You might also like
- IC Pembersihan Karang Gigi (Scaling) in EnglishDocument3 pagesIC Pembersihan Karang Gigi (Scaling) in EnglishmarcelloNo ratings yet
- IC Perawatan Bleaching in EnglishDocument4 pagesIC Perawatan Bleaching in EnglishmarcelloNo ratings yet
- IC Perawatan Implan in EnglishDocument4 pagesIC Perawatan Implan in EnglishmarcelloNo ratings yet
- IC Perawatan Syaraf Gigi (Endo) in EnglishDocument4 pagesIC Perawatan Syaraf Gigi (Endo) in EnglishmarcelloNo ratings yet
- EthicsDocument54 pagesEthicsMehek BatraNo ratings yet
- Informed Refusal Periodontal TreatmentDocument2 pagesInformed Refusal Periodontal TreatmentintaninfNo ratings yet
- Health HistoryDocument4 pagesHealth Historyapi-2220825740% (1)
- Dental consent form for minorsDocument2 pagesDental consent form for minorsJanNo ratings yet
- Informed ConsentDocument7 pagesInformed Consentdrpooja.kaloniyaNo ratings yet
- Consent Cosmetic TreatmentDocument2 pagesConsent Cosmetic Treatmentd. g.No ratings yet
- Clinic New Case HistoryDocument5 pagesClinic New Case HistoryRashmin ShahNo ratings yet
- Tonsillectomy Adenoidectomy ConsentDocument4 pagesTonsillectomy Adenoidectomy ConsentMohitNo ratings yet
- Sty ConsentDocument3 pagesSty ConsentNitin SharmaNo ratings yet
- Informed Consent For Closed Reduction of Nasal FractureDocument3 pagesInformed Consent For Closed Reduction of Nasal FractureWalter J. Florez-GuerraNo ratings yet
- Endoscopic Sinus Surgery ConsentDocument3 pagesEndoscopic Sinus Surgery ConsentNitin SharmaNo ratings yet
- 4 UJMDS 1340 RVDocument4 pages4 UJMDS 1340 RVNugraha AnggaNo ratings yet
- Consent Form For Telemedicine ConsultationDocument3 pagesConsent Form For Telemedicine ConsultationAdmin dahsNo ratings yet
- English Patient History NewDocument13 pagesEnglish Patient History NewPRAKASSH RNo ratings yet
- How to diagnose oral pain with a patient historyDocument6 pagesHow to diagnose oral pain with a patient historyMedoxNo ratings yet
- Patient and Family Rights and ResponsibilitiesDocument5 pagesPatient and Family Rights and Responsibilitiesnabh2019 inuNo ratings yet
- Consent Form For Tele-ConsultationDocument3 pagesConsent Form For Tele-ConsultationAdmin dahs100% (1)
- Dentistry-Informed Consent For Periodontal Treatment-MedPro GroupDocument2 pagesDentistry-Informed Consent For Periodontal Treatment-MedPro Groupednrg123No ratings yet
- Dental Consent FormDocument16 pagesDental Consent FormArnav Gupta100% (1)
- Telemedicine Consent FormDocument2 pagesTelemedicine Consent FormNICHAEL MARIA CELINA UYNo ratings yet
- Extraction Consent: Parkside Family Dental Informed Consent Tooth RemovalDocument14 pagesExtraction Consent: Parkside Family Dental Informed Consent Tooth Removalraymundo.ledfNo ratings yet
- Dental Medical Clearance Form SampleDocument1 pageDental Medical Clearance Form SampleTe Amo GuidNo ratings yet
- Dentistry-Informed Consent For Endodontic Procedures-MedPro GroupDocument2 pagesDentistry-Informed Consent For Endodontic Procedures-MedPro Groupednrg123No ratings yet
- Dentistry-Informed Consent For Orthodontic Treatment-MedPro GroupDocument3 pagesDentistry-Informed Consent For Orthodontic Treatment-MedPro Groupednrg123No ratings yet
- MEDICARE CLAIM FORMDocument2 pagesMEDICARE CLAIM FORMtagashiiNo ratings yet
- Consent For Tooth ExtractionDocument3 pagesConsent For Tooth ExtractionCommunity-based Health Program San Jose100% (1)
