yet
- Biodata Revised As of 11.5.18Document1 pageBiodata Revised As of 11.5.18S3 INSURANCENo ratings yet
- SSSI ApplicationFormForEmployment-V3.0 1633574829Document2 pagesSSSI ApplicationFormForEmployment-V3.0 1633574829renierarong18No ratings yet
- Bond Application-CorporationDocument5 pagesBond Application-CorporationDaniel BuenafeNo ratings yet
- Bond Application CorporationDocument3 pagesBond Application Corporationdataprotection.puicNo ratings yet
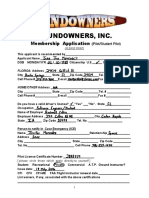
- Sundowner Pilot Application 2009Document2 pagesSundowner Pilot Application 2009Juan Jose MenendezNo ratings yet
- Corporate Questionnaire Farrugia & PartnersDocument9 pagesCorporate Questionnaire Farrugia & Partnerstrevorcity84No ratings yet
- Division of Graduate Medical Studies: Yong Loo Lin School of MedicineDocument5 pagesDivision of Graduate Medical Studies: Yong Loo Lin School of MedicinebloresamNo ratings yet
- DepEd Leave Application FormDocument2 pagesDepEd Leave Application FormJinn Dalisay Uy100% (3)
- Accident Investigation Report Form 1Document5 pagesAccident Investigation Report Form 1Mamun MahmudNo ratings yet
- Report On Health and Safety OrganizationDocument1 pageReport On Health and Safety OrganizationjasbalisacanNo ratings yet
- Application For Employment For Office Use OnlyDocument9 pagesApplication For Employment For Office Use OnlyMr. PicklesNo ratings yet
- Applicant Application FormDocument6 pagesApplicant Application FormJocelyn Joy ArcegaNo ratings yet
- Liability Claim FormDocument6 pagesLiability Claim FormHihiNo ratings yet
- Application For Employment BhfruralbankDocument3 pagesApplication For Employment BhfruralbankVivianAlcantaraDelaCruzNo ratings yet
- BOND APPLICATION INDIVIDUAL. Heirs BondDocument5 pagesBOND APPLICATION INDIVIDUAL. Heirs BondAnonymous 4nbk4yr100% (1)
- Undergraduate Application Form-23022022Document2 pagesUndergraduate Application Form-23022022bongisebodgeNo ratings yet
- Motor Claim Form THE ORIENTAL INSURANCE CO. LTD.Document4 pagesMotor Claim Form THE ORIENTAL INSURANCE CO. LTD.rajiv.surveyor7145No ratings yet
- Application For Games of Chance License, Bell Jar, Raffles Over 30,000 (GC-2, GC-2A, GC-2B)Document6 pagesApplication For Games of Chance License, Bell Jar, Raffles Over 30,000 (GC-2, GC-2A, GC-2B)Jacob GiffenNo ratings yet
- clearanceFormDocument3 pagesclearanceFormArvin BegasoNo ratings yet
- Insurance Agent Exam ApplicationDocument1 pageInsurance Agent Exam ApplicationBryan MagnayeNo ratings yet
- Supplier Accreditation Requirements MaterialDocument6 pagesSupplier Accreditation Requirements MaterialFred Vincent BaldomeroNo ratings yet
- Landero Clinic and Hospital: Notice of ChargeDocument1 pageLandero Clinic and Hospital: Notice of ChargeQuennie Marie Moreno VillanuevaNo ratings yet
- Work Experience Certification For Journeyman PlumberDocument2 pagesWork Experience Certification For Journeyman Plumberabood30513No ratings yet
- Important Notice: Florida Marine Transporters, Inc. PBC Management, IncDocument7 pagesImportant Notice: Florida Marine Transporters, Inc. PBC Management, Inccaneman85No ratings yet
- New Account Data SheetDocument1 pageNew Account Data SheetpicfixerNo ratings yet
- R.A. 7042 Interview SheetDocument2 pagesR.A. 7042 Interview SheetLenin Rey PolonNo ratings yet
- Application Form For Business LicenseDocument3 pagesApplication Form For Business LicenseberhanNo ratings yet
- EC Grievance Intake FormDocument1 pageEC Grievance Intake FormJelyn BujatinNo ratings yet
- Eskayvie Application Form - 230227 - 163219Document4 pagesEskayvie Application Form - 230227 - 163219boymk5797No ratings yet
- BAI-AHWD Form No. 1 FinalDocument2 pagesBAI-AHWD Form No. 1 FinalBrillantes JY100% (2)
- Es2620 Adobe11 PDFDocument2 pagesEs2620 Adobe11 PDFAnonymous anuhHTNo ratings yet
- Employee Information Sheet: Joining ReportDocument8 pagesEmployee Information Sheet: Joining ReportAhmad FeisalNo ratings yet
