Professional Documents
Culture Documents
Crohn's Disease
Uploaded by
Manuel alexanderOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Crohn's Disease
Uploaded by
Manuel alexanderCopyright:
Available Formats
Seminar
Crohn’s disease
Michael Dolinger, Joana Torres, Severine Vermeire
Crohn’s disease is a chronic inflammatory disease of the gastrointestinal tract that might lead to progressive bowel Published Online
damage and disability. The exact cause of Crohn’s disease is unknown, but evidence points towards multifactorial March 1, 2024
https://doi.org/10.1016/
events causing dysregulation of the innate immune system in genetically susceptible people. Commonly affecting the S0140-6736(23)02586-2
terminal ileum and proximal colon, Crohn’s disease inflammation is often discontinuous and patchy, segmental, and
Division of Paediatric
transmural. Identification of characteristic findings on ileocolonoscopy and histology remains the diagnostic gold Gastroenterology, Icahn School
standard, but complete assessment involves laboratory abnormalities, including micronutrient deficiencies, cross- of Medicine at Mount Sinai,
sectional imaging to identify transmural disease extent, severity and complications, and a psychosocial assessment. New York City, NY, USA
(M Dolinger MD); Division of
Treatment strategies for patients with Crohn’s disease now go beyond achieving clinical remission to include deeper Gastroenterology, Hospital da
targets of endoscopic healing and consideration of adjunctive histological and transmural targets to alter disease Luz, Lisbon, Portugal
progression potentially further. The use of early effective advanced therapies and development of therapies targeting (J Torres MD); Hospital Beatriz
alternative novel pathways with improved safety profiles have resulted in a new era of healing in Crohn’s disease Ângelo, Loures, Portugal
(J Torres); Faculdade de
management. Future combination of advanced therapies with diet or other biological drugs and small molecules, Medicina, Universidade de
together with improvements in tight control monitoring tools and predictive biomarkers might continue to improve Lisboa, Lisbon, Portugal
outcomes for patients with Crohn’s disease. (J Torres); Department of
Gastroenterology and
Hepatology, University
Introduction studies on incidence and prevalence from 1990 to 2016 Hospitals Leuven and KU
Crohn’s disease, one of the major entities within the reported a stable or decreasing incidence of adult Crohn’s Leuven, Leuven, Belgium
spectrum of inflammatory bowel diseases (IBDs), is a disease across most high-income countries, but not (Prof S Vermeire MD)
chronic inflammatory disease of the gastrointestinal tract paediatric Crohn’s disease and very-early onset IBD, in Correspondence to:
which might lead to progressive bowel damage and which incidence continues to rise.3 The highest reported Prof Severine Vermeire,
Department of Gastroenterology
disability.1 Crohn’s disease is now global, in part due to incidence rates of adult Crohn’s disease come from and Hepatology, University
rising incidence rates of adult and paediatric disease in Australia (29·3 × 10⁵ person-years), Canada (23·82 × 10⁵ Hospitals Leuven and KU Leuven,
middle-income countries.2,3 Novel insights of cells, cell– person-years), USA (13·9 × 10⁵ person-years), and Europe Leuven 3000, Belgium
cell communication, cytokines, and chemokines (15·4 × 10⁵ person-years). Nonetheless, high incidence severine.vermeire@uzleuven.be
implicated in disease pathogenesis, together with areas such as Denmark have reported incidence increasing
technological advances, have led to a substantial from 9·1 person-years (95% CI 8·3–10·0) in 1995 to
expansion of therapeutic options. Alongside the 17·8 person-years (16·8–19·0) in 2016. Prevalence rates
therapeutic revolution, modalities for non-invasive were highest in Europe (322·0 × 10⁵ person-years) and
monitoring to diagnose and follow-up patients are Canada (319 × 10⁵ person-years).3 In contrast to plateauing
rapidly emerging.4,5 Computational analyses of various incidence in high-income countries, areas of the world
omics data using patient-derived blood, stool, and tissue with historically low rates, such as Asia or South America,
samples provided new insights and biomarkers, some of seem to be witnessing an increase in incidence and
which are detectable before clinical onset of disease, prevalence, possibly due to changes in lifestyle, diet, and
opening the prospects of early diagnosis and disease pollution exposure.8 Data from sub-Saharan Africa also
prevention. This Seminar summarises the key advances indicate a recent rise in the incidence of ulcerative colitis,
of the past decade in each of these domains. followed by Crohn’s disease.9 Given that Crohn’s disease is
typically diagnosed at a young age, and is associated with
Epidemiology low mortality, prevalence is expected to reach up to 1% of
Crohn’s disease is usually diagnosed between ages 18 the population.8,10
years and 35 years; a second smaller peak has been
described between ages 50 years and 60 years.1 European Risk factors
and North American population-based studies have The strongest risk factor for developing Crohn’s disease is
reported a lower risk for women to develop Crohn’s having an affected first-degree relative (incidence rate
disease during childhood (as compared with ulcerative ratio 7·77, 95 CI 7·05–8·56; high-quality evidence).
colitis), until age 10–14 years, increasing thereafter, However, even in monozygotic twins, concordance for
especially after 25–29 years; in contrast to observations in Crohn’s disease reaches 50%, providing an argument for
Asia-Pacific populations, where predominance for Crohn’s the role of environmental factors in Crohn’s disease
disease in men was observed from adolescence to middle pathogenesis.11 Many environmental exposures have been
and late-middle age, potentially highlighting differences associated with increased Crohn’s disease risk, with
across world regions.6,7 Traditionally regarded as a disease variable strengths of evidence, such as cigarette smoking
of high-income countries of North America, Europe, and (odds ratio 1·76, 95% CI 1·40–2·20; moderate-quality
Oceania, the 21st century has seen an epidemiological evidence) and antibiotic exposure (1·74, 1·35–2·23; low
transition in IBD. Systematic reviews of population-based quality evidence), whereas others such as physical activity
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 1
Seminar
might reduce future risk of disease (relative risk 0·63, a key pathogenic factor, and inflammatory infiltrate is
95% CI 0·50–0·79; moderate-quality evidence).12–15 characterised by the Th1/Th17 response with production
Epidemiological studies have shown some early life of various proinflammatory cytokines (TNF-α, IFN-γ,
exposures (eg, breastfeeding and exposure to greenspace) IL-1, IL-6, IL-12, and IL-23) and impaired regulatory T-cell
reduce the risk of disease, whereas others (eg, childhood activity (figure 1).21–25 The luminal gut microbiota in
antibiotic exposure) increase the risk of disease, indicating Crohn’s disease is characterised by decreased diversity
a sensitive time-period for microbiome development and compared with healthy individuals, with a reduction in
immune system maturation that could repre sent a Firmicutes and Bacteroides, and an increase in
window of susceptibility for risk modulation.16,17 Dietary Actinobacteria and Proteobacteria. Specifically, the
factors including ultra-processed foods have been butyrate producers Faecalibacterium prausnitzii and
associated with higher risk for developing Crohn’s disease Roseburia spp are less abundant, whereas adherent-
(hazard ratio 1·82, 95% CI 1·22–2·72 for five or more invasive Escherichia coli are more abundant.26
servings per day; moderate-high-quality evidence).18
Clinical features
Pathophysiology Crohn’s disease can affect any gastrointestinal tract
The cause of Crohn’s disease is accepted to be segment, most commonly the terminal ileum and
multifactorial with hypotheses that the microbiome and proximal colon in a discontinuous, patchy, segmental,
other environmental factors drive inappropriate activation and transmural manner. Due to the transmural nature of
of the mucosal immune system in a genetically Crohn’s disease, fistula, abscesses, and strictures
susceptible host. Genome-wide association studies and frequently complicate the disease course. Extraintestinal
their meta-analyses have identified more than 260 risk manifestations, most commonly joint, skin, and eye
loci.19 Mutations in NOD2 (CARD15), the first identified manifestations, might be present in up to 50% of patients
gene conferring Crohn’s disease susceptibility, and other (figure 2).27 Presenting symptoms in Crohn’s disease can
identified pathways, such as autophagy and endoplasmic be variable, insidious, and dependent on location,
reticulum stress, point to dysregulation of the innate phenotype, and severity, which can result in delays in
immune system in response to luminal triggers to be key diagnosis. Chronic diarrhoea, abdominal pain, weight
in disease onset.20 loss, and fatigue presenting in a young adult should raise
The intestinal epithelium serves as a barrier between suspicion.28 Growth retardation or pubertal delay might
the intestinal lumen and environment and the mucosal be the single sign of Crohn’s disease in children and
immune system and protects against harmful bacteria. adolescents.29 In patients with stricturing disease,
An impaired intestinal epithelial barrier is recognised as post-prandial abdominal pain, bloating, nausea, or
Healthy state Diseased state
Terminal ileum
luminal environment Paneth cells with mutated genes
Barrier injury or Atg16L1 resulting in impairment in
Harmful
Secretion of breakdown function and decreased barrier
bacteria
antimicrobial (mucosal injury or integrity
invasion
factors inflammation)
Epithelium Paneth cells
NOD2 gene Tissue resident macrophages
expression working towards regeneration
of intestinal epithelial barrier
Cytokines
Immature
Extraluminal environment dentritic cell
(blood vessels, lymphatics, and mesentery) Naive
Monocyte
T cell
Th1, Th17
Plasma cell
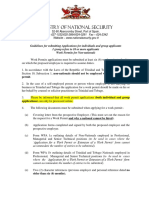
Figure 1: Intestinal epithelial barrier in the pathogenesis of Crohn’s disease
The intestinal epithelial barrier is visualised in both a healthy and diseased state, showing barrier injury as a key pathogenic factor in Crohn’s disease. Paneth cells,
an important source of NOD2 expression in the terminal ileum, play a central role in controlling bacterial invasion by secretion of antimicrobial factors. Paneth cell
metaplasia can result in their location outside of the terminal ileum, in the caecum, appendix, and distal colon. Paneth cells rely on autophagy to regulate secretory
capability and capacity. Disruption of this pathway through mutations in genes such as Atg16L1 result in impaired Paneth cell function, dysregulated microbiota, and
decreased barrier integrity. Tissue-resident macrophages are important for the regeneration of intestinal epithelial cells and for maintaining homeostasis in the gut.
2 www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2
Seminar
vomiting might be presenting features. Fistulising
disease symptoms depend on the affected organ:
enterovesical fistulae might present with faecaluria
pneumaturia or recurrent urinary tract infections;
Eyes or ocular
enteroenteric fistulae might be asymptomatic or Uveitis, episcleritis, and
complicate with inflammatory masses, phlegmons, or scleritis
Skin
abscesses; and rectovaginal fistulae might cause Erythema nodosum, pyoderma
dyspareunia or stool discharge from the vagina. gangrenosum, psoriasis, metastatic
Crohn’s disease, and Sweet’s syndrome
Approximately one-fifth of patients present with perianal Oral or mouth
lesions, which can include simple skin tags, anal canal Aphthous stomatitis,
periodontitis, and
lesions (stenosis, fissures, and ulcers), and fistulising orofacial granulomatosis
disease with or without perianal abscesses.30,31
Alternate diagnoses should be excluded through careful
clinical history. Recent gastrointestinal infections, travel, Lungs or respiratory
Granulomatous,
history of contact with tuberculosis, non-steroidal anti- lung disease
inflammatory drugs, and other drug intake should be
sought. Physical examination should evaluate for signs of
anaemia, dehydration, and malnourishment. Patients Liver
might present with a tender mass, most commonly in the Primary sclerosis
right iliac fossa. The perianal area should be carefully cholangitis, and
autoimmune hepatitis Pancreas
inspected for findings indicated above. Acute idiopathic pancreatitis,
and autoimmune pancreatitis
Diagnostic approach
Diagnosis often begins with non-invasive serum and stool
tests to detect inflammation and exclude infection.32
Joints or rheumatologic
Establishing the diagnosis of Crohn’s disease then Peripheral and axial
requires a combination of endoscopy to visualise the spondyloarthritis, and
enthesitis
mucosa, histological examination, and cross-sectional
imaging, with endoscopy and histopathology remaining
the gold standard.33–35 Diagnostic confirmation is crucial
after physical examination and exclusion of mimicking
pathologies, such as infectious enterocolitis (acute onset, Figure 2: Extraintestinal manifestations of Crohn’s disease
self-limited, microbial stool evaluation often revealing), Extraintestinal manifestations of Crohn’s disease might be present in up to 50% of patients, with multiple organs
involved and different manifestations within each organ.
