You might also like
- Cardiopulmonary Interaction in Critically Ill Patients: Major Determinants of Cardiovascular Responses to VentilationDocument48 pagesCardiopulmonary Interaction in Critically Ill Patients: Major Determinants of Cardiovascular Responses to VentilationAshish PandeyNo ratings yet
- Physiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiDocument52 pagesPhysiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiGHALEB A. AlmekhlafiNo ratings yet
- Physiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiDocument52 pagesPhysiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiGHALEB A. AlmekhlafiNo ratings yet
- Dynamic AuscultationDocument47 pagesDynamic AuscultationSrinivas PingaliNo ratings yet
- Fisiologi ShockDocument31 pagesFisiologi Shockdmandatari7327No ratings yet
- Fluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CADocument9 pagesFluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CAerwanNo ratings yet
- Hemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureDocument7 pagesHemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureKyle Saberon100% (1)
- Fluid ResponsivenessDocument27 pagesFluid ResponsivenessBiko Adji S. RahardjoNo ratings yet
- Bedside Preload Assessment CVP, PLR and USG Guided JCCA Bali 2016Document36 pagesBedside Preload Assessment CVP, PLR and USG Guided JCCA Bali 2016Ari YudhaNo ratings yet
- Physiology of Venous ReturnDocument42 pagesPhysiology of Venous Returncovid kojaNo ratings yet
- Coordinated cardiovascular responses to posture, Valsalva maneuver and exerciseDocument10 pagesCoordinated cardiovascular responses to posture, Valsalva maneuver and exerciseDrbee10No ratings yet
- Chap+12+CO, VRegul+Fall11 1Document17 pagesChap+12+CO, VRegul+Fall11 1Drbee100% (1)
- Cardiac Output Regulation and MeasurementDocument18 pagesCardiac Output Regulation and MeasurementGauravSinghNo ratings yet
- Hemodynamic MonitoringDocument33 pagesHemodynamic MonitoringISICLE GTNo ratings yet
- Arterial Pressure RegulationDocument50 pagesArterial Pressure RegulationareebNo ratings yet
- Cardiovascular PhysiologyDocument5 pagesCardiovascular Physiologycentrino1750% (2)
- Physiology of Hemodynamics-2: Clinical Implications of Shock StatesDocument37 pagesPhysiology of Hemodynamics-2: Clinical Implications of Shock StatesGHALEB A. AlmekhlafiNo ratings yet
- Graficastaller 2Document13 pagesGraficastaller 2Alberto MHNo ratings yet
- Cardiac Cycle JVPDocument70 pagesCardiac Cycle JVPAstrid PramudyaaNo ratings yet
- Coronary Circulation: Two Coronary Arteries (RT & LT) Arises From The Root of Aorta Supply Blood To MyocardiumDocument43 pagesCoronary Circulation: Two Coronary Arteries (RT & LT) Arises From The Root of Aorta Supply Blood To MyocardiumPhysiology by Dr RaghuveerNo ratings yet
- Regulation of Blood PressureDocument25 pagesRegulation of Blood PressurePhysiology by Dr RaghuveerNo ratings yet
- Swan Ganz FinalDocument36 pagesSwan Ganz FinalDanial HassanNo ratings yet
- Fuhrman2011. PEDIATRIC CRITICAL CARE, Ed 4 ISBN - 978-0-323-07307-3Document13 pagesFuhrman2011. PEDIATRIC CRITICAL CARE, Ed 4 ISBN - 978-0-323-07307-3Luz DiazNo ratings yet
- NCM 118 LECTURE Hemodynamics Understanding The Basic Principles 2021 For Canvas UpdatedDocument59 pagesNCM 118 LECTURE Hemodynamics Understanding The Basic Principles 2021 For Canvas UpdatedPollen Siega BunalNo ratings yet
- Myocardial Protection and CardioplegiaDocument56 pagesMyocardial Protection and CardioplegiaArhanNo ratings yet
- Physiology of Hemodynamics-2: Dr. Ghaleb AlmekhlafiDocument37 pagesPhysiology of Hemodynamics-2: Dr. Ghaleb AlmekhlafiGHALEB A. AlmekhlafiNo ratings yet
- Physio-DES-6 (Cardiac)Document56 pagesPhysio-DES-6 (Cardiac)Joseph Kim100% (1)