- Application To Rent GL FormDocument2 pagesApplication To Rent GL Formgeorgelange100% (2)
- BEDA - CaseZ-Doctrines-InsuranceDocument5 pagesBEDA - CaseZ-Doctrines-InsuranceMalcolm CruzNo ratings yet
- Private Motor 4 Wheeler: Customer - Care@sbigeneral - inDocument12 pagesPrivate Motor 4 Wheeler: Customer - Care@sbigeneral - inpooran singh chaudharyNo ratings yet
- Philam Insurance Co., Inc. v. Parc Chateau Condominium Unit Owners G.R. No. 201116Document3 pagesPhilam Insurance Co., Inc. v. Parc Chateau Condominium Unit Owners G.R. No. 201116abbywinsterNo ratings yet
- Private Car Comprehensive Policy: Certificate of Insurance Cum Policy ScheduleDocument4 pagesPrivate Car Comprehensive Policy: Certificate of Insurance Cum Policy Scheduleaakashgupta viaanshNo ratings yet
- Subrogation: The Insurance Involved Is Property Insurance 1Document3 pagesSubrogation: The Insurance Involved Is Property Insurance 1Esto, Cassandra Jill SumalbagNo ratings yet
- D096673877 7117287603297891 SchedulescDocument3 pagesD096673877 7117287603297891 SchedulescrakeshNo ratings yet
- Jaime TDocument3 pagesJaime TJune Karl CepidaNo ratings yet
- Win24_1D_Insurance_Pension_MrunalDocument22 pagesWin24_1D_Insurance_Pension_Mrunalanjan sahanaNo ratings yet
- PruLife Your TermDocument3 pagesPruLife Your TermDavrans GPNo ratings yet
- Tlscontact Visa Application Centre - Kiev List of Documents Medical TreatmentDocument3 pagesTlscontact Visa Application Centre - Kiev List of Documents Medical TreatmentMikeNo ratings yet
- Bajaj Finserv's Role in Consumer Finance and Customer PerceptionDocument58 pagesBajaj Finserv's Role in Consumer Finance and Customer PerceptionPramod KumarNo ratings yet
- AidsDocument9 pagesAidsKhushi GuptaNo ratings yet
- Certificate of Insurance: Inbound TravelDocument1 pageCertificate of Insurance: Inbound TravelAmanuel AsmareNo ratings yet
- In His Analysis of California S Proposition 103 See Illustration 4 2Document1 pageIn His Analysis of California S Proposition 103 See Illustration 4 2trilocksp SinghNo ratings yet
- Financial Market and Services Bba 2 Notes 1Document18 pagesFinancial Market and Services Bba 2 Notes 1Sneha AroraNo ratings yet
- TRAVEL INSURANCE COVER FOR ACCIDENTSDocument1 pageTRAVEL INSURANCE COVER FOR ACCIDENTSWan IkhwanNo ratings yet
- 4168 O-Tmcas 298685235 00 000Document8 pages4168 O-Tmcas 298685235 00 000insurancekatariaNo ratings yet
- RAKESHDocument3 pagesRAKESHRakesh GuptaNo ratings yet
- Insurance and Risk Management R6Y2dFBRs5Document290 pagesInsurance and Risk Management R6Y2dFBRs5jahnvi shahNo ratings yet
- Matching Principle Concept - AccountingDocument1 pageMatching Principle Concept - AccountingClauie BarsNo ratings yet
- InsurDocument1 pageInsurlegacyinternetcafe1No ratings yet
- Prudential SurrenderDocument5 pagesPrudential SurrenderBriltex IndustriesNo ratings yet
- Cashless Authorization Letter (Part-D)Document4 pagesCashless Authorization Letter (Part-D)AkhilNo ratings yet
- W4-Module Income Tax On CorporationDocument18 pagesW4-Module Income Tax On CorporationDanica VetuzNo ratings yet
- (Modified) IdentificationDocument4 pages(Modified) IdentificationKlarish Jay BeguinaNo ratings yet
- Blue Cross Healthcare Inc. v. OlivaresDocument2 pagesBlue Cross Healthcare Inc. v. OlivaresJUAN REINO CABITACNo ratings yet
- 1.contract Ii (Contracts of Guarantee An Analysis)Document11 pages1.contract Ii (Contracts of Guarantee An Analysis)Palak ThakrarNo ratings yet
- AINS 23 - Commercial Insurance NotesDocument52 pagesAINS 23 - Commercial Insurance Notesvijaijohn100% (1)
- Billing Definations 7Document15 pagesBilling Definations 7Saeed ahmed100% (1)
- International Students Paperwork Guide For Foreign Bureaucratic AffairsDocument8 pagesInternational Students Paperwork Guide For Foreign Bureaucratic AffairsJoana Laus CamposNo ratings yet