You might also like
- Sensorineural Hearing LossDocument19 pagesSensorineural Hearing LossBenitaNo ratings yet
- Mèniére's Disease DiplomaDocument47 pagesMèniére's Disease Diplomaadel madanyNo ratings yet
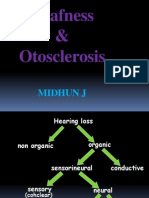
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- Hearing Loss: Mubarak MD Dhawal Mbbs (Iua), Morl (Mak) ENT Lecturer April 2019Document46 pagesHearing Loss: Mubarak MD Dhawal Mbbs (Iua), Morl (Mak) ENT Lecturer April 2019gibreilNo ratings yet
- ENT - UnitDocument63 pagesENT - Unitsuganthi rajesh kannaNo ratings yet
- Hearing LossDocument25 pagesHearing LossJumanne JayNo ratings yet
- Made By: DR Aditya RanjanDocument32 pagesMade By: DR Aditya RanjanArjun SainiNo ratings yet
- SSNHL SlidesDocument64 pagesSSNHL SlidesRAHMANo ratings yet
- Tuli Mendadak (Sudden Deafness)Document26 pagesTuli Mendadak (Sudden Deafness)Marisa FatkiyaNo ratings yet
- A. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthDocument6 pagesA. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthRubi MeeajanNo ratings yet
- Management of Adult Sensorineural Hearing Loss: EtiologiesDocument10 pagesManagement of Adult Sensorineural Hearing Loss: EtiologiesaldimugniNo ratings yet
- Ear ChronicDocument44 pagesEar ChronicȜLaa AsHrafNo ratings yet
- LabyrinthitisDocument7 pagesLabyrinthitisChristie ZamoraNo ratings yet
- Hearing Loss AssessmentDocument31 pagesHearing Loss AssessmentKIBET ERNEST MUTAINo ratings yet
- Hearing ImpairmentDocument7 pagesHearing ImpairmentIrene MendozaNo ratings yet
- Tinnitus 2Document35 pagesTinnitus 2Wael ShamyNo ratings yet
- Pathology: Efective Bsorption by Ndolymphatic AcDocument9 pagesPathology: Efective Bsorption by Ndolymphatic Acreza ahda kadirNo ratings yet
- Otitis MediaDocument98 pagesOtitis MediaLody Lean CruzNo ratings yet
- Labyrinth It Is Slides 040225Document38 pagesLabyrinth It Is Slides 040225Nadia YahayaNo ratings yet
- ICM 2 Cranial Nerve 7Document9 pagesICM 2 Cranial Nerve 7The Real UploaderNo ratings yet
- Mineire'sDocument16 pagesMineire'sShaykh Evangelista BacualNo ratings yet
- Meniere's DiseaseDocument50 pagesMeniere's DiseaseRaisa CleizeraNo ratings yet
- Seminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M LuxonDocument9 pagesSeminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M Luxonmaria_garaveNo ratings yet
- Unas Maret 101-130Document61 pagesUnas Maret 101-130Aji KusumaNo ratings yet
- Hearing Loss SMT IV44Document94 pagesHearing Loss SMT IV44abdul fattah mufidNo ratings yet
- Hearing Loss in Children - Etiology - UpToDateDocument39 pagesHearing Loss in Children - Etiology - UpToDateAlexander AdrielNo ratings yet
- AMBOSS Ear QuestionsDocument10 pagesAMBOSS Ear QuestionsSahil DnkNo ratings yet
- Genetics Evaluation of Persons/families With Hearing Loss, Genetic Screening Genetics of Hearing Impairment Gene Database For Hearing LossDocument12 pagesGenetics Evaluation of Persons/families With Hearing Loss, Genetic Screening Genetics of Hearing Impairment Gene Database For Hearing LosssherinNo ratings yet
- Meniere - Vestibular Disorders AssociationDocument11 pagesMeniere - Vestibular Disorders AssociationjdmjdmNo ratings yet
- Ear Notes - ExtractDocument50 pagesEar Notes - Extractadham bani younesNo ratings yet
- Sudden Sensorineural Hearing Loss by DrtbaluDocument3 pagesSudden Sensorineural Hearing Loss by DrtbaluAnish RajNo ratings yet
