You might also like
- 4 1Document2 pages4 1Raj BulaNo ratings yet
- Cellular CardiomyocyteDocument37 pagesCellular CardiomyocyteHiba PNo ratings yet
- Cardiac L2Document18 pagesCardiac L2Qutaybah JahmanyNo ratings yet
- The HeartDocument9 pagesThe HeartShiela Belandres MendozaNo ratings yet
- Learning Objectives: Chapter 4: Electrophysiology of The HeartDocument28 pagesLearning Objectives: Chapter 4: Electrophysiology of The HeartLaura PucheNo ratings yet
- Conduction System of HeartDocument7 pagesConduction System of HeartThakur KanchanNo ratings yet
- Physiology Worksheet Chapter Five: Cardiovascular SystemDocument2 pagesPhysiology Worksheet Chapter Five: Cardiovascular SystemTalya DannawiNo ratings yet
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- Cardiac AssessmentDocument54 pagesCardiac AssessmentAthira PSNo ratings yet
- G. Muscle Physiology - 1Document45 pagesG. Muscle Physiology - 1Milimo MweembaNo ratings yet
- Contractia MuscularaDocument33 pagesContractia MuscularaIulia JalbaNo ratings yet
- Cardio Physiology FullDocument11 pagesCardio Physiology FullSara Lee Wei LiNo ratings yet
- Lecture - 3 Properties of Cardiac MuscleDocument35 pagesLecture - 3 Properties of Cardiac MuscleMRM7MDNo ratings yet
- Mechanical Properties of The Heart IDocument30 pagesMechanical Properties of The Heart ISeba W WolfNo ratings yet
- Sifat Dan Kerja Otot Jantung - CVS-K10Document21 pagesSifat Dan Kerja Otot Jantung - CVS-K10Suci Intan FatrisiaNo ratings yet
- Lab Report 5 - Yixi LiuDocument22 pagesLab Report 5 - Yixi Liuapi-308855010100% (1)
- Aktivitas Elektrik Jantung: Rahmatina B. Herman Bagian Fisiologi Fakultas Kedokteran - UnandDocument33 pagesAktivitas Elektrik Jantung: Rahmatina B. Herman Bagian Fisiologi Fakultas Kedokteran - UnandRUNNINo ratings yet
- Topic 1 Biology 5Document21 pagesTopic 1 Biology 5Prachi SavaniNo ratings yet
- Physiology of the Circulatory System for Pharmacy StudentsDocument10 pagesPhysiology of the Circulatory System for Pharmacy StudentsMohaned MokhtarNo ratings yet
- Overview of AntihypertensiveDocument13 pagesOverview of AntihypertensiveKogulan SriNo ratings yet
- Clinical Electrocardiography and ECG Interpretation - ECG & ECHODocument15 pagesClinical Electrocardiography and ECG Interpretation - ECG & ECHORimaNo ratings yet
- Mechanical Function of The HeartDocument28 pagesMechanical Function of The HeartKarmilahNNo ratings yet
- Physiology of The Cardiovascular System - ENG AUDITDocument8 pagesPhysiology of The Cardiovascular System - ENG AUDITmarinescu danNo ratings yet
- Cardiovascular Physiology: The Autonomic Nervous SystemDocument8 pagesCardiovascular Physiology: The Autonomic Nervous SystemRidha Surya NugrahaNo ratings yet
- 38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciDocument16 pages38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciurtikikeNo ratings yet
- Characteristics of Cardiac Muscle Cells and Their Electrical PropertiesDocument36 pagesCharacteristics of Cardiac Muscle Cells and Their Electrical PropertiesLydia KosasihNo ratings yet
- Properties of Cardiac Muscle PDFDocument38 pagesProperties of Cardiac Muscle PDFZaid RazaliNo ratings yet
- Exer 2 Nerve Conduction Final ShitDocument3 pagesExer 2 Nerve Conduction Final ShitJosephineCarandangNo ratings yet
- Kuliah Muscle Contraction 2010Document69 pagesKuliah Muscle Contraction 2010bagir_dm10No ratings yet
- Circulation and Cardiovascular SystemDocument12 pagesCirculation and Cardiovascular SystemSatria MandalaNo ratings yet
- Physiology Lec: 2 Cardiovascular System دــيز .د يجقراطلاDocument7 pagesPhysiology Lec: 2 Cardiovascular System دــيز .د يجقراطلاArif NabeelNo ratings yet
- Physio, Mod1Document59 pagesPhysio, Mod1Ana AbuladzeNo ratings yet
- Cardiac Conduction System - WikipediaDocument32 pagesCardiac Conduction System - Wikipediakirubel demelashNo ratings yet
- CirculationDocument11 pagesCirculationRishikaphriya RauichandranNo ratings yet
