You might also like
- Nguyen 2013Document5 pagesNguyen 2013Biologija BiologyNo ratings yet
- Morphological Analyses and A Novel de Novo DLX3 Mutation Associated With Tricho - Dento-Osseous Syndrome in A Chinese FamilyDocument8 pagesMorphological Analyses and A Novel de Novo DLX3 Mutation Associated With Tricho - Dento-Osseous Syndrome in A Chinese FamilyMia De DiosNo ratings yet
- Dicostanzo 2011Document9 pagesDicostanzo 2011Biologija BiologyNo ratings yet
- Genetic Mapping of Autosomal Recessive Hypotrichosis Locus (LAH3), To Chromosome 13q14.11-q21.32, in A Family From BalochistanDocument8 pagesGenetic Mapping of Autosomal Recessive Hypotrichosis Locus (LAH3), To Chromosome 13q14.11-q21.32, in A Family From BalochistansternNo ratings yet
- Vascular Abnormalities of The Distal Deep Digital Flexor Tendon in 8 DraughtDocument4 pagesVascular Abnormalities of The Distal Deep Digital Flexor Tendon in 8 DraughtJulieta DiyorioNo ratings yet
- Alvim Pereira2008Document10 pagesAlvim Pereira2008Alejandro RuizNo ratings yet
- TaurodontismDocument15 pagesTaurodontismSiti Zahra MaharaniNo ratings yet
- Telomeres in Aging and Disease: Lessons From ZebrafishDocument12 pagesTelomeres in Aging and Disease: Lessons From Zebrafishsanwal hameedNo ratings yet
- 10 1002@sici1096-9896200003190@4516@@aid-Path5143 0 Co2-J PDFDocument2 pages10 1002@sici1096-9896200003190@4516@@aid-Path5143 0 Co2-J PDFjahdsdjad asffdhsajhajdkNo ratings yet
- Morphology of Cranial Sutures and RadiologicDocument6 pagesMorphology of Cranial Sutures and RadiologicEvans RodrigezNo ratings yet
- Reference and Techniques Used in Alveolar Bone ClassificationDocument5 pagesReference and Techniques Used in Alveolar Bone ClassificationAna Carolina LoyolaNo ratings yet
- Genetic Linkage of Hereditary Gingival Fibromatosis To Chromosome 2p21Document8 pagesGenetic Linkage of Hereditary Gingival Fibromatosis To Chromosome 2p21akasia.prillNo ratings yet
- Dento-Craniofacial Phenotypes and Underlying Molecular Mechanisms in Hypohidrotic Ectodermal Dysplasia (Hed) : A ReviewDocument11 pagesDento-Craniofacial Phenotypes and Underlying Molecular Mechanisms in Hypohidrotic Ectodermal Dysplasia (Hed) : A ReviewYusuf DiansyahNo ratings yet
- Library Dissertation On Stem Cells in DentistryDocument11 pagesLibrary Dissertation On Stem Cells in DentistryCustomPaperServicesCanada100% (1)
- Blazeketal2011 Disruption of Bone Development and Homeostasis byDocument16 pagesBlazeketal2011 Disruption of Bone Development and Homeostasis byLuis MiguelNo ratings yet
- Analysis of The Genetic Association Between Face Breadth and Maxillary Arch Width Using SMXA Recombinant Inbred Mouse StrainsDocument6 pagesAnalysis of The Genetic Association Between Face Breadth and Maxillary Arch Width Using SMXA Recombinant Inbred Mouse StrainsAhmad Ulil AlbabNo ratings yet
- Almstrup 2010Document8 pagesAlmstrup 2010Jair BrachoNo ratings yet
- Genetic Variation in Radiation-Induced Expression PhenotypesDocument6 pagesGenetic Variation in Radiation-Induced Expression PhenotypesAhmad ShamyNo ratings yet
- A Clinicoradiographic and Pathological Study of Pericoronal Follicles Associated To Mandibular Third MolarsDocument5 pagesA Clinicoradiographic and Pathological Study of Pericoronal Follicles Associated To Mandibular Third MolarsJean Carlos Barbosa FerreiraNo ratings yet
- Taurodontism in Dental Genetics: BdjopenDocument6 pagesTaurodontism in Dental Genetics: BdjopenFEBBY SITTINo ratings yet
- Butlers Field Theory PDFDocument7 pagesButlers Field Theory PDFsuchitra100% (1)
- Pubmed Article of Crotalus HorridusDocument3 pagesPubmed Article of Crotalus HorridusPraveen ManoharNo ratings yet
- Butler's Field TheoryDocument5 pagesButler's Field Theorypveginadu100% (1)
- Articulometodos 1Document19 pagesArticulometodos 1Sadness NeededNo ratings yet
- Tooth Agenesis Related GLI2 and GLI3 Genes May Contribute To CraniofacialDocument7 pagesTooth Agenesis Related GLI2 and GLI3 Genes May Contribute To Craniofacialhector rinconNo ratings yet
- The Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsDocument13 pagesThe Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsJevon JavierNo ratings yet
- 3 WiseDocument10 pages3 WiseAnonymous 64x5K7Di9rNo ratings yet
- Assessment of Complementary White Matter Microstructural CH - 2023 - Magnetic ReDocument10 pagesAssessment of Complementary White Matter Microstructural CH - 2023 - Magnetic ReKhushNo ratings yet
- Reprint of Prevalence and Characteristics of RootDocument11 pagesReprint of Prevalence and Characteristics of RootMarielEsmeraldaNo ratings yet