- A Rare Cause of Hearing Loss: Susac SyndromeDocument3 pagesA Rare Cause of Hearing Loss: Susac SyndromeBeny Pratama SidabutarNo ratings yet
- Background: Viral LabyrinthitisDocument6 pagesBackground: Viral LabyrinthitisranmiNo ratings yet
- Presbycusis: Dr. George Backleh Dept. of Otolaryngology/ Head and Neck Surgery Hadassah University Hospital JerusalemDocument16 pagesPresbycusis: Dr. George Backleh Dept. of Otolaryngology/ Head and Neck Surgery Hadassah University Hospital Jerusalemrezky_oktarianti_syahputriNo ratings yet
- Pemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanDocument71 pagesPemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanRilianda SimbolonNo ratings yet
- Meniere's Disease & OtosclerosisDocument44 pagesMeniere's Disease & OtosclerosisNadzirah Ahmad JailaniNo ratings yet
- Vestibular Neuritis and LabyrinthitisDocument18 pagesVestibular Neuritis and LabyrinthitischiquitaputriNo ratings yet
- Sordera SindromicaDocument8 pagesSordera SindromicaFabian Camelo OtorrinoNo ratings yet
- Disorders of Inner EarDocument82 pagesDisorders of Inner Earjhanavi rajeshNo ratings yet
- Drtbalu'S Otolaryngology Online: PresbyacusisDocument3 pagesDrtbalu'S Otolaryngology Online: PresbyacusisAnish RajNo ratings yet
- Meniere DiseaseDocument36 pagesMeniere DiseaseThamizharasan SivamaniNo ratings yet
- Uworld ENT NotesDocument4 pagesUworld ENT Notes808kailuaNo ratings yet
- Jurnal-NCBI-Paralisis Korda VokalisDocument20 pagesJurnal-NCBI-Paralisis Korda VokalisAchmad Hafidz BaraqbahNo ratings yet
- Keywords: Hearing Loss, Sudden Sensorineural Hearing Loss, Idiopathic Sudden SensorineuralDocument28 pagesKeywords: Hearing Loss, Sudden Sensorineural Hearing Loss, Idiopathic Sudden SensorineuralAnonymous TKpf3MFf15No ratings yet
- Hertzano 2020Document12 pagesHertzano 2020Moisés AarónNo ratings yet
- 중이염 Otitis MediaDocument213 pages중이염 Otitis MediaChangho LeeNo ratings yet
- Meniers DsDocument59 pagesMeniers DsAnurag SrivastavaNo ratings yet
- Lecture 2 Ent.Document70 pagesLecture 2 Ent.kiprotich weldonNo ratings yet
- What Is Presbycusis?: OtosclerosisDocument8 pagesWhat Is Presbycusis?: OtosclerosisIndraRukmanaHamimPartIINo ratings yet
- Approach To Hearing LossDocument7 pagesApproach To Hearing LossAlexandros GidarakosNo ratings yet
- Etiology and Diagnosis of Tinnitus - UpToDateDocument18 pagesEtiology and Diagnosis of Tinnitus - UpToDateAdri NolascoNo ratings yet
- Brain Abscess and SepsisDocument32 pagesBrain Abscess and SepsisSanjeet SahNo ratings yet
- Catetan BergunaDocument22 pagesCatetan BergunamellvinNo ratings yet
- Facial Nerve PalsyDocument3 pagesFacial Nerve PalsyGayle VillarizaNo ratings yet
- ENT 2marksDocument10 pagesENT 2marksSaileekitha AjamoniNo ratings yet
- Voice DisordersDocument6 pagesVoice DisorderssulnaikNo ratings yet
- Clinical Examination Techniques in Otology Edition IIDocument43 pagesClinical Examination Techniques in Otology Edition IIDr. T. Balasubramanian100% (2)
- 114 Barera CsDocument15 pages114 Barera Cskaloydiaz09No ratings yet
- Ear Disorders Hearing LossDocument21 pagesEar Disorders Hearing LossRatna PuspitasariNo ratings yet
- ANNEX I ASEAN GP For The Negative List Ver 3.0 (14nov14)Document27 pagesANNEX I ASEAN GP For The Negative List Ver 3.0 (14nov14)blackcholoNo ratings yet
- Adrenal FatigueDocument40 pagesAdrenal FatigueNimmi Nims67% (3)
- Morena E. Dail, RMT, MT (Amt), Mls (Ascpi) : Mors CodeDocument53 pagesMorena E. Dail, RMT, MT (Amt), Mls (Ascpi) : Mors CodemeriiNo ratings yet