intestinal Bechet (intestinal inflammation and recurrent
oral and genital ulceration), intestinal tuberculosis
(endemic exposure; histology reveals caseating granulo 2·7 mg/dL has the highest diagnostic positive predictive
mas instead of epithelioid granulomas), and familial value of 89·6%.40 However, many patients will have a
Mediterranean fever enterocolitis (recurrent fever attacks normal CRP despite active gastrointestinal tract
[Tel-Hashomer criteria]; histology reveals linear ulceration inflammation.41,42 Use of the stool biomarker faecal
without epithelioid cell granulomas).36–38 Age of symptom calprotectin less than 40 μg/g in the primary care setting
onset is important, as children 6 years and younger have can exclude diagnosis, with less than 1% of patients later
increased incidence of monogenic causes and immuno diagnosed.43 Faecal calprotectin concentrations greater
deficiencies, such as chronic granulomatous disease, than or equal to 1000 mg/g result in a maximum
making genetic testing necessary.39 After diagnosis is predictive value of 78·7% for Crohn’s disease activity,
established with endoscopy and histopathology, trans and concentrations less than 250 μg/g correlate with
mural disease extent, behaviour, and existing compli endoscopic remission in Crohn’s disease, whereas two
cations should be assessed using cross-sectional imaging. repeated values greater than 250 μg/g without symptoms
indicate a greater than 50% chance of developing relapse
Diagnostic investigations within 3 months.40,44 Additional serum tests for
Initial laboratory findings might include abnormalities hypoalbuminemia and micronutrient deficiencies, such
on the complete blood count, including leucocytosis, as iron, vitamin D, B12, B6, folate, selenium, and zinc
anaemia due to either chronic disease, or micro and can aid in diagnosis.
macroscopic blood loss via the gastrointestinal tract, or Although endoscopy is the diagnostic gold standard
both, and thrombocytosis, a surrogate marker of acute required, cross-sectional imaging, particularly intestinal
inflammation. Additional inflammatory markers, ultrasound, where available, can be used early in the
C-reactive protein (CRP), and erythrocyte sedimentation diagnostic evaluation to expedite endoscopy. Magnetic
rate might be elevated. A CRP greater than or equal to resonance enterography (MRE) or CT enterography
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 3
Seminar
(CTE) should be performed at diagnosis to evaluate the managed with 5-aminosalicylates, repeated corticosteroid
entirety of the bowel. MRE, where available, should be courses, and immunomodulators, the only available
considered first line over CTE in favour of limiting options at the time. High intestinal resection rates and
radiation exposure. Intestinal ultrasound can then complications from long-term corticosteroid exposure
complement MRE and CTE, having similar sensitivity to often left patients with clinical significant morbidities and
MRE for detecting disease presence in the terminal productivity loss. The approval of the first biological drug,
ileum (92% vs 97%).45 Intestinal ultrasound scores infliximab, in 1998, revolutionised Crohn’s disease
moderately correlate with the Simple Endoscopic Score treatment. The introduction of anti-TNF therapies led to
for Crohn’s Disease (SES-CD; p=0·55–0·80), showing major shifts in the therapeutic framework, from
high sensitivity (83–95%) and moderate specificity symptomatic clinical remission towards sustained deep
(70–85%) to detect endoscopic inflammation.46,47 remission. Treatment strategies shifted in parallel with
Endoscopic evaluation with histopathology for the evolution of therapeutic goals. Central to these
confirmation of Crohn’s disease diagnosis and exclusion strategies are the early introduction of effective therapy,
of mimicking pathologies is essential. The most common allied with a tight and frequent control of inflammatory
findings are longitudinal ulcerations, often with activity, and adjustment of therapy on the basis of that
erythema, oedema, and a nodular or cobblestone assessment (treat-to-target strategy).53,54
appearance of the mucosa.35 Scoring systems such as the
SES-CD and Crohn’s disease Endoscopic Index of Severity Evolution of endpoints and therapeutic goals
are used to grade severity of endoscopic inflammation.48,49 Therapeutic expansion has contributed to more stringent
See Online for appendix The hallmark histological feature of Crohn’s disease is endpoints in clinical trials (figure 3; appendix). The
the epithelioid granuloma; however, this is seen in fewer STRIDE II consensus incorporated both short (clinical
than 20% of biopsies. Additional histological features response [≤50% in patient reported-outcomes of abdominal
include focal patchy inflammatory infiltrate, lymphoid pain and stool frequency]), intermediate (clinical remission
aggregates, and pyloric gland metaplasia.34 When [abdominal pain score ≤1 and a stool frequency score ≤3, or
diagnosis is uncertain and suspicion remains, evaluation Harvey Bradshaw Index <5] and normalisation of
of the entire small bowel mucosa using wireless capsule biomarkers [CRP and faecal calprotectin <150–200 mg/g]),
endoscopy can be useful, especially in children with and long-term treatment goals (endoscopic healing
growth retardation.50 [SES-CD <3], normalised quality of life, absence of
disability, and restoration of growth for children).55
Classifying disease activity and severity Although histological and transmural healing are not yet
Using the above diagnostic approach, characterising formal treatment goals, they are considered useful
clinical features, serum and stool biomarkers, endoscopy adjunctive tools.
with histopathology, and cross-sectional imaging allows
for the classification of Crohn’s disease on the basis of Early intervention
location, phenotype, and severity (Montreal or Paris Post-hoc data have revealed that biological therapy is
Classification).51,52 Classification can aid in risk stratification more effective if introduced earlier in the disease course,
for the development of complications or surgery. preparing for the concept of early intervention and
opportunity. A systematic review and individual-patient
Management data meta-analysis of all placebo-controlled trials of
Management of Crohn’s disease has changed considerably biologics approved for Crohn’s disease showed that
in parallel with newly available therapies and therapeutic higher remission rates were observed during induction
strategy evolution. Previously, Crohn’s disease was in patients with shorter disease duration (≤18 months) in
Previous Current Future
Trials
Targan S CLASSIC-1 PRECISE-1 GEMINI2 UNITI 1&2 ADVANCE MOTIVATE
1997 2006 2007 2013 2016 2022 2022
Clinical response or remission
Endpoints
CDAI-70 Clinical remission CDAI-100 response, Clinical remission CDAI-100
response, (CDAI <150), week 6; response at (CDAI <150) and response, Endoscopic response
week 4 week 4 both weeks 6 and CDAI-100 week 6
26 in patients with response, CDAI <150 (USA), SF <2·8,
CRP >10 mg/L week 6 APS <1, week 12
Disease
modification
Figure 3: Evolution of treatment goals in Crohn’s disease trials with steroid-free remission and endoscopic response
APS=abdominal pain score. CDAI=Crohn’s disease activity index. CDAI-70=70-point decrease in Crohn’s disease activity index. CDAI-100=100-point decrease in
Crohn’s disease activity index. CRP=C-reactive protein. SF=stool frequency score.
4 www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2
Seminar
Efficacy Quality of the data Key adverse effects Limitations of data
5-aminosalicylate (oral)
57
5-aminosalycilates Not effective for induction or maintenance Low to moderate Well tolerated; key adverse events include renal Little data available on clinical
and sulphasalazine toxicity (interstitial nephritis and nephrotic response, PRO response and
syndrome), rare pulmonary toxicities (interstitial remission, biochemical and
lung disease and pulmonary granulomatosis), endoscopic improvement, and
pericarditis, and Stevens-Johnson syndrome serious adverse events
Budesonide57 (oral)
budesonide Effective in inducing clinical remission in Moderate Well tolerated; not to be used as a maintenance One RCT comparing budesonide to
mildly active ileal or ileocecal Crohn’s disease strategy; key adverse events include yeast 5-aminosalicylate with serious
compared with placebo; three RCTs infections (oral and genitourinary in females), inconsistency; overall no clinical
compared with mesalamine (no statistical urinary tract infections, and mild Cushing significant risk of bias; no high-
significant differences were observed for syndrome quality data on biomarker or
clinical remission, response, or adverse endoscopic response or remission
events)
Systemic corticosteroids57 (oral and intravenous)
Prednisone, Effective in inducing clinical remission and Moderate Adverse events five times more frequent Serious imprecision due to sparse
prednisolone, response in moderate to severe Crohn’s compared with placebo; key adverse events adverse events in RCTs, lowering
methylprednisolone disease; oral methylprednisolone 48 mg/day include Cushing syndrome, infection (increased the quality of evidence
and reduced on a weekly basis to 32 mg, risk of abdominal and pelvic abscesses in patients
24 mg, 20 mg, 16 mg, and 12 mg;58 oral with Crohn’s disease), and growth failure in
prednisolone ranged from 0·50 mg/kg to children; additional adverse events include
0·75 mg/kg, with a maximum daily dose of musculoskeletal (osteoporosis, osteonecrosis,
60 mg;59 prednisolone is usually tapered at and myopathy), acne, psychiatric (psychosis,
5 mg/week over an 8–12-week period, but suicidal ideation), metabolic (hypothalamic
can be tapered at a quicker rate depending pituitary axis suppression, hypertension,
on the efficacy of the advanced therapy diabetes, and cataracts), ecchymoses, and
initiated glaucoma
Thiopurines57 (oral)
6-mercaptopurine Not effective for induction of clinical Very low In a pooled analysis of five RCTs, no statistical Heterogenous trials (study design,
and azathioprine remission or response; recommend significant difference with placebo for adverse follow-up time, definition of active
Induction of performing thiopurine methyltransferase events; higher, albeit non-significant rates of disease, and definition of
remission before initiation; consideration of NUDT15 serious adverse events; key adverse events remission); most trials allowed for
polymorphisms depending on local include allergic reactions and pancreatitis concomitant use of steroids; the
guidelines to reduce potential adverse quality of evidence for estimating
events by starting at a lower dose or adding adverse events or serious adverse
allopurinol in the setting of events low due to reduced number
hypermethylation of events and wide confidence
intervals
6-mercaptopurine More effective than placebo based on a Moderate Adverse events and serious adverse events No data
and azathioprine pooled analysis in maintaining remission in during maintenance treatment were significantly
Maintenance of steroid-dependent Crohn’s disease patients higher than with placebo; key adverse events
remission include poor gastrointestinal tolerance,
myelosuppression, leukopenia, and potential
increased risk of malignancies (lymphoma, non-
melanoma skin cancer, myeloid disorders, and
urinary tract cancers); cautious use encouraged in
boys, adolescents, and young men and older
people who are at increased risk of developing
malignancy; other serious adverse events include
allergic reaction and infection
Methotrexate57 (oral and subcutaneous)
Induction of Effective for inducing clinical remission in Low Key adverse events resulting in treatment No studies looking at methotrexate
remission steroid-dependent patients over a 16-week discontinuation were liver enzyme elevation and monotherapy; the single RCT
period (25 mg/week of intramuscular nausea, which were significantly higher than available is limited by serious or
methotrexate combined with steroids); placebo very serious imprecision due to the
folate supplementation can be used to confounding effect of concomitant
reduce potential side-effects use of steroids
Maintenance of More effective than placebo in a single RCT Moderate Key adverse events are nausea and vomiting, Serious imprecision due to sparse
remission in maintaining remission in patients with which occurred more frequently among patients data; no data on biomarker
steroid-dependent Crohn’s disease compared with placebo remission, PRO remission, and
(methotrexate 15 mg/week intramuscularly) serious adverse events
(Table 1 continues on next page)
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 5
Seminar
Efficacy Quality of the data Key adverse effects Limitations of data
(Continued from previous page)
Anti-TNF57 (intravenous and subcutaneous)
Infliximab, Effective for induction and maintenance of Moderate Key serious adverse event include higher risk of Pooled analysis from RCTs limited
adalimumab, and clinical remission and response, and for serious infections and higher risk of lymphoma to assess steroid-free clinical
certolizumab pegol endoscopic improvement and remission in when combined with thiopurines, particularly in remission, PRO remission,
moderate to severe Crohn’s disease; older people; additional adverse events include radiological and biochemical
combination therapy with psoriasiform eczematous reactions of the skin remission, quality of life, and
immunomodulators might be used to serious adverse events
reduce development of anti-drug antibodies
Anti-Integrin57 (intravenous and subcutaneous)
Vedolizumab Effective for induction and maintenance of Moderate No statistical significant difference in adverse Limited quality of evidence, serious
clinical remission and response, for events or serious adverse events compared with (imprecision) to assess serious
