You might also like
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternEna Katherine CanonoNo ratings yet
- UntitledDocument4 pagesUntitledPie CanapiNo ratings yet
- The Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1From EverandThe Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1Rating: 5 out of 5 stars5/5 (1)
- Nursing Care Plan (Pedia)Document5 pagesNursing Care Plan (Pedia)JA BerzabalNo ratings yet
- The Basic Breathwork Book: A Fundamental Guide to Enhancing Health, Performance and MindfulnessFrom EverandThe Basic Breathwork Book: A Fundamental Guide to Enhancing Health, Performance and MindfulnessNo ratings yet
- NCP For LEC Act. 5Document1 pageNCP For LEC Act. 5Keneth Dave AglibutNo ratings yet
- Basics and modern practice of nasal high-flow therapyFrom EverandBasics and modern practice of nasal high-flow therapyRating: 5 out of 5 stars5/5 (1)
- NCP PCAPDocument9 pagesNCP PCAPCarl Simon CalingacionNo ratings yet
- Goal:: Ineffective Airway Clearance Related To Cumulation of SecretionDocument4 pagesGoal:: Ineffective Airway Clearance Related To Cumulation of SecretionWyen CabatbatNo ratings yet
- Nursing Care Plan in Pedia Ward: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan in Pedia Ward: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationCharlynne AraojoNo ratings yet
- AssessmentDocument7 pagesAssessmentJeenah HannahNo ratings yet
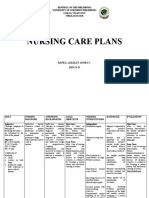
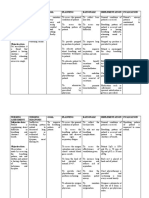
- Nursing Care Plans: Republic of The Philippines University of Northern Philippines Tamag, Vigan City 2700 Ilocos SurDocument6 pagesNursing Care Plans: Republic of The Philippines University of Northern Philippines Tamag, Vigan City 2700 Ilocos SurNo EulNo ratings yet
- Cebu Institute of Technology - University: Nursing Care PlanDocument2 pagesCebu Institute of Technology - University: Nursing Care PlanSergiNo ratings yet
- NCP of PnuemoniaDocument13 pagesNCP of PnuemoniaFrando kenneth100% (1)
- NCP (Ineffective Airway)Document2 pagesNCP (Ineffective Airway)Angeline CasabuenaNo ratings yet
- Nursing Care Plan: Cystic FibrosisDocument4 pagesNursing Care Plan: Cystic FibrosisYael EzraNo ratings yet
- PneumothoraxDocument33 pagesPneumothoraxjamil aldasriNo ratings yet
- Nursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaDocument5 pagesNursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaSofiaLopezNo ratings yet
- Er NCP AddahDocument2 pagesEr NCP AddahAddah, Dhenaraiza H.No ratings yet
- Assessment Planning Intervention Rationale Evaluation: Nursing DiagnosisDocument2 pagesAssessment Planning Intervention Rationale Evaluation: Nursing DiagnosisLovely CacapitNo ratings yet
- NCP SciDocument3 pagesNCP SciJaylord VerazonNo ratings yet
- NCP - CapDocument2 pagesNCP - CapbercoaprilgraceNo ratings yet
- Actaul Drug StudyDocument2 pagesActaul Drug Studyjasper pachingelNo ratings yet
- Pneumonia Nursing Care PlanDocument3 pagesPneumonia Nursing Care PlanElle RosalesNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care Planalexander abasNo ratings yet
- NCP PesebreDocument2 pagesNCP PesebreFrancoise Nicolette PesebreNo ratings yet
- ACUTE RESPIRATORY DISTRESSDocument1 pageACUTE RESPIRATORY DISTRESSchristine louise bernardo100% (1)