- General Consent For Dental TreatmentDocument1 pageGeneral Consent For Dental TreatmentSreekanth KrishnamurthyNo ratings yet
- Dentalconsent-Vizilite 0001Document4 pagesDentalconsent-Vizilite 0001Orlando GesualdoNo ratings yet
- Surat Keterangan Dokter - Doctor'S Report Penyakit Kanker - CancerDocument5 pagesSurat Keterangan Dokter - Doctor'S Report Penyakit Kanker - CancerUlinnoha FarrasNo ratings yet
- Nursing Admission FormDocument6 pagesNursing Admission FormErdin TriansyahNo ratings yet
- BHJ Online Consent 2021Document3 pagesBHJ Online Consent 2021Sherryl SarmientoNo ratings yet
- Informed Consent and Informed Refusal in Dentistry: by Dianne Glasscoe Watterson, RDH, BS, MbaDocument10 pagesInformed Consent and Informed Refusal in Dentistry: by Dianne Glasscoe Watterson, RDH, BS, MbaSanniie NuansaNo ratings yet
- Consent Form Pediatric Dental TreatmentDocument2 pagesConsent Form Pediatric Dental TreatmentthraldorNo ratings yet
- Informed Consent Form For Telerehabilitation Consultation: English VersionDocument3 pagesInformed Consent Form For Telerehabilitation Consultation: English VersionSergel Marco AgnoNo ratings yet
- New Patient FormDocument4 pagesNew Patient Formapi-288684181No ratings yet
- Patient Information FormDocument6 pagesPatient Information FormKimCriglerNo ratings yet
- New Patient Medical History FormDocument2 pagesNew Patient Medical History Form2oclockNo ratings yet
- Child and Family Therapy Intake PacketDocument14 pagesChild and Family Therapy Intake PacketIvanNo ratings yet
- AppForm - GroupMedIns - Member - 2016-06 (June14)Document3 pagesAppForm - GroupMedIns - Member - 2016-06 (June14)Ruchie EtolleNo ratings yet
- Rielle Bioethics AssDocument7 pagesRielle Bioethics Assdrae syNo ratings yet
- Welcome Rev2Document2 pagesWelcome Rev2Adam C. Price100% (1)
- Statement of Claim Form (OP IP CLAIM) (Hospitalization)Document1 pageStatement of Claim Form (OP IP CLAIM) (Hospitalization)Dreyfus MicianoNo ratings yet
- Mami Che's Ear Piercing ConsentDocument2 pagesMami Che's Ear Piercing ConsentDarlNo ratings yet
- Payment Policies and Agreement To PayDocument5 pagesPayment Policies and Agreement To PayChristopher HartmanNo ratings yet
- Informed Consent Form For General Dental Procedures2Document3 pagesInformed Consent Form For General Dental Procedures2SkAliHassanNo ratings yet
- SKD Death Claim English Ver. 01Document1 pageSKD Death Claim English Ver. 01velandoNo ratings yet
- Informed Consent For Treatment: What Is It? Howdoidoit?Document2 pagesInformed Consent For Treatment: What Is It? Howdoidoit?ISForeverNo ratings yet
- Fractional CO2Document4 pagesFractional CO2Rahul PillaiNo ratings yet
- Informed Consent For Laser DepigmentationDocument1 pageInformed Consent For Laser DepigmentationEking InNo ratings yet
- General ConsentDocument2 pagesGeneral ConsentdesyNo ratings yet
- Periodontal Care Plan - Thai HoangDocument21 pagesPeriodontal Care Plan - Thai Hoangapi-643588876No ratings yet
- DP New Patient Form - 2023Document5 pagesDP New Patient Form - 2023cdbn2326No ratings yet
- Maybe Not For Me: Ethics in OrthodonticsDocument1 pageMaybe Not For Me: Ethics in OrthodonticsDominikaSkórkaNo ratings yet
- Taking Charge of Your Health Care Activity and QuestionsDocument3 pagesTaking Charge of Your Health Care Activity and QuestionsIvan Miguel Cabrera QuezadaNo ratings yet
- AlternatorDocument3 pagesAlternatorVatsal PatelNo ratings yet
- Malabsorption and Elimination DisordersDocument120 pagesMalabsorption and Elimination DisordersBeBs jai SelasorNo ratings yet