maintenance of steroid-free clinical placebo in RCTs; no safety signals from long- adverse events due to sparse data;
remission, and for endoscopic improvement term follow-up studies to date; key adverse data on endoscopic, radiological,
and remission in moderate to severe Crohn’s events include Crohn’s disease exacerbation, and histological healing are not
disease; effective for inducing endoscopic, arthralgia, headache, and nausea; rarely, infusion placebo controlled; limited data on
radiological, and histological healing reactions (most often without the need for biomarker normalisation
discontinuation), enteric and sinopulmonary
infections, and diffuse severe musculoskeletal
pain occur
Anti-IL-12 or IL-2357 (intravenous and subcutaneous)
Ustekinumab Effective for induction and maintenance of Moderate to high No statistical significant difference in adverse Little data on biomarker and
clinical remission and response, for events or serious adverse events compared with endoscopic remission
maintenance of steroid-free clinical placebo in RCTs; no safety signals from long-
remission, and for endoscopic improvement term follow-up studies to date; key adverse
and remission in moderate to severe Crohn’s events include upper respiratory tract infection,
disease nasopharyngitis, infusion, and injection site
reactions; rare adverse events and serious
adverse events include serious infections,
arthralgias, rash, headache, and elevated
transaminases
Anti-IL-2360 (intravenous and subcutaneous)
Risankizumab Effective for induction and maintenance of High Lower risk of serious adverse events during Little real-world data available;
clinical remission and response, and for induction and maintenance with risankizumab long-term safety profile unknown
endoscopic remission was seen; key adverse events include in the setting of Crohn’s disease
hypersensitivity and injection site reactions and
hepatotoxicity; the most frequent adverse events
are headache, arthralgia, and nasopharyngitis
JAK inhibitors61 (oral)
Tofacitinib Not effective for inducing clinical remission Moderate to high Key serious adverse events include herpes zoster, High placebo rates, inclusion of
or endoscopic remission although not frequently encountered in Crohn’s patients with mild disease, and lack
disease RCTs; EMA PRAC assessment of requirement for centrally read
recommends caution to use on patients older confirmation of endoscopic
than 65 years with risk factors or history of inflammation or elevated CRP or
smoking due to potential risk for MACE and faecal calprotectin at enrolment
malignancy; other adverse events include
leukopenia, elevated transaminases,
hypercholesterolemia, and development or
worsening of acne
Filgotinib Effective for inducing clinical remission Moderate to high Key serious adverse events include herpes zoster, Failed to get regulatory approval
although not frequently encountered in Crohn’s due to failure to meet the co-
disease RCTs; EMA PRAC assessment primary endpoint of clinical
recommends caution to use on patients older remission and endoscopic response
than 65 years with risk factors or history of at week 10
smoking due to potential risk for MACE and
malignancy; other adverse events include
leukopenia, elevated transaminases,
hypercholesterolemia, and development or
worsening of acne
(Table 1 continues on next page)
6 www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2
Seminar
Efficacy Quality of the data Key adverse effects Limitations of data
(Continued from previous page)
Upadacitinib Effective for inducing and maintaining Moderate to high Key serious adverse events include herpes zoster, No data
clinical response and remission, and although not frequently encountered in Crohn’s
endoscopic improvement and remission disease RCTs; EMA PRAC assessment recommends
caution to use on patients older than 65 years
with risk factors or history of smoking due to
potential risk for MACE and malignancy; other
adverse events include leukopenia, elevated
transaminases, hypercholesterolemia, and
development or worsening of acne
Anti-TNF=anti-tumour necrosis factor. CRP=C-reactive protein. EMA=European Medicines Agency. MACE=major adverse cardiovascular events. PRAC=Pharmacovigilance Risk Assessment Committee.
PRO=patient reported outcome. RCT=randomised controlled trial.
Table 1: Efficacy and safety of Crohn’s disease pharmacotherapy
both active and placebo treatment groups, compared recommended for induction of remission.57 Systemic
with remission rates in patients with longer disease corticosteroids are effective in inducing remission in
duration (>18 months).56 However, absence of validated moderate-to-severe Crohn’s disease and other disease
objective biomarkers for prediction of disease course locations, but have no proven efficacy as maintenance
makes it difficult to appropriately select patients that treatment. Steroid-free remission is a major treatment
benefit the most from early intensive treatment. goal, and repeated systemic corticosteroid courses should
be avoided given the well known toxicity associated with
Medical management prolonged exposure (table 1).
Recent therapeutic expansion with new biologics and
small molecules, either recently introduced or soon to Immunomodulators
arrive in practice, has complicated treatment choice. Thiopurines (azathioprine and mercaptopurine) and
Treatment selection should actively involve the patient in methotrexate might be used as monotherapy for
the decision-making process and be individually guided by maintenance or remission in steroid-dependent Crohn’s
disease activity, location, phenotype, patient (comorbidities, disease and have an important role in preventing
lifestyle, wish for pregnancy, etc) and drug-related factors antidrug–antibody development (immunogenicity) to
(safety, cost, speed of onset, administration, etc). Patient anti-TNF.57 Efficacy of thiopurines to achieve endoscopic
education on therapeutic goals and monitoring strategy healing is substantially lower compared with anti-TNF.63
should be provided before treatment, in conjunction with Two controlled trials in early Crohn’s disease did not
treatment selection counselling. Table 1 summarises the show azathioprine monotherapy efficacy for disease modi
efficacy and safety of pharmacotherapy discussed below. fication.64,65 In the prospective PANTS study, immuno
modulator addition to anti-TNF mitigated the risk of
Aminosalicylates immunogenicity.66 Besides limited efficacy, thiopurines
Aminosalicylates are not effective in treating Crohn’s are frequently poorly tolerated (gastrointestinal intolerance
disease and have low efficacy to prevent postoperative in ~15% of patients), can cause myelosup pression,
recurrence and, therefore, should not be used during idiosyncratic pancreatitis, and have potential for increased
induction or maintenance. risk of malignancies (lymphoma, non-mela noma skin
cancers, myeloid disorders, and urinary tract cancers).
Antibiotics Therefore, thiopurines should be used with caution in
Antibiotics are indicated to treat Crohn’s disease-related young men and older patients who are at increased risk of
perianal and intra-abdominal abscesses, not for treatment developing malignancy.
of luminal Crohn’s disease nor as monotherapy for
complex fistulising disease.57 One study suggests that Anti-TNF therapy
ciprofloxacin combined with anti-TNF therapy could Anti-TNF agents are among the most effective therapies
impact anti-TNF efficacy for perianal fistula closure in to induce and maintain remission in Crohn’s disease.
the short term, but not long term, after antibiotic therapy Although three agents (infliximab, adalimumab, and
discontinuation.62 certoliziumab pegol) are approved, only infliximab and
adalimumab are used globally; use of certolizumab is
Corticosteroids limited to fewer countries. Infliximab is the only
For patients with mild localised ileal or ileocecal disease, advanced therapy with a dedicated randomised controlled
budesonide, a locally acting glucocorticosteroid with trial to show efficacy for the treatment of perianal disease,
fewer side-effects compared with prednisone, is whereas adalimumab has shown efficacy, compared to
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 7
Seminar
placebo, for fistula healing in the CHARM trial as a There has been a shift towards new convenient oral
secondary endpoint.67,68 Additional advantages of anti- agents in recent years that lack immunogenicity, have a
TNF include their efficacy in treating extraintestinal short half-life, and fast onset of action janus kinase (JAK)
manifestations, such as pyoderma, uveitis, psoriasis, and inhibitors interfere with STAT signalling and have broad
axial spondyloarthropathy, and specific situations such as and potent anti-inflammatory effects. Tofacitinib has not
stricture (CREOLE study) disease, postoperative shown efficacy in phase 2 studies and stopped further
prophylaxis (PREVENT study), and pregnancy (PIANO development in Crohn’s disease. Upadacitinib and
study).69–71 Due to immunogenicity potential, anti-TNF filgotinib, JAK-1 selective agents, completed phase 3.84,85
efficacy is improved when combined with an immuno The randomised phase 3 upadacitinib induction studies,
modulator.66 U-EXCEL and U-EXCEED, and the maintenance
Biosimilars, which are similar in efficacy and safety to U-ENDURE study, met primary endpoints of inducing
the originators while representing potential cost-savings and maintaining clinical remission and endoscopic
and greater access worldwide, have been approved since response in patients with moderate to severe Crohn’s
For more on Janus kinase September, 2013 in Europe and April, 2016 in the USA. disease.86 JAK inhibitors have advantages of targeting
inhibitors see https://www.ema. Although anti-TNFs provided an important therapeutic multiple extraintestinal mani festations but should be
europa.eu/en/medicines/human/
advancement, and for patients with perianal fistulising used with caution in patients with risk factors for
referrals/janus-kinase-inhibitors-
jaki disease remain the most effective option, response to thromboembolic events. Furthermore, this class of agents
treatment is not observed in 15–20% of patients, and should only be used if no alternative treatment options
30% of patients will lose response over time.66 Side- are available in patients 65 years or older, or at increased
effects of anti-TNFs, including serious infections and risk of cancer or major cardiovascular events (table 1).
psoriasiform eczematous reactions of the skin, paved the
way for newer, safer agents.72,73 The risks and benefits of Positioning of therapies
combination therapy with an immunomodulator need to With newer therapies arriving to clinical practice, there is
be considered, especially in older people, given the great debate on how to position and sequence advanced
higher risk for infections and lymphomas.74,75 therapies. The SEAVUE head-to-head trial comparing
ustekinumab and adalimumab as induction and
Therapies targeting alternative pathways to anti-TNF maintenance therapy in moderate-to-severe biological
Vedolizumab and ustekinumab are IgG1 biologics with naive Crohn’s disease showed similar rates of clinical
different mechanisms of action, the approval of which and endoscopic remission after 1 year.87 A recent network
followed anti-TNF for treatment of moderate-to-severe meta-analysis looking at efficacy of therapies in moderate-
Crohn’s disease. Both classes appear to have few serious to-severe Crohn’s disease reported that infliximab
side effects (table 1) and reduced immunogenicity 5 mg/kg ranked first for induction of clinical remission,
without the need for combination therapy with an but risankizumab 600 mg ranked first in patients who
immunomodulator, although long-term safety data are were biologically exposed. Upadacitinib 30 mg once per
still limited. First-line use is limited in many countries day ranked first for maintenance of remission.88 Although
due to reimbursement policies that require previous network meta-analyses might be useful to estimate
anti-TNF failure. comparative efficacy and safety outcomes, they reflect
Vedolizumab is an anti-α4β7 integrin monoclonal indirect comparisons and cannot replace head-to-head
antibody with gut selectivity, administered intravenously trials. Additionally, there is increasing acknowledgement
every 8 weeks during maintenance, following an that features such as disease location and disease
induction period (weeks 0, 2, and 6).76 Although gut duration can affect efficacy outcomes—aspects that are
selectivity of vedolizumab is responsible for its favourable usually not considered in randomised controlled trials.
safety profile, it limits the use in treatment of Crohn’s Although the quest for molecular markers that might
disease with extraintestinal manifestations. Within the guide therapy selection (precision medicine) continues,
class of lymphocyte trafficking agents, other molecules therapy positioning in clinical practice is often driven by
such as etrolizumab and ontamalimab have not met disease activity and desired safety profile, in addition to
efficacy endpoints in randomised controlled trials.77,78 other factors such as reimbursement policies, drug-
Ustekinumab, an anti-IL-12 and IL-23 p40 antibody, is related factors (cost or mode of administration), and
given by subcutaneous injection every 8 weeks following patient-related factors (comorbidities or wish for
weight-based dosage intravenous induction.79 pregnancy; table 1). In table 2, we describe some of the
Ustekinumab is also approved for plaque psoriasis and scenarios frequently encountered in clinical practice, and
psoriatic arthritis. Within the class of IL-12 and IL-23 how those might affect positioning for currently approved
signalling, promising antibodies targeting the p19 therapies for moderate-to-severe Crohn’s disease.
