You might also like
- NCM 106 PHARMACOLOGY - PrelimsDocument26 pagesNCM 106 PHARMACOLOGY - PrelimsKelsey Macaraig100% (3)
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- PharmacologyDocument51 pagesPharmacologyAndy MirandaNo ratings yet
- BASIC PRINCIPLES OF PHARMACOLOGY For DENTISTRYDocument142 pagesBASIC PRINCIPLES OF PHARMACOLOGY For DENTISTRYKuya RnJNo ratings yet
- Week 2 PCOL211 Review of Pharmacodynamics - Evaluation of DrugsDocument15 pagesWeek 2 PCOL211 Review of Pharmacodynamics - Evaluation of DrugsTrixie SalcedoNo ratings yet
- Introduction To PkokineticsDocument3 pagesIntroduction To PkokineticspdladvaNo ratings yet
- Introduction To PharmacotherapeuticsDocument21 pagesIntroduction To Pharmacotherapeuticstf.almutairi88No ratings yet
- PN-Chapter 2-Introduction To Drug ActionDocument52 pagesPN-Chapter 2-Introduction To Drug ActionmysNo ratings yet
- Unit #1 IntroductionDocument22 pagesUnit #1 IntroductionSaima VictorNo ratings yet
- 4.1 BiopharmaceuticsDocument8 pages4.1 BiopharmaceuticsAzech Yam Ü100% (1)
- Unit #1 IntroductionDocument22 pagesUnit #1 IntroductionSaima VictorNo ratings yet
- Intro + Pharmacodynamics 2Document46 pagesIntro + Pharmacodynamics 2Dana E AbuqaudNo ratings yet
- P&T Chapter Wise 300 MCQDocument13 pagesP&T Chapter Wise 300 MCQsudeep kulkarni100% (1)
- Pharmacology Pharmacokinetics and Pharmacodynamics - PPT - Dr. Maulana Antian Empitu (Airlangga Medical Faculty)Document59 pagesPharmacology Pharmacokinetics and Pharmacodynamics - PPT - Dr. Maulana Antian Empitu (Airlangga Medical Faculty)rizkyyunitaa15No ratings yet
- Subject Forensic ScienceDocument12 pagesSubject Forensic SciencepartikNo ratings yet
- Pharmacology: Outline PharmacodynamicsDocument11 pagesPharmacology: Outline PharmacodynamicsAlloiBialbaNo ratings yet
- Pharma Trans 1 PHARMA, TOXI, DYNA, THERADocument7 pagesPharma Trans 1 PHARMA, TOXI, DYNA, THERAFiel Virata 許慧安No ratings yet
- Articulo 1 Farmacodinámica PDFDocument4 pagesArticulo 1 Farmacodinámica PDFdavid stNo ratings yet
- Pharmacology Course OutlineDocument15 pagesPharmacology Course OutlineKeith OmwoyoNo ratings yet
- PHARMA 02. PharmacodynamicsDocument11 pagesPHARMA 02. PharmacodynamicsCindy Mae MacamayNo ratings yet
- PharmaDocument4 pagesPharmaJake RenNo ratings yet
- Medicinal Chemistry I 1435h: Drug Structure & Pharmacological ActivityDocument59 pagesMedicinal Chemistry I 1435h: Drug Structure & Pharmacological ActivityAbd ElraHman ElbahraWyNo ratings yet
- MT6314 1st LessonDocument7 pagesMT6314 1st Lessonlanceferdinand.tan.pharmaNo ratings yet
- 01.20.01 Pharmacodynamics 2 - Mechanisms of Drug ActionDocument11 pages01.20.01 Pharmacodynamics 2 - Mechanisms of Drug ActionMikmik DGNo ratings yet
- Sour-C E: Rang & Dale's Phamacology, Elsevier: Ap Animate DatesDocument53 pagesSour-C E: Rang & Dale's Phamacology, Elsevier: Ap Animate DatessintiaNo ratings yet
- Pharmacology Block 1.3 - PharmacodynamicsDocument12 pagesPharmacology Block 1.3 - Pharmacodynamicsdaleng subNo ratings yet
- Pharmacology 1Document2 pagesPharmacology 1Nairin W. EdzlaNo ratings yet
- P PH Ha Arrm Ma Ac Co Od Dy Yn Na Am Miic Cs S A An ND D S Siig GN Na All T Trra An Ns SD Du Uc Cttiio On N 2Document12 pagesP PH Ha Arrm Ma Ac Co Od Dy Yn Na Am Miic Cs S A An ND D S Siig GN Na All T Trra An Ns SD Du Uc Cttiio On N 2Enrique GuerreroNo ratings yet
- PharmacokineticsDocument32 pagesPharmacokineticssaravanan1987100% (4)
- 1 PHA6120 IntroductionDocument86 pages1 PHA6120 Introductionchristian redotaNo ratings yet