- Design and Analysis of Buck ConverterDocument18 pagesDesign and Analysis of Buck Converterk rajendraNo ratings yet
- DOJ OIG Issues 'Fast and Furious' ReportDocument512 pagesDOJ OIG Issues 'Fast and Furious' ReportFoxNewsInsiderNo ratings yet
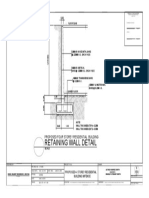
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- ASIA IVALUE Business ProfileDocument9 pagesASIA IVALUE Business ProfileDidiek PriambudiNo ratings yet
- FIL M 216 2nd Yer Panitikan NG PilipinasDocument10 pagesFIL M 216 2nd Yer Panitikan NG PilipinasJunas LopezNo ratings yet
- CBK Test QuestionsDocument2 pagesCBK Test QuestionsMehul GuptaNo ratings yet
- Ginglen 2022 - Necrotizing Enterocolitis - StatPearlsDocument8 pagesGinglen 2022 - Necrotizing Enterocolitis - StatPearlsBee GuyNo ratings yet
- EBSD Specimen Prep PaperDocument36 pagesEBSD Specimen Prep PaperPaul RosiahNo ratings yet
- G7-UNIT - I. (Module - 1 (Week 1 - 3 (Microscopy & Levels of Org.)Document8 pagesG7-UNIT - I. (Module - 1 (Week 1 - 3 (Microscopy & Levels of Org.)Margie Gabo Janoras - DaitolNo ratings yet
- INSYS - EBW Serie EbookDocument4 pagesINSYS - EBW Serie EbookJorge_Andril_5370No ratings yet
- Unit Rates and Cost Per ItemDocument213 pagesUnit Rates and Cost Per ItemDesiree Vera GrauelNo ratings yet
- Summarised Maths Notes (Neilab Osman)Document37 pagesSummarised Maths Notes (Neilab Osman)dubravko_akmacicNo ratings yet
- VDR G4 Manual Steinsohn PDFDocument185 pagesVDR G4 Manual Steinsohn PDFVariya Dharmesh100% (1)
- Research on Comparisons between Sabah and Diesel CyclesDocument8 pagesResearch on Comparisons between Sabah and Diesel CyclesjorgeNo ratings yet
- BTEC International Level 3 IT Pearson Set Assignment Unit 11 Cyber SecurityDocument8 pagesBTEC International Level 3 IT Pearson Set Assignment Unit 11 Cyber SecurityGergana Stamenova100% (1)
- A Report On Kantajew MandirDocument21 pagesA Report On Kantajew MandirMariam Nazia 1831388030No ratings yet
- A Primer On Financial Time Series AnalysisDocument93 pagesA Primer On Financial Time Series AnalysisKM AgritechNo ratings yet
- Mycophenolic Acid Chapter-1Document34 pagesMycophenolic Acid Chapter-1NabilaNo ratings yet
- 1.1 Enterprise AssessmentDocument1 page1.1 Enterprise AssessmentGermanRobertoFongNo ratings yet
- Technical Information System Overview Prosafe-Com 3.00 Prosafe-ComDocument49 pagesTechnical Information System Overview Prosafe-Com 3.00 Prosafe-Comshekoofe danaNo ratings yet
- Safety Data Sheet: 1. Identification of The Substance/preparation and of The Company/undertakingDocument4 pagesSafety Data Sheet: 1. Identification of The Substance/preparation and of The Company/undertakingBalasubramanian AnanthNo ratings yet
- Ce Brochure 20july16Document76 pagesCe Brochure 20july16Yogesh SharmaNo ratings yet
- JMPRTraininga I5545e PDFDocument500 pagesJMPRTraininga I5545e PDFmvptoxNo ratings yet
- FMAI - Ch04 - Stock MarketDocument105 pagesFMAI - Ch04 - Stock Marketngoc duongNo ratings yet
- Health Fitness Guide UK 2018 MayDocument100 pagesHealth Fitness Guide UK 2018 MayMitch Yeoh100% (2)
- The Manning EquationDocument10 pagesThe Manning EquationFederico LeonNo ratings yet
- The Beggar's Opera by Gay, John, 1685-1732Document50 pagesThe Beggar's Opera by Gay, John, 1685-1732Gutenberg.orgNo ratings yet
- TM T70 BrochureDocument2 pagesTM T70 BrochureNikhil GuptaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)