subunit are expected to provide better efficacy over
ustekinumab, and phase 3 data are available for Surgery
risankizumab, whereas phase 2 data have been published Surgical indications can be divided into abdominal
for mirikizumab and guselkumab.80–83 Crohn’s disease and perianal Crohn’s disease, with
8 www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2
Seminar
emergent and non-emergent considerations. Emergent
Initial therapy consideration Selection reasoning
abdominal Crohn’s disease surgery indications include
acute bowel obstruction with vomiting, absence of Age ≥60–65 years or other risk Vedolizumab or ustekinumab Lower risk of serious infections
factors for serious infections74,60 compared with anti-TNF or JAK
passage of stool or flatus per rectum, and intestinal
Perianal disease67,68 Infliximab (adalimumab as RCT data for infliximab; post-hoc
perforation, whereas non-emergent indications include second-line therapy if secondary data available for adalimumab
medically refractory disease and complications not LOR to infliximab)
amenable to medical therapy. For perianal Crohn’s Prevention of postoperative Anti-TNF or vedolizumab RCT data available
disease surgery, complex fistulae and perianal abscesses recurrence70
are common indications, with pelvic sepsis being an High inflammatory burden (deep Anti-TNF or upadacitinib Fast onset of action
ulcerations, high CRP,
emergent indication. Surgical management should be
hypoalbuminemia, or severe
multidisciplinary, including nutritional optimisation, disease activity)
steroid tapering, thromboembolic event prevention, Psoriasis or psoriatic arthritis Anti-TNF or ustekinumab Both target bowel and skin
laboratory abnormality correction, smoking cessation inflammation
counselling, and post-surgical monitoring and pro Axial spa Anti-TNF or JAKs Both target bowel and axial
phylactic therapy discussions.89 The positioning of inflammation
surgery early in Crohn’s disease has been supported by Preconception and pregnancy71 Anti-TNF (greatest experience), Established safety and do not
vedolizumab, or ustekinumab cross placenta during the first
the L!RIC trial,90 in which patients with uncomplicated trimester of pregnancy
terminal ileitis less than 40 cm, for whom conventional Thiopurine contraindicated Vedolizumab, ustekinumab, or Less or no immunogenicity; no
therapy did not elicit a response, were randomly assigned (intolerance or history of upadacitinib evident benefit of using
to early laparoscopic resection or infliximab initiation. pancreatitis) combination therapy to increase
The primary endpoint, quality of life (measured by the efficacy
Inflammatory Bowel Disease Questionnaire) was similar Loss of response to a first anti-TNF Alternative anti-TNF in Higher chances of developing
due to immunogenicity combination with antibodies to a second anti-TNF
in both groups.90 When comparing adverse events, clinical immunomodulators, agent compared with first anti-
significant surgical intervention-related complications vedolizumab, ustekinumab, and TNF
occurred in four of 73 patients in the resection group, upadacitinib
and treatment related serious adverse events occurred in Possible clinical scenarios that might drive therapeutic decision and positioning of different advanced therapies.
two of 70 patients in the infliximab group. At 5-year CRP=C-reactive protein. LOR=loss of response. RCT=randomised controlled trial. *The therapeutic options listed reflect
follow-up, although none of the surgical patients required the authors’ own clinical opinion.
re-resection, approximately one-quarter of patients Table 2: Positioning of Crohn’s disease therapies in different clinical scenarios*
required a biologic, whereas in the anti-TNF group half of
the patients needed surgery.91 As Crohn’s disease is
lifelong, and post-surgical recurrence occurs frequently, prolapse or obstruction should be discussed with the
balloon dilation or novel stent placement in patients patient before creation.
with obstructive Crohn’s disease should be
considered.92 Resection of the mesentery, and the Kono-S Mental health and the burden of living with Crohn’s disease
anastomosis (antimesenteric, functional, end-to-end, Crohn’s disease has a significant psychological impact, with
hand-sewn ileocolic anastomosis) are recently proposed anxiety and depressive symptoms in 35% and 22% of
surgical techniques that might decrease the chance of patients, respectively.95 Psychosocial comorbidities are often
postoperative recurrence when surgery is performed.93,94 exacerbated by unpredictable flares and symptoms, causing
During surgical resection, emphasis should be placed on coping difficulties and substantial distress; however, for
small bowel preservation and maintenance of continence many people, the severity of psychological distress is
for perianal surgery. independent of gastrointestinal activity.96 During periods of
Treatment and surgical management of perianal clinical remission, not only during flares, fatigue and
Crohn’s disease remains challenging. In a persistence of food-related issues can be reported in up to
multidisciplinary team approach with an experienced 50% of patients, including loss of appetite and independent
colorectal surgeon and gastroenterologist, treatment use of diet to control symptoms, which affect patient lives
might require examination under anaesthesia, incision, and require addressing during clinical visits.97,98 Symptoms
and drainage of abscesses, with placement of non-cutting of anxiety and depression in patients with IBD are often
setons to facilitate drainage of fistula tracts and prevent driven by specific areas of concern; disease impact,
ongoing infection and sepsis, and optimisation of treatment, intimacy, and stigma can contribute to work
medical therapies, simultaneously. Ultimately, many impairment and low self-esteem.99 Cognitive behavioural
patients require stoma creation to divert stool from the therapy is an effective option to improve symptoms of
perianal area to aid healing. However, once a stoma is anxiety or depression and quality of life in patients with
created, there is a high chance of permanence. Review of Crohn’s disease, but is limited by availability at few expert
potential stoma complications, such as leaking of stool centres.100
contents, peristomal complications such as pyoderma Psychosocial effects of Crohn’s disease can lead to high
gangrenosum, and surgical complications such as rates of disability. In a 10-year follow-up study of a Danish
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 9
Seminar
unselected population-based inception cohort, Crohn’s ability to monitor transmural disease activity using
disease patients presented substantial direct costs, but intestinal ultrasound for rapid response assessment and
also indirect costs of lost income, paid sick leave, leaves decision making and response has begun to shift cross-
of absence, or unemployment benefits.101 sectional imaging from a static to dynamic tool.
Incorporation of early intestinal ultrasound assessment,
Monitoring strategies and tools benchmarked to gold standard endoscopy and MRE to
Tight monitoring monitor responsiveness is likely to enhance our ability for
Central to disease control is activity monitoring in specific accurate tight monitoring. In centres where intestinal
intervals based on objective biomarkers (tight ultrasound is available for short interval tight monitoring,
monitoring). The CALM study was a randomised, two- MRE can be used in a similar treat-to-target manner as
arm, multicentre, open-label study, in which therapy was endoscopy to assess for transmural healing.
escalated based on symptoms (conventional group) or
objective biomarkers of inflammation, CRP or faecal Intestinal ultrasound as a monitor of treatment response
calprotectin, or both (tight control group).102 This study Two multicentre studies have shown that monitoring
showed that biomarker dominant tight control was treatment response to biological therapies with intestinal
associated with better clinical and endoscopic outcomes ultrasound is possible.107,108 A decrease in bowel wall
compared with symptom-driven control alone.102 thickness can occur within 12 weeks of treatment
initiation. In children with Crohn’s disease, changes in
Treat-to-target bowel wall thickness can be seen as early as 2 weeks
STARDUST was the first treat-to-target trial in Crohn’s after anti-TNF initiation; in adults, change in bowel wall
disease in which therapy was adjusted on the basis of thickness at 4 weeks could predict endoscopic
endoscopic response. The primary endpoint of endoscopic response.108,109
response (SES-CD decrease of 50%) at week 52 was not
met, possibly due to high efficacy in the standard of care Future direction
group and a primarily bio-naive population.103 The cluster Predicting disease onset and the prospect of disease prevention
randomisation REACT-2 trial in Crohn’s disease will Data support the concept that Crohn’s disease is present
assess whether treating to endoscopic healing will reduce before clinical symptoms.110 Preclinical studies could lead
disease progression and complications (NCT01698307). to a better understanding of disease initiation events and
After random assignment of 525 patients with Crohn’s potentially uncover biomarkers that aid in disease
disease to early combination therapy and therapy prediction and prognostication before symptoms.
intensification to target absence of ulcers (>5 mm in size; Antimicrobial markers and up to 51 proteins have been
enhanced care) and 569 patients to standard of care and shown to be predictive of Crohn’s disease future
treatment intensification to target clinical remission diagnosis.111,112 Antimicrobial antibodies in first-degree
(Harvey-Bradshaw Index <4), the primary endpoint relatives have also shown to increase risk of developing
(Crohn’s disease-related complications) was achieved in future Crohn’s disease.113 Increased intestinal permeability
40·9% and 43·1% of patients (adjusted risk difference was also associated with future development of Crohn’s
[ARD] −1·5%; 95% CI −10·2 to 7·2; p=0·73). Although disease.114
complete analysis is needed, a high proportion of patients
in remission at study entry might be the reason for the Predicting disease course
apparent lack of significant difference in endpoints To better predict disease at diagnosis, the RISK cohort of
between groups. In post-hoc analysis based on active newly diagnosed, treatment-naive paediatric patients
disease, defined by CRP greater than 5 mg/L and presence with Crohn’s disease identified an extracellular matrix
of baseline ulcerations, the ARD was −15·1% (−27·8 to signature associated with risk of stricture within 3 years.115
−2·4) and −21·6% (−34·3% to 8·9; p<0·001) for enhanced A CD8+ T-cell transcriptional signature that has been
care versus standard-of-care, respectively.104 shown to predict disease course is currently being
explored in the biomarker-stratified PROFILE trial.116,117
Cross-sectional imaging in the treat-to-target strategy
STRIDE-II considered transmural healing as an adjunctive Monitoring disease progression
goal, but since publication, increased use of transmural The SPIRIT initiative proposed goals to achieve in disease-
disease activity monitoring and healing as a treatment modification trials for preventing disease progression.118
target have become increasingly recognised.55 MRE The Lemann Index, an objective reproducible measure of
indices have shown capability for monitoring treatment Crohn’s disease progression and structural bowel damage,
responsiveness, but multiple barriers to implementation, has been proposed as one outcome of such trials.119,120
such as cost, availability, real-world specificity, and
tolerability have reduced its use in tight control.105,106 For Combination of advanced therapies and new approaches
serial transmural tight monitoring assessment, intestinal Despite five distinct classes of advanced therapies soon
ultrasound is emerging as a patient-centric modality. The to be available in the clinic, remission rates for all agents
10 www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2
Seminar
are plateauing at approximately 30%.121 Combining Targeting transmural healing to improve long-term outcomes
biologics has so far not provided answers. Other solutions Transmural healing confers additional benefits over
include improved patient stratification with companion mucosal healing for decreasing the risk of Crohn’s disease
biomarkers to enrich study populations. progression.130–134 Postoperative patients with Crohn’s
disease who have transmural inflammation but mucosal
Predicting response to therapies healing have increased risk of endoscopic and surgical
To date, no validated markers are available, as oncostatin recurrence.135 Patients with Crohn’s disease with evidence
M and TREM-1 have provided conflicting results to of transmural healing have reduced medication escalation,
predict anti-TNF non-response.122,123 Carrying HLA- corticosteroid use, hospitalisation, and surgery.136 It has
DQA1*05 polymorphisms was associated with an become clear that achievement of transmural healing is
increased risk of development of antibodies against anti- more readily possible today, but rates of transmural
TNF agents.124 healing in Crohn’s disease still remain low overall, at
25–42%, 1–2 years after biological therapy initiation.137–139
Diet modification to treat Crohn’s disease Contributors
In addition to potential effects on intestinal inflammation All authors contributed to the manuscript concept and design, and
and symptoms, dietary therapies also enhance the drafted, revised, and approved the final version of the manuscript.