- CopdDocument6 pagesCopdapi-3717941100% (2)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationYzel Vasquez AdavanNo ratings yet
- Vi. Nursing Care PlanDocument3 pagesVi. Nursing Care PlanJopaii TanakaNo ratings yet
- NURSING INTERVENTIONS FOR INEFFECTIVE BREATHING PATTERNDocument7 pagesNURSING INTERVENTIONS FOR INEFFECTIVE BREATHING PATTERNDanica Kate GalleonNo ratings yet
- Manila Doctors College: Pres. Diosdado Macapagal BLVD., Metropolitan Park, Pasay CityDocument3 pagesManila Doctors College: Pres. Diosdado Macapagal BLVD., Metropolitan Park, Pasay CityNichole CastleNo ratings yet
- NCP AsthmaDocument8 pagesNCP Asthmaqweyo yhuNo ratings yet
- FAELDONEA, PJ - Nursing Care PlanDocument6 pagesFAELDONEA, PJ - Nursing Care PlanPatricia Jean Faeldonea100% (1)
- Case Pres Ncps FinalDocument13 pagesCase Pres Ncps FinalMariejoy YadaoNo ratings yet
- Promoting Effective Breathing and Airway ClearanceDocument7 pagesPromoting Effective Breathing and Airway ClearanceJinaan MahmudNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- NCP For Scenario BreathingDocument4 pagesNCP For Scenario Breathingmy moznNo ratings yet
- Careplan 1Document11 pagesCareplan 1ligaba1559No ratings yet
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternReichelle Perlas62% (13)
- Nursi NG Care Plan: Cues Nursing Diagnosis Planning Nursing Intervention Rationale Expected OutcomeDocument2 pagesNursi NG Care Plan: Cues Nursing Diagnosis Planning Nursing Intervention Rationale Expected OutcomeErika Mae MananganNo ratings yet
- Assessing and Managing Respiratory DistressDocument3 pagesAssessing and Managing Respiratory DistressGen RodriguezNo ratings yet
- Pneumonia: (Related To Copious Tracheobronchial Secretions.)Document1 pagePneumonia: (Related To Copious Tracheobronchial Secretions.)Alyssa Mae DumularNo ratings yet
- NCP For CAP TB.Document5 pagesNCP For CAP TB.Cherry Ann BalagotNo ratings yet
- Improving Airway ClearanceDocument8 pagesImproving Airway ClearanceNikael Patun-ogNo ratings yet
- NCP NRMFDocument2 pagesNCP NRMFJai CortezNo ratings yet
- Managing COPD ExacerbationDocument17 pagesManaging COPD ExacerbationSean Menard Flores100% (1)
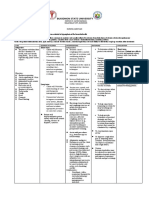
- Bukidnon State University: Subjective: Short Term: Short TermDocument1 pageBukidnon State University: Subjective: Short Term: Short TermSimbo Ralph JulesNo ratings yet
- Nursing Care Plan for DyspneaDocument2 pagesNursing Care Plan for DyspneaBianca Mikaela DosdosNo ratings yet
- Nursing Diagnosis Nursing Intervention Rationale Breathing PatternDocument8 pagesNursing Diagnosis Nursing Intervention Rationale Breathing PatternJinaan MahmudNo ratings yet
- NCP Priority1Document13 pagesNCP Priority1Jezebhel ArestaNo ratings yet
- Valeriano, NCPDocument4 pagesValeriano, NCPVALERIANO TRISHANo ratings yet
- AssessmentDocument7 pagesAssessmentSheryhan Tahir BayleNo ratings yet
- NCP.2F 2B 1Document5 pagesNCP.2F 2B 1JustineNo ratings yet
- 1 Impaired Gas ExchangeDocument11 pages1 Impaired Gas ExchangeKristian Dave DivaNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- NCP 1 AND SOAPIE 1) Ineffective Breathing PatternDocument5 pagesNCP 1 AND SOAPIE 1) Ineffective Breathing PatternMicaela CrisostomoNo ratings yet
- Panasonic Conduit CatalogDocument8 pagesPanasonic Conduit CatalogAhmed Said100% (2)