- Anatomy & Physiology of The HeartDocument30 pagesAnatomy & Physiology of The HeartejarnmdNo ratings yet
- Interpretation CVP Measurements: Vol26 I971Document7 pagesInterpretation CVP Measurements: Vol26 I971AsmaahammadNo ratings yet
- Applied Cardiovascular PhysiologyDocument1 pageApplied Cardiovascular Physiologyoperation KDNANo ratings yet
- CV AnatomyDocument49 pagesCV AnatomymichaelNo ratings yet
- CVP Guided Deresuscitation in Managing Overload in Icu PDFDocument57 pagesCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- Short and Long Term Regulation and Determinants of BPDocument90 pagesShort and Long Term Regulation and Determinants of BPDan Tristam MicabaloNo ratings yet
- Intra Aortic Balloon CounterpulsationDocument39 pagesIntra Aortic Balloon Counterpulsationmerin sunilNo ratings yet
- Blood PressureDocument58 pagesBlood PressureAyurveda PgNo ratings yet
- Inotropes and Vasoconstictor PackageDocument25 pagesInotropes and Vasoconstictor PackageYoussef MokdadNo ratings yet
- Regulation of Aterial Blood PressureDocument18 pagesRegulation of Aterial Blood Pressurenihal handNo ratings yet
- Cardiac L4Document19 pagesCardiac L4Qutaybah JahmanyNo ratings yet
- 2010 Systolic Properties of The Left VentricleDocument5 pages2010 Systolic Properties of The Left VentriclexeroldNo ratings yet
- Blood Pressure Regulation MechanismsDocument68 pagesBlood Pressure Regulation MechanismsPhysiology by Dr RaghuveerNo ratings yet
- Pericardial1 221013202347 8e6727d0Document54 pagesPericardial1 221013202347 8e6727d0Fiorella GonzalesNo ratings yet
- LVAD-Induced Reverse ModelingDocument46 pagesLVAD-Induced Reverse ModelingKitchanan KosalathipNo ratings yet
- Cardiovascular PhysiologyDocument49 pagesCardiovascular PhysiologyAndreea ŞtefănescuNo ratings yet
- Cardiac Output, Venous Return, and Their RegulationDocument50 pagesCardiac Output, Venous Return, and Their RegulationMohammed T. Abdul Razak100% (1)
- Cardiacmanuveres 160818075238Document56 pagesCardiacmanuveres 160818075238Rapmle PrasadNo ratings yet
- Blood PressureDocument64 pagesBlood PressureSrishti GoenkaNo ratings yet
- Pitfalls in Anesthesia MonitoringDocument56 pagesPitfalls in Anesthesia MonitoringDr.Sandeep Kumar Kar100% (1)
- Cardiac Physiology NotesDocument11 pagesCardiac Physiology Notespunter11100% (1)
- PhysiologyDocument10 pagesPhysiologyAmyrah MagajiNo ratings yet
- 1 VascularDocument75 pages1 Vasculareman el saeedNo ratings yet
- Graphical Analysis of CO and VR CurvesDocument29 pagesGraphical Analysis of CO and VR Curvesevamed2027No ratings yet
- NCMB 418 Hemodynamics Week 7Document34 pagesNCMB 418 Hemodynamics Week 7Jennifer Ambrosio100% (1)
- Heart Failure PharmDocument7 pagesHeart Failure PharmAmitShettyNo ratings yet
- Hemodynamic Monitoring Pocket CardDocument5 pagesHemodynamic Monitoring Pocket CardFitz JaminitNo ratings yet
- Section 3 Vascular PhysiologyDocument155 pagesSection 3 Vascular Physiologyraanja2No ratings yet
- Basic Concepts of Uid ResponsivenessDocument8 pagesBasic Concepts of Uid ResponsivenessibamdganiNo ratings yet
- Comparing LVEDP vs PCWP JAMA Cardio.2018Document2 pagesComparing LVEDP vs PCWP JAMA Cardio.2018Sajjad HussainNo ratings yet
- Right Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Document9 pagesRight Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Trần Quang HuyNo ratings yet
- Blood Pressure Regulation-2Document40 pagesBlood Pressure Regulation-2Juliza FelicianoNo ratings yet
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsFrom EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNo ratings yet
- Pathophysiology of Heart Failure With Reduced Ejection Fraction - Hemodynamic Alterations and Remodeling - UpToDateDocument29 pagesPathophysiology of Heart Failure With Reduced Ejection Fraction - Hemodynamic Alterations and Remodeling - UpToDatesamNo ratings yet