nutritional status of patients with Crohn’s disease. The Declaration of interests
benefit of dietary therapies is evident in the preoperative MD is a consultant for Neurologica, a subsidiary of Samsung Electronics,
and Pfizer. He has received grant funding from the Helmsley Charitable
setting, in which treatment with exclusive enteral Trust. JT has received grant support from AbbVie and Janssen; payments
nutrition (EEN) shortens duration of surgery and reduces or honoraria from AbbVie, Janssen, and Pfizer; advisory board fees from
postoperative complications.125 EEN is used globally as an for AbbVie, Pfizer, and Janssen; and support for meetings or travel, or
alternative to steroids, especially in children, where it has both, from AbbVie. SV has received research support from AbbVie,
Johnson & Johnson, Pfizer, Galapagos, and Takeda; lecture fees from
a benefit over corticosteroids in improving mucosal AbbVie, Alimentiv, Arena Pharmaceuticals, AstraZeneca, Bristol Myers
inflammation.126 Although complying with a strict EEN Squibb, Ferring, Galapagos, Genentech-Roche, Gilead, Janssen, Johnson
diet is challenging, partial enteral nutrition (PEN) might & Johnson, Lilly, Materia Prima, Merck Sharp & Dohme, Pfizer, Takeda,
only be needed. When used in combination with the Tillotts Pharma, and Zealand Pharma; and consulting fees from AbbVie,
AbolerIS Pharma, AgomAb, Alimentiv, Arena Pharmaceuticals,
Crohn’s disease exclusion diet (CDED; a whole foods diet AstraZeneca, Avaxia, BMS, Boehringer Ingelheim, Celgene, CVasThera,
administered in phases attempting to limit foods that Dr Falk Pharma, Ferring, Galapagos, Genentech-Roche, Gilead, GSK,
alter the microbiome or intestinal barrier), PEN plus Hospira, Imidomics, Janssen, Johnson & Johnson, Lilly, Materia Prima,
CDED was superior to EEN alone in inducing clinical MiroBio, Morphic, MrMHealth, Mundipharma Merck, Pfizer, Prodigest,
Progenity, Prometheus, Robarts Clinical Trials, Second Genome, Shire,
remission and normalising CRP compared with EEN Surrozen, Takeda, Theravance, Tillots Pharma, and Zealand Pharma.
alone after 12 weeks.127 CDED alone has been shown to
Acknowledgments
have no differences in sustained or endoscopic remission We would thank academic medical illustrator Jill Gregory for her help
24 weeks after initiation combined to CDED with PEN in with the original figure design.
an open-label, pilot, randomised trial of adults.128 The References
evidence for the simple carbohydrate and Mediterranean 1 Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s
diets remains less clear.129 disease. Lancet 2017; 389: 1741–55.
2 Kuenzig ME, Fung SG, Marderfeld L, et al. Twenty-first century
trends in the global epidemiology of pediatric-onset inflammatory
bowel disease: systematic review. Gastroenterology 2022; 162: 1147–59.
Search strategy and selection criteria 3 Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and
prevalence of inflammatory bowel disease in the 21st century:
We searched for relevant manuscripts using PubMed, a systematic review of population-based studies. Lancet 2017;
390: 2769–78.
MEDLINE, and the Cochrane Library, from database inception
4 Plevris N, Lees CW. Disease monitoring in inflammatory bowel
until Sept 1, 2022. The search combined the MeSH terms disease: evolving principles and possibilities. Gastroenterology 2022;
“Crohn’s disease” and “inflammatory bowel disease” with 162: 1456–75.
subheadings “biomarkers”, “complications”, “diagnosis”, 5 Wilkens R, Dolinger M, Burisch J, Maaser C. Point-of-care testing
and home testing: pragmatic considerations for widespread
“endoscopy”, “epidemiology”, “genetics”, “imaging”, incorporation of stool tests, serum tests, and intestinal ultrasound.
“monitoring”, “pathophysiology”, “precision”, “prediction”, Gastroenterology 2022; 162: 1476–92.
“prevention”, “surveillance”, “target”, and “therapy”. 6 Shah SC, Khalili H, Chen CY, et al. Sex-based differences in the
incidence of inflammatory bowel diseases-pooled analysis of
We searched bibliographies of the included articles for population-based studies from the Asia-Pacific region.
additional references and critically reviewed all manuscripts Aliment Pharmacol Ther 2019; 49: 904–11.
considered. We then prioritised manuscripts published since 7 Shah SC, Khalili H, Gower-Rousseau C, et al. Sex-based differences
in incidence of inflammatory bowel diseases-pooled analysis of
the last version of this Seminar over the past 5 years. Where population-based studies from western countries. Gastroenterology
possible, priority was given to randomised, placebo- 2018; 155: 1079–89.
controlled trials, and meta-analyses. Relevant abstracts from 8 Alatab S, Sepanlou SG, Ikuta K, et al. The global, regional, and
national burden of inflammatory bowel disease in 195 countries and
major meetings were also considered before publication of
territories, 1990-2017: a systematic analysis for the Global Burden of
associated manuscripts. Disease Study 2017. Lancet Gastroenterol Hepatol 2020; 5: 17–30.
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 11
Seminar
9 Watermeyer G, Katsidzira L, Setshedi M, Devani S, Mudombi W, 33 Maaser C, Sturm A, Vavricka SR, et al. ECCO-ESGAR guideline for
Kassianides C. Inflammatory bowel disease in sub-Saharan Africa: diagnostic assessment in IBD part 1: initial diagnosis, monitoring
epidemiology, risk factors, and challenges in diagnosis. of known IBD, detection of complications. J Crohns Colitis 2019;
Lancet Gastroenterol Hepatol 2022; 7: 952–61. 13: 144–64.
10 Kaplan GG, Windsor JW. The four epidemiological stages in the 34 Magro F, Langner C, Driessen A, et al. European consensus on the
global evolution of inflammatory bowel disease. histopathology of inflammatory bowel disease. J Crohns Colitis 2013;
Nat Rev Gastroenterol Hepatol 2021; 18: 56–66. 7: 827–51.
11 Moller FT, Andersen V, Wohlfahrt J, Jess T. Familial risk of 35 Annese V, Daperno M, Rutter MD, et al. European evidence based
inflammatory bowel disease: a population-based cohort study consensus for endoscopy in inflammatory bowel disease.
1977–2011. Am J Gastroenterol 2015; 110: 564–71. J Crohns Colitis 2013; 7: 982–1018.
12 Cosnes J, Carbonnel F, Carrat F, Beaugerie L, Cattan S, Gendre J. 36 Feakins R, Torres J, Borralho-Nunes P, et al. ECCO topical review
Effects of current and former cigarette smoking on the clinical on clinicopathological spectrum and differential diagnosis of
course of Crohn’s disease. Aliment Pharmacol Ther 1999; 13: 1403–11. inflammatory bowel disease. J Crohns Colitis 2022; 16: 343–68.
13 Torres J, Gomes C, Jensen CB, et al. Risk factors for developing 37 Chachu KA, Osterman MT. How to diagnose and treat IBD mimics
inflammatory bowel disease within and across families with a in the refractory IBD patient who does not have IBD.
family history of IBD. J Crohns Colitis 2023; 17: 30–36. Inflamm Bowel Dis 2016; 22: 1262–74.
14 Ungaro R, Bernstein CN, Gearry R, et al. Antibiotics associated with 38 Chin AB, Kumar AS. Behcet colitis. Clin Colon Rectal Surg 2015;
increased risk of new-onset Crohn’s disease but not ulcerative 28: 99–102.
colitis: a meta-analysis. Am J Gastroenterol 2014; 109: 1728–38. 39 Ouahed J, Spencer E, Kotlarz D, et al. Very early onset inflammatory
15 Piovani D, Danese S, Peyrin-Biroulet L, Nikolopoulos GK, Lytras T, bowel disease: a clinical approach with a focus on the role of
Bonovas S. Environmental risk factors for inflammatory bowel genetics and underlying immune deficiencies. Inflamm Bowel Dis
diseases: an umbrella review of meta-analyses. Gastroenterology 2020; 26: 820–42.
2019; 157: 647–59. 40 Menees SB, Powell C, Kurlander J, Goel A, Chey WD. A meta-
16 Agrawal M, Sabino J, Frias-Gomes C, et al. Early life exposures and analysis of the utility of C-reactive protein, erythrocyte
the risk of inflammatory bowel disease: systematic review and meta- sedimentation rate, fecal calprotectin, and fecal lactoferrin to
analyses. EClinicalMedicine 2021; 36: 100884. exclude inflammatory bowel disease in adults with IBS.
17 Torres J, Hu J, Seki A, et al. Infants born to mothers with IBD Am J Gastroenterol 2015; 110: 444–54.
present with altered gut microbiome that transfers abnormalities of 41 Florin THJ, Paterson EWJ, Fowler EV, Radford-Smith GL. Clinically
the adaptive immune system to germ-free mice. Gut 2020; active Crohn’s disease in the presence of a low C-reactive protein.
69: 42–51. Scand J Gastroenterol 2006; 41: 306–11.
18 Narula N, Wong ECL, Dehghan M, et al. Association of ultra- 42 Mosli MH, Zou G, Garg SK, et al. C-reactive protein, fecal
processed food intake with risk of inflammatory bowel disease: calprotectin, and stool lactoferrin for detection of endoscopic
prospective cohort study. BMJ 2021; 374: n1554. activity in symptomatic inflammatory bowel disease patients:
19 McGovern DP, Kugathasan S, Cho JH. Genetics of inflammatory a systematic review and meta-analysis. Am J Gastroenterol 2015;
bowel diseases. Gastroenterology 2015; 149: 1163–76. 110: 802–19.
20 Ogura Y, Bonen DK, Inohara N, et al. A frameshift mutation in 43 van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for
NOD2 associated with susceptibility to Crohn’s disease. Nature 2001; screening of patients with suspected inflammatory bowel disease:
411: 603–06. diagnostic meta-analysis. BMJ 2010; 341: c3369.
21 Sartor RB. Reviews in basic and clinical gastroenterology. 44 Wright EK, Kamm MA, De Cruz P, et al. Measurement of fecal
Gastroenterology 2008; 134: 577–94. calprotectin improves monitoring and detection of recurrence of
22 Round JL, Mazmanian SK. The gut microbiota shapes intestinal Crohn’s disease after surgery. Gastroenterology 2015; 148: 938–47.
immune responses during health and disease. Nat Rev Immunol 45 Taylor SA, Mallett S, Bhatnagar G, et al. Diagnostic accuracy of
2009; 9: 313–23. magnetic resonance enterography and small bowel ultrasound for
23 Kamada N, Seo SU, Chen GY, Núñez G. Role of the gut microbiota the extent and activity of newly diagnosed and relapsed Crohn’s
in immunity and inflammatory disease. Nat Rev Immunol 2013; disease (METRIC): a multicentre trial. Lancet Gastroenterol Hepatol
13: 321–35. 2018; 3: 548–58.
24 Becker C, Neurath MF, Wirtz S. The intestinal microbiota in 46 Sævik F, Eriksen R, Eide GE, Gilja OH, Nylund K. Development
inflammatory bowel disease. ILAR J 2015; 56: 192–204. and validation of a simple ultrasound activity score for Crohn’s
disease. J Crohns Colitis 2021; 15: 115–24.
25 Maloy KJ, Powrie F. Intestinal homeostasis and its breakdown in
inflammatory bowel disease. Nature 2011; 474: 298–306. 47 Allocca M, Craviotto V, Bonovas S, et al. Predictive value of bowel
ultrasound in Crohn’s disease: a 12-month prospective study.
26 Larabi A, Barnich N, Nguyen HTT. New insights into the interplay
Clin Gastroenterol Hepatol 2022; 20: e723–40.
between autophagy, gut microbiota and inflammatory responses in
IBD. Autophagy 2020; 16: 38–51. 48 Daperno M, D’Haens G, Van Assche G, et al. Development and
validation of a new, simplified endoscopic activity score for Crohn’s
27 Rogler G, Singh A, Kavanaugh A, Rubin DT. Extraintestinal
disease: the SES-CD. Gastrointest Endosc 2004; 60: 505–12.
manifestations of inflammatory bowel disease: current concepts,
treatment, and implications for disease management. 49 Mary JY, Modigliani R. Development and validation of an
Gastroenterology 2021; 161: 1118–32. endoscopic index of the severity for Crohn’s disease: a prospective
multicentre study. Groupe d’Etudes Thérapeutiques des
28 Nóbrega VG, Silva INN, Brito BS, Silva J, da Silva MCM,
Affections Inflammatoires du Tube Digestif (GETAID). Gut 1989;
Santana GO. The onset of clinical manifestations in inflammatory
30: 983–89.
bowel disease patients. Arq Gastroenterol 2018; 55: 290–95.