- Pdynamics For PrescrberDocument6 pagesPdynamics For PrescrberpdladvaNo ratings yet
- BP (Protein Binding)Document13 pagesBP (Protein Binding)Babu PatelNo ratings yet
- Pharmacology Module 1Document6 pagesPharmacology Module 1maurizemedija15No ratings yet
- Chapter 2Document6 pagesChapter 2FazeelaNo ratings yet
- Pilapil PharmacologyDocument6 pagesPilapil PharmacologyIza FaboresNo ratings yet
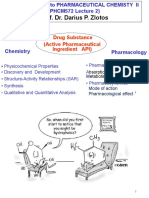
- Prof. Dr. Darius P. Zlotos: Drug Substance (Active Pharmaceutical Ingredient API)Document24 pagesProf. Dr. Darius P. Zlotos: Drug Substance (Active Pharmaceutical Ingredient API)Mirette AshrafNo ratings yet
- 4 PharmacaldynamicsDocument274 pages4 PharmacaldynamicsLulu MushiNo ratings yet
- Pharmacology IDocument82 pagesPharmacology IMelanieNo ratings yet
- UnitI PHARMACOLOGYTOXICOLOGYDocument29 pagesUnitI PHARMACOLOGYTOXICOLOGYGURU BEN PIANO STUDIO PRODUCTIONNo ratings yet
- Pharmacokinetics 1: AbsorptionDocument15 pagesPharmacokinetics 1: AbsorptionCecilia GrayebNo ratings yet
- Modul: Pharmacodynamics I. DescriptionDocument9 pagesModul: Pharmacodynamics I. DescriptionEli Ezer SimangunsongNo ratings yet
- Cap 2 FarmacoDocument21 pagesCap 2 Farmacomgch99No ratings yet
- PHARMACOLOGYDocument3 pagesPHARMACOLOGYEMETERIO TUTOR IIINo ratings yet
- 01.25.01 Principles of Pharmacokinetics - Absorption and DistributionDocument10 pages01.25.01 Principles of Pharmacokinetics - Absorption and DistributionMikmik DGNo ratings yet
- Topic 1 & 2Document14 pagesTopic 1 & 2Julianne Marie LacsentoNo ratings yet
- Insignis Pharma PharmacodynamicsDocument9 pagesInsignis Pharma PharmacodynamicsMa. Mil Adrianne PamaNo ratings yet
- Cara Baca SWISSADME-TargetPredDocument38 pagesCara Baca SWISSADME-TargetPredVictor DelacroixNo ratings yet
- Introduction To Biopharmaceutics and PharmacokineticsDocument3 pagesIntroduction To Biopharmaceutics and PharmacokineticsSyeda Eshaal JavaidNo ratings yet
- Pharmacology Module 2Document7 pagesPharmacology Module 2maurizemedija15No ratings yet
- Pharmi Blocki 14Document139 pagesPharmi Blocki 14202210034No ratings yet
- Agonists This Means That TheyDocument5 pagesAgonists This Means That TheyMaya Audrey KanekoNo ratings yet
- Biopharmaceutics & Pharmacokinetics: PCT400 (AY 2021-2022)Document7 pagesBiopharmaceutics & Pharmacokinetics: PCT400 (AY 2021-2022)Shaira MuksanNo ratings yet
- 1 General Principle of PharmacologyDocument4 pages1 General Principle of Pharmacologys.palao.annfrencislouiseNo ratings yet
- Lec1 - Introduction To Pharmacology - 1Document38 pagesLec1 - Introduction To Pharmacology - 1ABDALRHMAN ABU ZAIDNo ratings yet
- 2021-DD 01-IntroductionDocument36 pages2021-DD 01-IntroductionAlyamni AllNo ratings yet
- Week 2 - Pharmacodynamics PhaseDocument3 pagesWeek 2 - Pharmacodynamics PhaseTEDDY BEAR PRODUCTIONNo ratings yet
- 2 - Pharmacodynamics and Signal - 2012 - Elsevier S Integrated Review PharmacoloDocument11 pages2 - Pharmacodynamics and Signal - 2012 - Elsevier S Integrated Review PharmacoloCecilia GrayebNo ratings yet
- Bioavailability, Bioequivalence and BCS System: by Dr. Ashwani Kumar VermaDocument35 pagesBioavailability, Bioequivalence and BCS System: by Dr. Ashwani Kumar Vermagopal jhaNo ratings yet
- Articulo FarmacocineticaDocument12 pagesArticulo FarmacocineticaJESUS DAVID BOLA‹O JIMENEZNo ratings yet
- Safety Policy PDFDocument2 pagesSafety Policy PDFAnonymous Y6VYmM7zNo ratings yet
- August 2012Document64 pagesAugust 2012Eric SantiagoNo ratings yet