- Pathophysiology On ArrhythmiaDocument34 pagesPathophysiology On ArrhythmiaYhr Yh100% (1)
- 225 AssignmentDocument7 pages225 AssignmentsadiqNo ratings yet
- Coordination: Physiology of Muscle Contraction and Different Muscle Contraction (Isotonic, Isometric, Isokinetic)Document6 pagesCoordination: Physiology of Muscle Contraction and Different Muscle Contraction (Isotonic, Isometric, Isokinetic)nn1216No ratings yet
- Electrical conduction system of the heart: an overview of its structure and functionDocument27 pagesElectrical conduction system of the heart: an overview of its structure and functionAnonymous gUjimJKNo ratings yet
- Muscle Lecture on Innervation and Contraction TypesDocument4 pagesMuscle Lecture on Innervation and Contraction TypesDan ChoiNo ratings yet
- Pathophysiology of Cardiovascular System Feghiu I., Tacu L., Iarovoi ADocument25 pagesPathophysiology of Cardiovascular System Feghiu I., Tacu L., Iarovoi ALunguVictoriaNo ratings yet
- MUSCLE PHYSIOLOGY: AN OVERVIEWDocument50 pagesMUSCLE PHYSIOLOGY: AN OVERVIEWJoyce Adjei-boateng100% (1)
- Physiology of The Normal Heart: Key PointsDocument5 pagesPhysiology of The Normal Heart: Key PointsGustavo TejerinaNo ratings yet
- Cardiac excitability, mechanisms of arrhythmia, and action of antiarrhythmic drugs - UpToDateDocument32 pagesCardiac excitability, mechanisms of arrhythmia, and action of antiarrhythmic drugs - UpToDateClaudia AlessandraNo ratings yet
- Skeletal Muscle Physiology PDFDocument6 pagesSkeletal Muscle Physiology PDFAstri Ggamjong Xiao LuNo ratings yet
- Heart 2018 - Part IDocument57 pagesHeart 2018 - Part Iwww.hudevaa6No ratings yet
- Physiology of Excitable Tissue and Action PotentialsDocument12 pagesPhysiology of Excitable Tissue and Action PotentialsTamar PertiaNo ratings yet
- Daftar Pustaka (Mini Projek)Document18 pagesDaftar Pustaka (Mini Projek)herfikaNo ratings yet
- Physiology Lec: 1 دــيز .د يجقراطلا Cardiovascular system (Introduction) HeartDocument6 pagesPhysiology Lec: 1 دــيز .د يجقراطلا Cardiovascular system (Introduction) HeartArif NabeelNo ratings yet
- Nervous SystemDocument6 pagesNervous Systembritney sookdeoNo ratings yet
- 22cardiac PV Loop Cardiac PhysiologyDocument19 pages22cardiac PV Loop Cardiac PhysiologyJaydave PatelNo ratings yet
- Chapter 12 Muscle Physiology - Important Questions: 6. Mechanism of Muscle ContractionDocument7 pagesChapter 12 Muscle Physiology - Important Questions: 6. Mechanism of Muscle ContractionIrum RafeeqNo ratings yet
- Bp503t Pcol Unit-IDocument77 pagesBp503t Pcol Unit-IAakkkNo ratings yet
- Muscoskeletal SystemDocument5 pagesMuscoskeletal SystemJeevikaGoyalNo ratings yet
- Phase 2 Cardiac Muscle - 1Document30 pagesPhase 2 Cardiac Muscle - 1erenyorulmaz143No ratings yet
- DhruvalHow Is Strength of Contraction Regulated in Different Types of MuscleDocument5 pagesDhruvalHow Is Strength of Contraction Regulated in Different Types of MuscleDhruvalNo ratings yet
- Frank-Starling LawDocument6 pagesFrank-Starling LawGauri RastogiNo ratings yet
- Summary Vet Quiz (Cvs-heart)Document3 pagesSummary Vet Quiz (Cvs-heart)Deeza Joice CastañedaNo ratings yet
- 01-Jenkins ch01 p01-026 PDFDocument26 pages01-Jenkins ch01 p01-026 PDFflaviana17No ratings yet
- Cardiac Muscle2Document39 pagesCardiac Muscle2Darius GanNo ratings yet
- Skeletal Muscle Lab: Structure, Function & Excitation-Contraction CouplingDocument19 pagesSkeletal Muscle Lab: Structure, Function & Excitation-Contraction Couplingkkk13whyNo ratings yet
- 17 - The Functional Structure of The Respiratory System - Ass. Prof. Mona Gamal - 2020Document7 pages17 - The Functional Structure of The Respiratory System - Ass. Prof. Mona Gamal - 2020Hossam BaniisNo ratings yet
- 18 - Mechanics of Respiration - Prof. Abdelrahman Fahmy - 2020Document5 pages18 - Mechanics of Respiration - Prof. Abdelrahman Fahmy - 2020Hossam BaniisNo ratings yet