- Standardised Inotrope and Vasopressor Guidelines - Learning Package FINALDocument30 pagesStandardised Inotrope and Vasopressor Guidelines - Learning Package FINALInês MendonçaNo ratings yet
- Physiology Summary Chapter 20Document9 pagesPhysiology Summary Chapter 20gail01850% (2)
- Quiz Cardiovascular Part 1 of 3Document30 pagesQuiz Cardiovascular Part 1 of 3MedShare90% (10)
- Cardiovascular Physiology: Cardiac Output, Blood Flow ControlsDocument33 pagesCardiovascular Physiology: Cardiac Output, Blood Flow ControlsLuiz Jorge MendonçaNo ratings yet
- PiCCO Technology Brochure PDFDocument32 pagesPiCCO Technology Brochure PDFHue PhamNo ratings yet
- Cardiology Mcq's Part - 1Document31 pagesCardiology Mcq's Part - 1aymenNo ratings yet
- Cardiac OutputDocument31 pagesCardiac OutputDylan BhuriNo ratings yet
- Frank-Starling LawDocument5 pagesFrank-Starling LawNTA UGC-NETNo ratings yet
- Cardiac Contractility: Factors Affecting Strength of Heart Muscle ContractionDocument4 pagesCardiac Contractility: Factors Affecting Strength of Heart Muscle ContractionzaidNo ratings yet
- 3.cardiac OutputDocument18 pages3.cardiac Outputsamar yousif mohamedNo ratings yet
- Fluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CADocument9 pagesFluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CAerwanNo ratings yet
- Quick Guide To Cardiopulmonary Care 4th EditionDocument185 pagesQuick Guide To Cardiopulmonary Care 4th EditionLorenzo Romero AlbarranNo ratings yet
- The Heart As A PumpDocument25 pagesThe Heart As A PumpBali PalNo ratings yet
- Cardiovascular Physiology ConceptsDocument257 pagesCardiovascular Physiology ConceptsRicky Ali100% (1)
- Chapter 9 CARDIOVASCULAR SYSTEMDocument21 pagesChapter 9 CARDIOVASCULAR SYSTEMAlexander Santiago ParelNo ratings yet
- Congestive Heart Failure, Pulmonary Edema, and CPAPDocument35 pagesCongestive Heart Failure, Pulmonary Edema, and CPAPSherwan R Shal100% (1)
- Physio 2 - NotesDocument157 pagesPhysio 2 - NotesSivaranjini BhalaNo ratings yet
- Cardiovascular Physiology Concepts Klabu PDFDocument257 pagesCardiovascular Physiology Concepts Klabu PDFJer100% (4)
- Multiple Choice Questions: A. B. C. DDocument55 pagesMultiple Choice Questions: A. B. C. DwanderagroNo ratings yet
- Acute Care Handbook For Physical Therapists - 2nd Edition PDFDocument977 pagesAcute Care Handbook For Physical Therapists - 2nd Edition PDFShahid Ahmed Heera90% (10)
- Hemodynamic Parameters To Guide Fluid Therapy: Review Open AccessDocument9 pagesHemodynamic Parameters To Guide Fluid Therapy: Review Open AccessClaudioValdiviaNo ratings yet
- Kasus 6 (ADHF Grade II + NSTEMI + HHD + Dislipidemia) - Blok CVS - Tingkat 2 - NRP 1910211099 - REZA RAMADHANSYAHDocument34 pagesKasus 6 (ADHF Grade II + NSTEMI + HHD + Dislipidemia) - Blok CVS - Tingkat 2 - NRP 1910211099 - REZA RAMADHANSYAHReza RamadhansyahNo ratings yet
- Cardiovascular Physiology Applied To Critical Care and AnesthesiDocument12 pagesCardiovascular Physiology Applied To Critical Care and AnesthesiLuis CortezNo ratings yet
- Basic & Advanced Hemodynamic Monitoring Part 1 PDFDocument142 pagesBasic & Advanced Hemodynamic Monitoring Part 1 PDFUlfah UulNo ratings yet
- All CICM Examiner ReportsDocument432 pagesAll CICM Examiner ReportsHani MikhailNo ratings yet
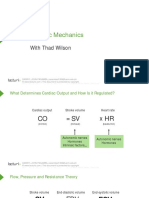
- Cardiac Mechanics: With Thad WilsonDocument26 pagesCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNo ratings yet
- 3 - Cardiac Contractility - Ass. Prof. Doaa Abou-Bakr - 2020Document8 pages3 - Cardiac Contractility - Ass. Prof. Doaa Abou-Bakr - 2020Hossam BaniisNo ratings yet
- Heart FailureDocument29 pagesHeart Failuremerin sunilNo ratings yet