50 Enns RA, Hookey L, Armstrong D, et al. Clinical practice guidelines
29 Yu YR, Rodriguez JR. Clinical presentation of Crohn’s, ulcerative
for the use of video capsule endoscopy. Gastroenterology 2017;
colitis, and indeterminate colitis: symptoms, extraintestinal
152: 497–514.
manifestations, and disease phenotypes. Semin Pediatr Surg 2017;
26: 349–55. 51 Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated
clinical, molecular and serological classification of inflammatory
30 Panés J, Rimola J. Perianal fistulizing Crohn’s disease:
bowel disease: report of a Working Party of the 2005 Montreal
pathogenesis, diagnosis and therapy. Nat Rev Gastroenterol Hepatol
World Congress of Gastroenterology. Can J Gastroenterol. 2005;
2017; 14: 652–64.
19: 5A–36A.
31 Tsai L, McCurdy JD, Ma C, Jairath V, Singh S. Epidemiology and
52 Levine A, Griffiths A, Markowitz J, et al. Pediatric modification of
natural history of perianal Crohn’s disease: a systematic review and
the Montreal classification for inflammatory bowel disease:
meta-analysis of population-based cohorts. Inflamm Bowel Dis 2022;
the Paris classification. Inflamm Bowel Dis 2011; 17: 1314–21.
28: 1477–84.
53 Ordás I, Feagan BG, Sandborn WJ. Early use of
32 Gecse KB, Vermeire S. Differential diagnosis of inflammatory
immunosuppressives or TNF antagonists for the treatment of
bowel disease: imitations and complications.
Crohn’s disease: time for a change. Gut 2011; 60: 1754–63.
Lancet Gastroenterol Hepatol 2018; 3: 644–53.
12 www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2
Seminar
54 Sandborn WJ, Hanauer S, Van Assche G, et al. Treating beyond 75 Lemaitre M, Kirchgesner J, Rudnichi A, et al. Association between
symptoms with a view to improving patient outcomes in use of thiopurines or tumor necrosis factor antagonists alone or in
inflammatory bowel diseases. J Crohns Colitis 2014; 8: 927–35. combination and risk of lymphoma in patients with inflammatory
55 Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: an update on the bowel disease. JAMA 2017; 318: 1679–86.
selecting therapeutic targets in inflammatory bowel disease 76 Sandborn WJ, Feagan BG, Rutgeerts P, et al. Vedolizumab as
(STRIDE) initiative of the International Organization for the Study induction and maintenance therapy for Crohn’s disease.
of IBD (IOIBD): determining therapeutic goals for treat-to-target N Engl J Med 2013; 369: 711–21.
strategies in IBD. Gastroenterology 2021; 160: 1570–83. 77 Sandborn WJ, Vermeire S, Tyrrell H, et al. Etrolizumab for the
56 Ben-Horin S, Novack L, Mao R, et al. Efficacy of biologic drugs in treatment of ulcerative colitis and Crohn’s disease: an overview of
short-duration versus long-duration inflammatory bowel disease: the phase 3 clinical program. Adv Ther 2020; 37: 3417–31.
a systematic review and an individual-patient data meta-analysis of 78 Sandborn WJ, Lee SD, Tarabar D, et al. Phase II evaluation of
randomized controlled trials. Gastroenterology 2022; 162: 482–94. anti-MAdCAM antibody PF-00547659 in the treatment of Crohn’s
57 Torres J, Bonovas S, Doherty G, et al. ECCO guidelines on disease: report of the OPERA study. Gut 2018; 67: 1824–35.
therapeutics in Crohn’s disease: medical treatment. J Crohns Colitis 79 Feagan BG, Sandborn WJ, Gasink C, et al. Ustekinumab as
2020; 14: 4–22. induction and maintenance therapy for Crohn’s disease.
58 Malchow H, Ewe K, Brandes JW, et al. European Cooperative N Engl J Med 2016; 375: 1946–60.
Crohn’s Disease Study (ECCDS): results of drug treatment. 80 D’Haens G, Panaccione R, Baert F, et al. Risankizumab as
Gastroenterology 1984; 86: 249–66. induction therapy for Crohn’s disease: results from the phase 3
59 Summers RW, Switz DM, Sessions JT Jr, et al. National Cooperative ADVANCE and MOTIVATE induction trials. Lancet 2022;
Crohn’s Disease Study: results of drug treatment. Gastroenterology 399: 2015–30.
1979; 77: 847–69. 81 Ferrante M, Panaccione R, Baert F, et al. Risankizumab as
60 Vuyyuru SK, Solitano V, Hogan M, et al. Efficacy and safety of maintenance therapy for moderately to severely active Crohn’s
IL-12/23 and IL-23 inhibitors for Crohn’s disease: systematic review disease: results from the multicentre, randomised, double-blind,
and meta-analysis. Dig Dis Sci 2023; 68: 3702–13. placebo-controlled, withdrawal phase 3 FORTIFY maintenance trial.
61 Solitano V, Vuyyuru SK, MacDonald JK, et al. Efficacy and safety Lancet 2022; 399: 2031–46.
of oral small molecules for inflammatory bowel disease: 82 Sandborn WJ, D’Haens GR, Reinisch W, et al. Guselkumab for the
systematic review and meta-analysis. J Crohns Colitis 2023; treatment of Crohn’s disease: induction results from the phase 2
17: 1800–16. GALAXI-1 study. Gastroenterology 2022; 162: 1650–64.
62 Dewint P, Hansen BE, Verhey E, et al. Adalimumab combined with 83 Sands BE, Peyrin-Biroulet L, Kierkus J, et al. Efficacy and safety of
ciprofloxacin is superior to adalimumab monotherapy in perianal mirikizumab in a randomized phase 2 study of patients with
fistula closure in Crohn’s disease: a randomised, double-blind, Crohn’s disease. Gastroenterology 2022; 162: 495–508.
placebo controlled trial (ADAFI). Gut 2014; 63: 292–99. 84 Sandborn WJ, Feagan BG, Loftus EV Jr, et al. Efficacy and safety of
63 Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, upadacitinib in a randomized trial of patients with Crohn’s disease.
azathioprine, or combination therapy for Crohn’s disease. Gastroenterology 2020; 158: 2123–38.
N Engl J Med 2010; 362: 1383–95. 85 Vermeire S, Schreiber S, Petryka R, et al. Clinical remission in
64 Panés J, López-Sanromán A, Bermejo F, et al. Early azathioprine patients with moderate-to-severe Crohn’s disease treated with
therapy is no more effective than placebo for newly diagnosed filgotinib (the FITZROY study): results from a phase 2, double-
Crohn’s disease. Gastroenterology 2013; 145: 766–74. blind, randomised, placebo-controlled trial. Lancet 2017;
65 Cosnes J, Bourrier A, Laharie D, et al. Early administration of 389: 266–75.
azathioprine vs conventional management of Crohn’s disease: 86 Loftus EV, Panes J, Lacerda AP et al. Upadacitinib induction and
a randomized controlled trial. Gastroenterology 2013; 145: 758–65. maintenance therapy for Crohn’s disease. N Engl J Med 2023;
66 Kennedy NA, Heap GA, Green HD, et al. Predictors of anti-TNF 388: 1966–80.
treatment failure in anti-TNF-naive patients with active luminal 87 Sands BE, Irving PM, Hoops T, et al. Ustekinumab versus
Crohn’s disease: a prospective, multicentre, cohort study. adalimumab for induction and maintenance therapy in biologic-I
Lancet Gastroenterol Hepatol 2019; 4: 341–53. patients with moderately to severely active Crohn’s disease:
67 Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance a multicentre, randomised, double-blind, parallel-group, phase 3b
therapy for fistulizing Crohn’s disease. N Engl J Med 2004; 350: 876–85. trial. Lancet 2022; 399: 2200–11.
68 Colombel JF, Schwartz DA, Sandborn WJ, et al. Adalimumab for 88 Barberio B, Gracie DJ, Black CJ, Ford AC. Efficacy of biological
the treatment of fistulas in patients with Crohn’s disease. Gut 2009; therapies and small molecules in induction and maintenance of
58: 940–48. remission in luminal Crohn’s disease: systematic review and
69 Bouhnik Y, Carbonnel F, Laharie D, et al. Efficacy of adalimumab in network meta-analysis. Gut 2023; 72: 264–74.
patients with Crohn’s disease and symptomatic small bowel 89 Adamina M, Bonovas S, Raine T, et al. ECCO guidelines on
stricture: a multicentre, prospective, observational cohort (CREOLE) therapeutics in Crohn’s disease: surgical treatment. J Crohns Colitis
study. Gut 2018; 67: 53–60. 2020; 14: 155–68.
70 Regueiro M, Schraut W, Baidoo L, et al. Infliximab prevents Crohn’s 90 Ponsioen CY, de Groof EJ, Eshuis EJ, et al. Laparoscopic ileocaecal
disease recurrence after ileal resection. Gastroenterology 2009; resection versus infliximab for terminal ileitis in Crohn’s disease:
136: 441–50. a randomised controlled, open-label, multicentre trial. Lancet
71 Mahadevan U, Long MD, Kane SV, et al. Pregnancy and neonatal Gastroenterol Hepatol 2017; 2: 785–92.
outcomes after fetal exposure to biologics and thiopurines among 91 Stevens TW, Haasnoot ML, D’Haens GR, et al. Laparoscopic
women with inflammatory bowel disease. Gastroenterology 2021; ileocaecal resection versus infliximab for terminal ileitis in Crohn’s
160: 1131–39. disease: retrospective long-term follow-up of the LIR!C trial. Lancet
72 Singh S, Facciorusso A, Dulai PS, Jairath V, Sandborn WJ. Gastroenterol Hepatol 2020; 5: 900–07.
Comparative risk of serious infections with biologic and/or 92 Shen B, Kochhar G, Navaneethan U, et al. Practical guidelines on
immunosuppressive therapy in patients with inflammatory bowel endoscopic treatment for Crohn’s disease strictures: a consensus
diseases: a systematic review and meta-analysis. statement from the Global Interventional Inflammatory Bowel
Clin Gastroenterol Hepatol 2020; 18: 69–81. Disease Group. Lancet Gastroenterol Hepatol 2020; 5: 393–405.
73 Xie W, Xiao S, Huang H, Zhang Z. Incidence of and risk factors for 93 Holubar SD, Gunter RL, Click BH, et al. Mesenteric excision and
paradoxical psoriasis or psoriasiform lesions in inflammatory bowel exclusion for ileocolic Crohn’s disease: feasibility and safety of an
disease patients receiving anti-TNF therapy: systematic review with innovative, combined surgical approach with extended mesenteric
meta-analysis. Front Immunol 2022; 13: 847160. excision and Kono-S anastomosis. Dis Colon Rectum 2022; 65: e5–13.
74 Kirchgesner J, Lemaitre M, Carrat F, Zureik M, Carbonnel F, 94 Luglio G, Rispo A, Imperatore N, et al. Surgical prevention of
Dray-Spira R. Risk of serious and opportunistic infections anastomotic recurrence by excluding mesentery in Crohn’s disease:
associated with treatment of inflammatory bowel diseases. the SuPREMe-CD study – a randomized clinical trial. Ann Surg
Gastroenterology 2018; 155: 337–46. 2020; 272: 210–17.