- 5 - Cardiac Output - Ass. Prof. Dalia Abd El-Salam - 2020Document6 pages5 - Cardiac Output - Ass. Prof. Dalia Abd El-Salam - 2020Hossam BaniisNo ratings yet
- The Cardiac Cycle: - Again, This Is A Sequence of Events That Is Repeated With Each and EveryDocument4 pagesThe Cardiac Cycle: - Again, This Is A Sequence of Events That Is Repeated With Each and EveryHossam BaniisNo ratings yet
- Lecture (3) Body of The UterusDocument30 pagesLecture (3) Body of The UterusHossam BaniisNo ratings yet
- Fundamentals of Cardiology For The USMLE and General Medics PDFDocument287 pagesFundamentals of Cardiology For The USMLE and General Medics PDFMaria Patitu100% (2)
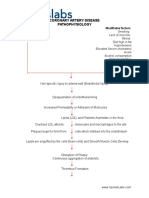
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps50% (4)
- Muscle AnswersDocument10 pagesMuscle AnswersTofik MohammedNo ratings yet
- Modified Sgarbossa CriteriaDocument13 pagesModified Sgarbossa CriteriaJenny de OzNo ratings yet
- Final Exam PracticeDocument6 pagesFinal Exam PracticeErvin T MileNo ratings yet
- Zoology I (EM) BLM 2021-22Document50 pagesZoology I (EM) BLM 2021-22Nishith ReddyNo ratings yet
- A Practical Approach To Cardiac Anesthesia-Lippincot - Wolters Kluwer (2012)Document1,677 pagesA Practical Approach To Cardiac Anesthesia-Lippincot - Wolters Kluwer (2012)ElenaCondratscribdNo ratings yet
- Muscle Tissue DefinitionDocument3 pagesMuscle Tissue DefinitionEleanor RamosNo ratings yet
- U Shield PremierDocument9 pagesU Shield PremierChiara YhaselleNo ratings yet
- Cell Injury RobbinsDocument44 pagesCell Injury RobbinsAnastasia DosiNo ratings yet
- Cardiovascular System SheetDocument11 pagesCardiovascular System SheetBetsy Brown ByersmithNo ratings yet
- Chapter 10-Rhythmical Excitation of The HeartDocument13 pagesChapter 10-Rhythmical Excitation of The Heartmuna s100% (1)
- Andersons Pediatric Cardiology 4ed 2020Document7,173 pagesAndersons Pediatric Cardiology 4ed 2020Nhựt Ý Nguyễn Phan100% (1)
- Ran Ola ZineDocument20 pagesRan Ola ZineHamza AlmaqtriNo ratings yet
- JV Electrophysiology of HeartDocument19 pagesJV Electrophysiology of HeartRiya GuptaNo ratings yet
- Cardiac PhysiologyDocument102 pagesCardiac PhysiologyPeter Larsen100% (1)
- Development, Basic Goals and Concepts in MyocardialDocument13 pagesDevelopment, Basic Goals and Concepts in MyocardialAtia KiranNo ratings yet
- Thermotherapy For Chest PainDocument8 pagesThermotherapy For Chest PainnabilaNo ratings yet
- Myocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPDocument94 pagesMyocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPLianne LagayanNo ratings yet
- Properties of Cardiac MuscleDocument60 pagesProperties of Cardiac MuscleBukhari Husain0% (1)
- Chapter 11 The Cardiovascular SystemDocument25 pagesChapter 11 The Cardiovascular SystemYeshia InocencioNo ratings yet
- ) Science (Department: Grade (10) Final Revision Worksheet (Biology)Document13 pages) Science (Department: Grade (10) Final Revision Worksheet (Biology)Toto BjNo ratings yet
- Non-Profit Organization Funds Gregory Grabovoi TeachingsDocument95 pagesNon-Profit Organization Funds Gregory Grabovoi Teachingsssss87va93% (27)
- Anatomy and Physiology - Circulatory System - The HeartDocument14 pagesAnatomy and Physiology - Circulatory System - The Heartxuxi dulNo ratings yet
- What Is CardiomyopathyDocument8 pagesWhat Is CardiomyopathysakuraleeshaoranNo ratings yet
- Full Download Test Bank For Robbins Basic Pathology 9th Edition Vinay Kumar Abul Abbas Jon Aster PDF Full ChapterDocument35 pagesFull Download Test Bank For Robbins Basic Pathology 9th Edition Vinay Kumar Abul Abbas Jon Aster PDF Full Chapternervous.vielle60lnwy100% (17)
- What Is Atrial DepolarizationDocument5 pagesWhat Is Atrial DepolarizationPrashant wadkarNo ratings yet
- Heart AnatomyDocument11 pagesHeart AnatomyJohn FisherNo ratings yet
- Locomotion and MovementDocument3 pagesLocomotion and MovementYouTutor PSNo ratings yet
- Guyton Physiology Chapter 9 OutlineDocument18 pagesGuyton Physiology Chapter 9 Outlinebahahahah100% (5)