- Rodriguez, Et Al. 2004. MPC Fluoroquinolones For M.tuberculosisDocument4 pagesRodriguez, Et Al. 2004. MPC Fluoroquinolones For M.tuberculosisraindrasNo ratings yet
- Indian Herbs and Herbal Drugs Used For The Treatment of Diabetes PDFDocument12 pagesIndian Herbs and Herbal Drugs Used For The Treatment of Diabetes PDFPremkumar VNo ratings yet
- OBAT2Document12 pagesOBAT2AuliaHadiningratNo ratings yet
- Can Ambien Cause AmnesiaDocument4 pagesCan Ambien Cause Amnesiaark6of7No ratings yet
- MMS Usage ChartDocument1 pageMMS Usage Chartyrneh3No ratings yet
- Clinical Research MethodologyDocument11 pagesClinical Research MethodologymisganaNo ratings yet
- BB Biotech ReportDocument24 pagesBB Biotech ReportVíctor MentosNo ratings yet
- Alternative MedicineDocument318 pagesAlternative MedicineSudhansu Ranjan Swain100% (4)
- Nausea and Vomiting in Palliative Care Audit PresentationDocument68 pagesNausea and Vomiting in Palliative Care Audit PresentationGonzalo MaldonadoNo ratings yet
- Dossier Common Technical Document CTD Index: (Sample Document Will Provide On Request)Document6 pagesDossier Common Technical Document CTD Index: (Sample Document Will Provide On Request)Karem EladweyNo ratings yet
- Protein & Peptide Drug Delivery SystemDocument12 pagesProtein & Peptide Drug Delivery SystemSandeep SainiNo ratings yet
- Online Testing 2019Document4 pagesOnline Testing 2019api-488199038No ratings yet
- PHAR Midterm Notes - History of PH PharmacyDocument2 pagesPHAR Midterm Notes - History of PH PharmacyKami Nisama100% (4)
- Monitoreo de Ambientes en MerckDocument32 pagesMonitoreo de Ambientes en MerckPedro978No ratings yet
- Pharmaceutical Waste in The Environment: A Cultural PerspectiveDocument6 pagesPharmaceutical Waste in The Environment: A Cultural PerspectiveTerrence Terry BhengoeNo ratings yet
- Stability of Probiotic in Capsules PDFDocument4 pagesStability of Probiotic in Capsules PDFanand1540No ratings yet
- Formulation of Immediate Release Dosage Form of Ranitidine HCL Tabletsusing HPMC and Starch Acetate Film FormerDocument11 pagesFormulation of Immediate Release Dosage Form of Ranitidine HCL Tabletsusing HPMC and Starch Acetate Film Formersunaina agarwalNo ratings yet
- How To Calculate Ddds FinalDocument11 pagesHow To Calculate Ddds FinalO' They AdistNo ratings yet
- Dapuss DapusDocument3 pagesDapuss DapusidaapriliaNo ratings yet
- Amphotericin B Deoxycholate (Conventional) - Drug Information - UpToDate-6Document4 pagesAmphotericin B Deoxycholate (Conventional) - Drug Information - UpToDate-6Vh TRNo ratings yet
- Alkaloid OpiumDocument22 pagesAlkaloid OpiumPhoethree LauTnerNo ratings yet
- Requirement of Dissolution Test For f2 - Gastro Resistant TabletDocument17 pagesRequirement of Dissolution Test For f2 - Gastro Resistant Tabletfad12345No ratings yet
- Sympathetic Agonist and Antagonist 23Document12 pagesSympathetic Agonist and Antagonist 23PNo ratings yet
- Bản Sao Tóm Tắt Các ThuốcDocument10 pagesBản Sao Tóm Tắt Các ThuốcHan NguyenNo ratings yet
- F&IP Lab Manual 4th YearDocument173 pagesF&IP Lab Manual 4th YearVargheseNo ratings yet
- Stok Opname AprilDocument5 pagesStok Opname AprilRunaya Haryadi NingsihNo ratings yet
- Mirena Warning Letter From Department of Health To Bayer, Challenging Misleading and Unsubstantiated StatementsDocument7 pagesMirena Warning Letter From Department of Health To Bayer, Challenging Misleading and Unsubstantiated StatementsPublicNo ratings yet
- Care PlanDocument11 pagesCare PlanAlyssa Cardinal100% (1)