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 13
Seminar
95 Neuendorf R, Harding A, Stello N, Hanes D, Wahbeh H. 113 Lee SH, Turpin W, Espin-Garcia O, et al. Anti-microbial antibody
Depression and anxiety in patients with inflammatory bowel response is associated with future onset of Crohn’s disease
disease: a systematic review. J Psychosom Res 2016; 87: 70–80. independent of biomarkers of altered gut barrier function,
96 Taft TH, Ballou S, Bedell A, Lincenberg D. Psychological subclinical inflammation, and genetic risk. Gastroenterology 2021;
considerations and interventions in inflammatory bowel disease 161: 1540–51.
patient care. Gastroenterol Clin North Am 2017; 46: 847–58. 114 Turpin W, Lee SH, Raygoza Garay JA, et al. Increased intestinal
97 D’Silva A, Fox DE, Nasser Y, et al. Prevalence and risk factors for permeability is associated with later development of Crohn’s
fatigue in adults with inflammatory bowel disease: a systematic disease. Gastroenterology 2020; 159: 2092–100.
review with meta-analysis. Clin Gastroenterol Hepatol 2022; 115 Kugathasan S, Denson LA, Walters TD, et al. Prediction of
20: 995–1009. complicated disease course for children newly diagnosed with
98 Czuber-Dochan W, Morgan M, Hughes LD, Lomer MCE, Crohn’s disease: a multicentre inception cohort study. Lancet 2017;
Lindsay JO, Whelan K. Perceptions and psychosocial impact of 389: 1710–18.
food, nutrition, eating and drinking in people with inflammatory 116 Lee JC, Lyons PA, McKinney EF, et al. Gene expression profiling of
bowel disease: a qualitative investigation of food-related quality of CD8+ T cells predicts prognosis in patients with Crohn disease and
life. J Hum Nutr Diet 2020; 33: 115–27. ulcerative colitis. J Clin Invest 2011; 121: 4170–79.
99 Drossman DA, Leserman J, Li ZM, Mitchell CM, Zagami EA, 117 Parkes M, Noor NM, Dowling F, et al. predicting outcomes for
Patrick DL. The rating form of IBD patient concerns: a new Crohn’s disease using a molecular biomarker (PROFILE): protocol
measure of health status. Psychosom Med 1991; 53: 701–12. for a multicentre, randomised, biomarker-stratified trial. BMJ Open
100 Knowles SR, Monshat K, Castle DJ. The efficacy and 2018; 8: e026767.
methodological challenges of psychotherapy for adults with 118 Le Berre C, Peyrin-Biroulet L, Sandborn WJ, et al. Selecting end
inflammatory bowel disease: a review. Inflamm Bowel Dis 2013; points for disease-modification trials in inflammatory bowel
19: 2704–15. disease: the SPIRIT consensus from the IOIBD. Gastroenterology
101 Lo B, Vind I, Vester-Andersen MK, Bendtsen F, Burisch J. Direct 2021; 160: 1452–60.
and indirect costs of inflammatory bowel disease: ten years of 119 Pariente B, Mary JY, Danese S, et al. Development of the Lémann
follow-up in a Danish population-based inception cohort. index to assess digestive tract damage in patients with Crohn’s
J Crohns Colitis 2020; 14: 53–63. disease. Gastroenterology 2015; 148: 52–63.
102 Colombel JF, Panaccione R, Bossuyt P, et al. Effect of tight control 120 Pariente B, Torres J, Burisch J, et al. Validation and update of the
management on Crohn’s disease (CALM): a multicentre, Lémann index to measure cumulative structural bowel damage in
randomised, controlled phase 3 trial. Lancet 2017; 390: 2779–89. Crohn’s disease. Gastroenterology 2021; 161: 853–64.
103 Danese S, Vermeire S, D’Haens G, et al. Treat to target versus 121 Kayal M, Ungaro RC, Bader G, Colombel JF, Sandborn WJ, Stalgis
standard of care for patients with Crohn’s disease treated with C. Net remission rates with biologic treatment in Crohn’s disease:
ustekinumab (STARDUST): an open-label, multicentre, a reappraisal of the clinical trial data. Clin Gastroenterol Hepatol
randomised phase 3b trial. Lancet Gastroenterol Hepatol 2022; 2023; 21: 1348–50.
7: 294–306. 122 West NR, Hegazy AN, Owens BMJ, et al. Oncostatin M drives
104 Jairath V, Khanna R, Guizetti L, et al. A cluster randomized intestinal inflammation and predicts response to tumor necrosis
controlled trial of enhanced treatment algorithm for the factor-neutralizing therapy in patients with inflammatory bowel
management of Crohn’s disease: REACT-2. disease. Nat Med 2017; 23: 579–89.
United European Gastroenterol J 2022; 10: 89. 123 Verstockt B, Verstockt S, Dehairs J, et al. Low TREM1 expression in
105 Hanžel J, Jairath V, Ma C, et al. Responsiveness of magnetic whole blood predicts anti-TNF response in inflammatory bowel
resonance enterography indices for evaluation of luminal disease disease. EbioMedicine 2019; 40: 733–42.
activity in Crohn’s disease. Clin Gastroenterol Hepatol 2022; 124 Sazonovs A, Kennedy NA, Moutsianas L, et al. HLA-DQA1*05
20: 2598–606. carriage associated with development of anti-drug antibodies to
106 Kumar S, Parry T, Mallett S, et al. Diagnostic performance of infliximab and adalimumab in patients with Crohn’s disease.
magnetic resonance enterography disease activity indices compared Gastroenterology 2020; 158: 189–99.
with a histological reference standard for adult terminal ileal 125 Heerasing N, Thompson B, Hendy P, et al. Exclusive enteral
Crohn’s disease: experience from the METRIC trial. J Crohns Colitis nutrition provides an effective bridge to safer interval elective
2022; 16: 1531–39. surgery for adults with Crohn’s disease. Aliment Pharmacol Ther
107 Kucharzik T, Wittig BM, Helwig U, et al. Use of intestinal 2017; 45: 660–69.
ultrasound to monitor Crohn’s disease activity. Clin Gastroenterol 126 Borrelli O, Cordischi L, Cirulli M, et al. Polymeric diet alone versus
Hepatol 2017; 15: 535–42. corticosteroids in the treatment of active pediatric Crohn’s disease:
108 Calabrese E, Rispo A, Zorzi F, et al. Ultrasonography tight control a randomized controlled open-label trial. Clin Gastroenterol Hepatol
and monitoring in Crohn’s disease during different biological 2006; 4: 744–53.
therapies: a multicenter study. Clin Gastroenterol Hepatol 2022; 127 Levine A, Wine E, Assa A, et al. Crohn’s disease exclusion diet plus
20: e711–22. partial enteral nutrition induces sustained remission in a
108 Dillman JR, Dehkordy SF, Smith EA, et al. Defining the randomized controlled trial. Gastroenterology 2019; 157: 440–50.
ultrasound longitudinal natural history of newly diagnosed 128 Yanai H, Levine A, Hirsch A, et al. The Crohn’s disease exclusion
pediatric small bowel Crohn disease treated with infliximab and diet for induction and maintenance of remission in adults with
infliximab-azathioprine combination therapy. Pediatr Radiol 2017; mild-to-moderate Crohn’s disease (CDED-AD): an open-label,
47: 924–34. pilot, randomised trial. Lancet Gastroenterol Hepatol 2022;
109 de Voogd F, Bots S, Gecse K, Gilja OH, D’Haens G, Nylund K. 7: 49–59.
Intestinal ultrasound early on in treatment follow-up predicts 129 Lewis JD, Sandler RS, Brotherton C, et al. A randomized trial
endoscopic response to anti-TNFα treatment in Crohn’s Disease. comparing the specific carbohydrate diet to a mediterranean diet in
J Crohns Colitis 2022; 16: 1598–608. adults with Crohn’s disease. Gastroenterology 2021; 161: 837–52.
110 Torres J, Halfvarson J, Rodríguez-Lago I, et al. Results of the 130 Deepak P, Fletcher JG, Fidler JL, et al. Radiological response is
Seventh Scientific Workshop of ECCO: precision medicine in associated with better long-term outcomes and is a potential
IBD-prediction and prevention of inflammatory bowel disease. treatment target in patients with small bowel Crohn’s disease.
J Crohns Colitis 2021; 15: 1443–54. Am J Gastroenterol 2016; 111: 997–1006.
111 Torres J, Petralia F, Sato T, et al. Serum biomarkers identify patients 131 Fernandes SR, Rodrigues RV, Bernardo S, et al. Transmural healing
who will develop inflammatory bowel diseases up to 5 years before is associated with improved long-term outcomes of patients with
diagnosis. Gastroenterology 2020; 159: 96–104. Crohn’s disease. Inflamm Bowel Dis 2017; 23: 1403–09.
112 Mortha A, Remark R, Del Valle DM, et al. Neutralizing anti-GM- 132 Castiglione F, Imperatore N, Testa A, et al. One-year clinical
CSF autoantibodies recognize posttranslational glycosylations on outcomes with biologics in Crohn’s disease: transmural healing
GM-CSF years prior to diagnosis and predict complicated Crohn’s compared with mucosal or no healing. Aliment Pharmacol Ther 2019;
disease. Gastroenterology 2022; 163: 659–70. 49: 1026–39.
14 www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2
Seminar
133 Hallé E, Azahaf M, Duveau N, et al. Radiological response is 137 Castiglione F, Testa A, Rea M, et al. Transmural healing evaluated
associated with better outcomes and should be considered a by bowel sonography in patients with Crohn’s disease on
therapeutic target in Crohn’s disease. Dig Dis Sci 2020; maintenance treatment with biologics. Inflamm Bowel Dis 2013;
65: 2664–74. 19: 1928–34.
134 Lafeuille P, Hordonneau C, Vignette J, et al. Transmural healing 138 Castiglione F, Mainenti P, Testa A, et al. Cross-sectional evaluation
and MRI healing are associated with lower risk of bowel damage of transmural healing in patients with Crohn’s disease on
progression than endoscopic mucosal healing in Crohn’s disease. maintenance treatment with anti-TNF alpha agents. Dig Liver Dis
Aliment Pharmacol Ther 2021; 53: 577–86. 2017; 49: 484–89.
135 Bachour SP, Shah RS, Lyu R, et al. Test characteristics of cross- 139 Paredes JM, Moreno N, Latorre P, et al. Clinical impact of
sectional imaging and concordance with endoscopy in postoperative sonographic transmural healing after anti-TNF antibody treatment
Crohn’s disease. Clin Gastroenterol Hepatol 2022; 20: 2327–36. in patients with Crohn’s disease. Dig Dis Sci 2019; 64: 2600–06.
136 Vaughan R, Tjandra D, Patwardhan A, et al. Toward transmural
healing: sonographic healing is associated with improved long-term Copyright © 2024 Elsevier Ltd. All rights reserved.
outcomes in patients with Crohn’s disease. Aliment Pharmacol Ther
2022; 56: 84–94.