- Stress 1Document28 pagesStress 1DrAma StabLeNo ratings yet
- Ece-Research Work 1Document10 pagesEce-Research Work 1Peale ObiedoNo ratings yet
- DR 38312-011Document33 pagesDR 38312-011Julio Csar da SilvaNo ratings yet
- Ball Pen Canvas Painting Exhibition MumbaiDocument19 pagesBall Pen Canvas Painting Exhibition Mumbaiapi-25885725No ratings yet
- Sample Weekly Home Learning PlansDocument2 pagesSample Weekly Home Learning PlansJINGKY HUMAMOYNo ratings yet
- Model Business Plan Mango Pineapple Banana 1 1 1Document86 pagesModel Business Plan Mango Pineapple Banana 1 1 1ebubec92% (13)
- CV Electrical Engineer 2.7 Yrs ExpDocument4 pagesCV Electrical Engineer 2.7 Yrs ExpShams Tabrez0% (1)
- ACS Appl. Energy Mater. 5 (2022) 367-379 PDFDocument13 pagesACS Appl. Energy Mater. 5 (2022) 367-379 PDFEdgar QuintanillaNo ratings yet
- Atlas of Alteration MineralsDocument7 pagesAtlas of Alteration MineralsErick Leiva PadillaNo ratings yet
- 00 - Orientation LessonDocument32 pages00 - Orientation LessonRekha ShahNo ratings yet
- Curriculum MapDocument3 pagesCurriculum MapSem PerezNo ratings yet
- Public List Programs by Specialty 460Document9 pagesPublic List Programs by Specialty 460Enta SyngNo ratings yet
- Toyota Vehicle Glossary TermsDocument31 pagesToyota Vehicle Glossary TermsEdward Ugochukwu AdighibeNo ratings yet
- Conceptual SLDDocument1 pageConceptual SLDakhilNo ratings yet
- Present Perfect and Simple Past Tenses in ESL Grammar ExercisesDocument36 pagesPresent Perfect and Simple Past Tenses in ESL Grammar ExercisesNguyen Quoc AnhNo ratings yet
- Fmea PC ProcessDocument2 pagesFmea PC Processsudeep_singh1No ratings yet
- F 25 Sensor Family Miniature Sensors for Precision DetectionDocument34 pagesF 25 Sensor Family Miniature Sensors for Precision DetectionAlex GarduñoNo ratings yet
- Pump CommissioningDocument1 pagePump CommissioningMD SAMANNo ratings yet
- Amulets Talismans and CharmsDocument3 pagesAmulets Talismans and CharmsreikiladyNo ratings yet
- Official All Things Turmeric PPT GuidebookDocument14 pagesOfficial All Things Turmeric PPT Guidebookapi-507527047No ratings yet
- Manual Carpa Instant TentDocument2 pagesManual Carpa Instant TentBermans Olivares LayNo ratings yet
- Measuring: TranslateDocument5 pagesMeasuring: Translatechelsea romaidaNo ratings yet
- Guidelines in The Evaluation of Comprehensive Land Use PlanDocument8 pagesGuidelines in The Evaluation of Comprehensive Land Use PlanPa Rian Rho DoraNo ratings yet
- Chiller Maintenance Service 2015Document29 pagesChiller Maintenance Service 2015Huong Ban MaiNo ratings yet
- Development of Female Genital Tract and Its AnomaliesDocument44 pagesDevelopment of Female Genital Tract and Its AnomaliesSuresh KatakamNo ratings yet
- Irrigation Project ManualDocument66 pagesIrrigation Project ManualHorace Prophetic DavisNo ratings yet
- Industrial Attachment at Meghna Knit Composite Ltd.Document137 pagesIndustrial Attachment at Meghna Knit Composite Ltd.Riasat Alam50% (2)
- Definitions for Agricultural FinancingDocument15 pagesDefinitions for Agricultural FinancingShahid MehmoodNo ratings yet
- Evaluation of Plant Extracts Against Two Spotted Spider MiteDocument7 pagesEvaluation of Plant Extracts Against Two Spotted Spider MiteAnkaranaRenvaNo ratings yet