- Effect of Nasapana in The Management of Avabahuka A Case StudyDocument5 pagesEffect of Nasapana in The Management of Avabahuka A Case StudyEditor IJTSRDNo ratings yet
- Excretion and Homeostasis.Document70 pagesExcretion and Homeostasis.philomenanjuguna72No ratings yet
- 24 VASQ Method VitA Intake 2006Document60 pages24 VASQ Method VitA Intake 2006aruniakpNo ratings yet
- Brief Notes Parish of St. RafaelDocument3 pagesBrief Notes Parish of St. RafaelAl F. Dela CruzNo ratings yet
- A Disease Prediction by Machine Learning Over Bigdata From Healthcare CommunitiesDocument3 pagesA Disease Prediction by Machine Learning Over Bigdata From Healthcare CommunitiesHarikrishnan ShunmugamNo ratings yet
- HPP Neuro Paper GraserDocument12 pagesHPP Neuro Paper GraserCaro ErazoNo ratings yet
- Presentation List Language Disorders in ChildrenDocument3 pagesPresentation List Language Disorders in Childrenramandeep kaurNo ratings yet
- Armohib 28 MSDSDocument8 pagesArmohib 28 MSDSdalton2004No ratings yet
- Chest X-Ray: Preparation Items Are Removed Appropriate Clothing Is Given ProcedureDocument5 pagesChest X-Ray: Preparation Items Are Removed Appropriate Clothing Is Given ProcedureRoshelMaeReasolBagotsayNo ratings yet
- PANCE Prep Pearls Cardio Questions PDFDocument9 pagesPANCE Prep Pearls Cardio Questions PDFkat100% (3)
- Neem LeavesDocument3 pagesNeem LeavesabdullahNo ratings yet
- Lecture 3 Innate ImmunityDocument26 pagesLecture 3 Innate ImmunitytimcarasNo ratings yet
- Apollo Excellence Report 2019 e VersionDocument289 pagesApollo Excellence Report 2019 e VersionrajNo ratings yet
- Rickey Dixon Letter To The Court On NFL Concussion Settlement FeesDocument9 pagesRickey Dixon Letter To The Court On NFL Concussion Settlement FeesRobert Lee100% (1)
- GIT Fluid BalanceDocument33 pagesGIT Fluid BalanceMaryNo ratings yet
- Zat Aktif & PBFDocument153 pagesZat Aktif & PBFnabilaNo ratings yet
- 681 FullDocument6 pages681 FullKurnia AnharNo ratings yet
- Full Download Test Bank For Ebersole and Hess Gerontological Nursing and Healthy Aging 2nd Canadian Edition by Touhy PDF Full ChapterDocument36 pagesFull Download Test Bank For Ebersole and Hess Gerontological Nursing and Healthy Aging 2nd Canadian Edition by Touhy PDF Full Chapteradrianblackiadxetkrqm100% (15)
- 4UFZ75PF0FYRH8 4UFZ75PF0FYRH8 : Division of Forensic SciencesDocument7 pages4UFZ75PF0FYRH8 4UFZ75PF0FYRH8 : Division of Forensic SciencesAttila KissNo ratings yet
- Myths PDFDocument8 pagesMyths PDFLuisa Elena HernandezNo ratings yet
- Xiong Et AlDocument21 pagesXiong Et AlVanessa AndradeNo ratings yet
- Respiratory PhysiologyDocument16 pagesRespiratory PhysiologyYsabel Salvador DychincoNo ratings yet
- Quality Assurance LaboratoryDocument118 pagesQuality Assurance LaboratoryMahesh KumarNo ratings yet
- Causative Agent: Mycobacterium TuberculosisDocument20 pagesCausative Agent: Mycobacterium TuberculosisDivya TiwariNo ratings yet
- Low Platelet CountDocument9 pagesLow Platelet Countfatimah_zkhanNo ratings yet
- Cataract Consent FormDocument4 pagesCataract Consent FormHitesh Sharma100% (1)
- 2017 - Pardede - Penerapan Terapi Suportif Dengan Teknik Bimbingan Untuk Mengurangi Dorongan Bunuh Diri Pada Pasien Skizofrenia PDFDocument8 pages2017 - Pardede - Penerapan Terapi Suportif Dengan Teknik Bimbingan Untuk Mengurangi Dorongan Bunuh Diri Pada Pasien Skizofrenia PDFIra Mayang SNo ratings yet