www.thelancet.com Published online March 1, 2024 https://doi.org/10.1016/S0140-6736(23)02586-2 15
You might also like
- How To Make An Effective PowerPoint PresentationDocument12 pagesHow To Make An Effective PowerPoint PresentationZach Hansen100% (1)
- Ulcerative ColitisDocument8 pagesUlcerative ColitispipotoNo ratings yet
- BS 215-2-1970-Aluminium Conductors and Aluminium Conductors Steel-Reinforced For Overhead Power TransmissionDocument16 pagesBS 215-2-1970-Aluminium Conductors and Aluminium Conductors Steel-Reinforced For Overhead Power TransmissionDayan Yasaranga100% (2)
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Learning Module - Joints, Taps and SplicesDocument9 pagesLearning Module - Joints, Taps and SplicesCarlo Cartagenas100% (1)
- School Clinic Action PlanDocument2 pagesSchool Clinic Action PlanAlera Kim100% (7)
- Ulcerative ColitisDocument13 pagesUlcerative ColitisAlis GomezNo ratings yet
- Boala Crohn La Copil: Crohn's Disease in ChildrenDocument14 pagesBoala Crohn La Copil: Crohn's Disease in ChildrenFranceska FilippiNo ratings yet
- Crohn Review Lancet 2017Document15 pagesCrohn Review Lancet 2017Medicina UFU 92No ratings yet
- Seminar: Joana Torres, Saurabh Mehandru, Jean-Frédéric Colombel, Laurent Peyrin-BirouletDocument15 pagesSeminar: Joana Torres, Saurabh Mehandru, Jean-Frédéric Colombel, Laurent Peyrin-BirouletKaren ojedaNo ratings yet
- Ungaro2016 PDFDocument15 pagesUngaro2016 PDFAbraham SalvadorNo ratings yet
- Pohon Masalah AnsietasDocument16 pagesPohon Masalah AnsietasDeva NatarummandaNo ratings yet
- A Review of Crohn's Disease: Pathophysiology, Genetics, Immunology, Environmental Factors, Clinical Presentation, Diagnosis, ManagementDocument18 pagesA Review of Crohn's Disease: Pathophysiology, Genetics, Immunology, Environmental Factors, Clinical Presentation, Diagnosis, ManagementValentina RodriguezNo ratings yet
- Crohn 1 EspDocument8 pagesCrohn 1 EspRomina GonzálezNo ratings yet
- A Review of Crohn's DiseaseDocument8 pagesA Review of Crohn's DiseaseSalwiyadiNo ratings yet
- 1 s2.0 S0140673623009662 MainDocument14 pages1 s2.0 S0140673623009662 MainKesia MaldonadoNo ratings yet
- Bmri2013 297501Document11 pagesBmri2013 297501tiaraNo ratings yet
- Hypokalemia, Can Be A Cause of Ileus and Should be-WT - SummariesDocument11 pagesHypokalemia, Can Be A Cause of Ileus and Should be-WT - SummariesLiav KfirNo ratings yet
- Crohns Epidemio Diagnositco y TratamientoDocument16 pagesCrohns Epidemio Diagnositco y TratamientoSantiago ZamudioNo ratings yet
- Nanoparticle-Mediated-Therapeutic-Approach-for-Ulcerative-Colitis-TreatmentDocument22 pagesNanoparticle-Mediated-Therapeutic-Approach-for-Ulcerative-Colitis-TreatmentAchudan JiiNo ratings yet
- Antibiotic Therapy and Risk of Early-Onset Colorectal Cancer: A National Case-Control StudyDocument8 pagesAntibiotic Therapy and Risk of Early-Onset Colorectal Cancer: A National Case-Control StudyMohammed KhalidNo ratings yet
- Risk Predictors of Progression To Severe Disease of DengueDocument13 pagesRisk Predictors of Progression To Severe Disease of DengueTaufiqurrokhman RofiiNo ratings yet
- Pathophysiology of IBDDocument11 pagesPathophysiology of IBDOktarina Heni SunandarNo ratings yet
- Pancreatic Tuberculosis Review ArticleDocument24 pagesPancreatic Tuberculosis Review ArticlesamudraandiNo ratings yet
- Rcuh PDFDocument27 pagesRcuh PDFicoanamareNo ratings yet
- HHS Public AccessDocument22 pagesHHS Public AccessZakirNo ratings yet
- Approach To The Management of Recently Diagnosed IDocument19 pagesApproach To The Management of Recently Diagnosed IdudinkarulesNo ratings yet
- 4019.NEJM, GastroentDocument11 pages4019.NEJM, Gastroentbrian.p.lucasNo ratings yet
- [03241750 - Acta Medica Bulgarica] Extraintestinal Manifestations and Intestinal Complications in Patients with Crohn's Disease_ Associations with Some Clinico-Laboratory Findings, Immunological Markers and Therapy.pdfDocument6 pages[03241750 - Acta Medica Bulgarica] Extraintestinal Manifestations and Intestinal Complications in Patients with Crohn's Disease_ Associations with Some Clinico-Laboratory Findings, Immunological Markers and Therapy.pdfTeodorNo ratings yet
- Elife 79397 v2Document21 pagesElife 79397 v2lata.pauccaraNo ratings yet
- Inflamatory Bowel Disease: Dr. Samir IsmailDocument82 pagesInflamatory Bowel Disease: Dr. Samir IsmailGhadeer EbraheemNo ratings yet
- Endo 1Document7 pagesEndo 1Soulseller1983No ratings yet
- Nihms 1688237Document20 pagesNihms 1688237Mohammed KhalidNo ratings yet
- Fenotipo IBDDocument9 pagesFenotipo IBDMaria FannyNo ratings yet
- ECCO-manage Infections in IBD2021Document35 pagesECCO-manage Infections in IBD2021Ramez AntakiaNo ratings yet
- Healthmed 15 1 Damir SecicDocument6 pagesHealthmed 15 1 Damir SecicEdoHNo ratings yet
- CA Colon OncologyDocument8 pagesCA Colon OncologyAgstri Dwi MarselaNo ratings yet
- Epidemiologyand Pathogenesisofulcerative Colitis: Lillian Du,, Christina HaDocument12 pagesEpidemiologyand Pathogenesisofulcerative Colitis: Lillian Du,, Christina HaVinicius BalanNo ratings yet
- Colitis UlcerativaDocument20 pagesColitis UlcerativaMargareth Vargas BéjarNo ratings yet
- CoinfectionDocument13 pagesCoinfectionabznaim420No ratings yet
- 2340-Article Text-6948-6-10-20230531Document9 pages2340-Article Text-6948-6-10-20230531Don SarNo ratings yet
- Shingadia 2003Document9 pagesShingadia 2003syifa fileNo ratings yet
- 10.1038@s41572 020 0205 XDocument20 pages10.1038@s41572 020 0205 XJesús Cortés HernándezNo ratings yet
- TB SleDocument11 pagesTB SlePulmonologi Dan Kedokteran Respirasi FK UNRINo ratings yet
- Adenosine Role in CancerDocument21 pagesAdenosine Role in CancerPilar AufrastoNo ratings yet
- Cholelithiasis For ChildrenDocument9 pagesCholelithiasis For ChildrenAgustina TambingNo ratings yet
- Definitions, Epidemiology, and Risk Factors For Inflammatory Bowel Disease - UpToDateDocument25 pagesDefinitions, Epidemiology, and Risk Factors For Inflammatory Bowel Disease - UpToDateTurma A 2019.1 Med-FCMNo ratings yet
- Enfermedad de CrohnDocument16 pagesEnfermedad de CrohnFabrizzio BardalesNo ratings yet
- Extraintestinal Focal Infections in Adults With Nontyphoid Salmonella 2006Document10 pagesExtraintestinal Focal Infections in Adults With Nontyphoid Salmonella 2006Carlos Antonio Arrieta NieblesNo ratings yet
- Celiac DiseaseDocument14 pagesCeliac Diseasebibhutimah02No ratings yet
- Isolated Crohn's Disease of The Appendix - A Rare DisorderDocument5 pagesIsolated Crohn's Disease of The Appendix - A Rare DisorderСергей СадовниковNo ratings yet
- Last Sci Pape001Document8 pagesLast Sci Pape001Mark MartinNo ratings yet
- Acute Pyelonephritis in PregnancyDocument7 pagesAcute Pyelonephritis in PregnancyKvmLlyNo ratings yet
- Pone 0228256Document17 pagesPone 0228256Azzahra ZaydNo ratings yet
- Global Prevalence of Norovirus in Cases of Gastroenteritis: A Systematic Review and Meta-AnalysisDocument6 pagesGlobal Prevalence of Norovirus in Cases of Gastroenteritis: A Systematic Review and Meta-AnalysisSeruni Allisa AslimNo ratings yet
- Role of Bacterial Infections in Pancreatic Cancer: ReviewDocument5 pagesRole of Bacterial Infections in Pancreatic Cancer: ReviewZilbran BerontaxNo ratings yet
- Clinicopathological Profile and Surgical Treatment of Abdominal Tuberculosis: A Single Centre Experience in Northwestern TanzaniaDocument9 pagesClinicopathological Profile and Surgical Treatment of Abdominal Tuberculosis: A Single Centre Experience in Northwestern TanzaniaDala VWNo ratings yet
- Colitis PDFDocument11 pagesColitis PDFicoanamareNo ratings yet
- Clostridium Difficile Infection and Fecal BacteriotherapyDocument9 pagesClostridium Difficile Infection and Fecal BacteriotherapyAnonymous nEC4alrPjGNo ratings yet
- Inflammatory Bowel DiseaseDocument37 pagesInflammatory Bowel DiseaseDrTushar GoswamiNo ratings yet
- Artikel Rotaviruses FinalDocument30 pagesArtikel Rotaviruses Finalsemangat pagiNo ratings yet
- Acute Diare DiaseseDocument9 pagesAcute Diare DiaseseAnonymous l3X3jf0NPNo ratings yet
- Perera2018 Article NLRP3InflammasomeInColitisADocument14 pagesPerera2018 Article NLRP3InflammasomeInColitisAValean DanNo ratings yet
- Inflammatory Potential of Diet and Risk of Colorectal Cancer A Casecontrol Study From ItalyDocument7 pagesInflammatory Potential of Diet and Risk of Colorectal Cancer A Casecontrol Study From ItalyHenrique VidalNo ratings yet
- Rolling TechnologyDocument4 pagesRolling TechnologyFrancis Erwin Bernard100% (1)
- ProjectDocument22 pagesProjectSayan MondalNo ratings yet
- Sidomuncul20190313064235169 1 PDFDocument298 pagesSidomuncul20190313064235169 1 PDFDian AnnisaNo ratings yet
- Exercise-3 (B) : Linear EquationsDocument3 pagesExercise-3 (B) : Linear EquationsVRUSHABHNo ratings yet
- Black Hole Safety Brochure Trifold FinalDocument2 pagesBlack Hole Safety Brochure Trifold Finalvixy1830No ratings yet
- Wood ReportDocument36 pagesWood Reportメルヴリッ クズルエタNo ratings yet
- Beng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtDocument9 pagesBeng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtMarcelo BaptistaNo ratings yet
- MikoritkDocument6 pagesMikoritkChris Jonathan Showip RouteNo ratings yet
- Retailing PPT (Shailwi Nitish)Document14 pagesRetailing PPT (Shailwi Nitish)vinit PatidarNo ratings yet
- USTH Algorithm RecursionDocument73 pagesUSTH Algorithm Recursionnhng2421No ratings yet
- Phenomenology of The SelfDocument5 pagesPhenomenology of The SelfGuilherme CastelucciNo ratings yet
- ITCNASIA23 - Visitor GuideDocument24 pagesITCNASIA23 - Visitor Guideibrahim shabbirNo ratings yet
- Java Edition Data Values - Official Minecraft WikiDocument140 pagesJava Edition Data Values - Official Minecraft WikiCristian Rene SuárezNo ratings yet
- Pepperberg Notes On The Learning ApproachDocument3 pagesPepperberg Notes On The Learning ApproachCristina GherardiNo ratings yet
- Case Study Managerial EconomicsDocument4 pagesCase Study Managerial EconomicsZaza Afiza100% (1)
- Work Permits New Guideline Amendments 2021 23.11.2021Document7 pagesWork Permits New Guideline Amendments 2021 23.11.2021Sabrina BrathwaiteNo ratings yet
- Southern California International Gateway Final Environmental Impact ReportDocument40 pagesSouthern California International Gateway Final Environmental Impact ReportLong Beach PostNo ratings yet
- Rwamagana s5 Mathematics CoreDocument4 pagesRwamagana s5 Mathematics Coreevariste.ndungutse1493No ratings yet
- LP MAPEH 10 1st Quarter Printing Final.Document29 pagesLP MAPEH 10 1st Quarter Printing Final.tatineeesamonteNo ratings yet
- Technical DescriptionDocument2 pagesTechnical Descriptioncocis_alexandru04995No ratings yet
- Portfolio Final AssignmentDocument2 pagesPortfolio Final Assignmentkaz7878No ratings yet
- Net Pert: Cable QualifierDocument4 pagesNet Pert: Cable QualifierAndrés Felipe Fandiño MNo ratings yet
- Measures For FloodsDocument4 pagesMeasures For FloodsMutsitsikoNo ratings yet
- Teambinder Product BrochureDocument7 pagesTeambinder Product BrochurePrinceNo ratings yet
- Master Data FileDocument58 pagesMaster Data Fileinfo.glcom5161No ratings yet
- Oral Com Reviewer 1ST QuarterDocument10 pagesOral Com Reviewer 1ST QuarterRaian PaderesuNo ratings yet




























![[03241750 - Acta Medica Bulgarica] Extraintestinal Manifestations and Intestinal Complications in Patients with Crohn's Disease_ Associations with Some Clinico-Laboratory Findings, Immunological Markers and Therapy.pdf](https://imgv2-2-f.scribdassets.com/img/document/472637710/149x198/2a81753cb8/1597598960?v=1)