- Current Status of Sexing Mammalian Spermatozoa PDFDocument11 pagesCurrent Status of Sexing Mammalian Spermatozoa PDFMusunuri Ratna TejaNo ratings yet
- Comparative Corneal Topography and Refractive Variables in Monozygotic and Dizygotic TwinsDocument6 pagesComparative Corneal Topography and Refractive Variables in Monozygotic and Dizygotic TwinsPotencia SalasNo ratings yet
- Identification and Characterization of Essential Genes in The Human GenomeDocument7 pagesIdentification and Characterization of Essential Genes in The Human Genome戴义宾No ratings yet
- Duchenne Muscular Dystrophy Case Report and ReviewDocument3 pagesDuchenne Muscular Dystrophy Case Report and Reviewanita anjaniNo ratings yet
- Dis. Model. Mech. 2010 Hortopan 144 8Document5 pagesDis. Model. Mech. 2010 Hortopan 144 8Awanish MishraNo ratings yet
- Crime Investigation Through DNA Methylation AnalysisDocument17 pagesCrime Investigation Through DNA Methylation AnalysisAjay RanaNo ratings yet
- 2018 Article 92 PDFDocument16 pages2018 Article 92 PDFichaNo ratings yet
- HGPSDocument7 pagesHGPSIoana PaulaNo ratings yet
- Novel Mutations HMDocument9 pagesNovel Mutations HMSitipradyta KasimNo ratings yet
- Human Embryonic Stem Cells and Developing Human Fetal Liver Distinct DNA Methylation Patterns Characterize DifferentiatedDocument15 pagesHuman Embryonic Stem Cells and Developing Human Fetal Liver Distinct DNA Methylation Patterns Characterize DifferentiatedRoberto Bascuñan Dela FuenteNo ratings yet
- A Practical Approach To Interpretation of Dual-Energy X-Ray Absorptiometry (DXA) For Assessment of Bone DensityDocument12 pagesA Practical Approach To Interpretation of Dual-Energy X-Ray Absorptiometry (DXA) For Assessment of Bone DensityMuliaNo ratings yet
- Genetics in OrthodonticsDocument56 pagesGenetics in OrthodonticsSadhu AbhijeetNo ratings yet
- X-Linked Dominant Chondrodysplasia PunctataDocument5 pagesX-Linked Dominant Chondrodysplasia Punctatalocos3dNo ratings yet
- This Content Downloaded From 39.41.147.101 On Thu, 27 May 2021 00:05:54 UTCDocument4 pagesThis Content Downloaded From 39.41.147.101 On Thu, 27 May 2021 00:05:54 UTCIrfan Ullah 116-FBAS/MSCHM/F20No ratings yet
- Heat-Killed IStaphylococcusDocument14 pagesHeat-Killed IStaphylococcusSilmy IndariNo ratings yet
- Quantitative Heterodonty in Crocodylia ADocument37 pagesQuantitative Heterodonty in Crocodylia ACrocodilo VasconcelosNo ratings yet
- Ni Hms 38034Document9 pagesNi Hms 38034John ChambiNo ratings yet
- Karla P. García Pelagio 2011 - Biomechanics of The Sarcolemma and Costameres in Single Skeletal Muscle Fibers From Normal and Dystrophin-Null MiceDocument14 pagesKarla P. García Pelagio 2011 - Biomechanics of The Sarcolemma and Costameres in Single Skeletal Muscle Fibers From Normal and Dystrophin-Null MiceManuel SHNo ratings yet
- Comparison of Four Species-Delimitation Methods Applied To A DNA Barcode Data Set of Insect Larvae For Use in Routine BioassessmentDocument11 pagesComparison of Four Species-Delimitation Methods Applied To A DNA Barcode Data Set of Insect Larvae For Use in Routine BioassessmentLu ChiberryNo ratings yet
- Molecular Ecology - 2012 - O Neill - Parallel Tagged Amplicon Sequencing Reveals Major Lineages and Phylogenetic StructureDocument19 pagesMolecular Ecology - 2012 - O Neill - Parallel Tagged Amplicon Sequencing Reveals Major Lineages and Phylogenetic Structuremendozar787No ratings yet
- Aging and Cortical Bone Density of Mandible WithDocument5 pagesAging and Cortical Bone Density of Mandible WithAsdal AttoNo ratings yet
- 385 FullDocument8 pages385 FullEduardo MendozaNo ratings yet
- Im 2006Document10 pagesIm 2006Anonymous HcvcLY0No ratings yet
- Int Endodontic J - 2022 - Alsamahi - Type 2 Diabetes and The Clinically Normal Pulp An in Vitro StudyDocument12 pagesInt Endodontic J - 2022 - Alsamahi - Type 2 Diabetes and The Clinically Normal Pulp An in Vitro StudyAKSNo ratings yet
- A New Mouse Model of EhlersDanlos Syndrome Generated Using CRISPRCas9mediated Genomic editingDMM Disease Models and MechanismsDocument12 pagesA New Mouse Model of EhlersDanlos Syndrome Generated Using CRISPRCas9mediated Genomic editingDMM Disease Models and MechanismsMyrza AkbariNo ratings yet
- Telomere Shortening To Save Energy Leads To Weakened Immune SystemDocument19 pagesTelomere Shortening To Save Energy Leads To Weakened Immune SystemDavid LaPointNo ratings yet
- Restorative DentistryDocument3 pagesRestorative DentistryNawaf RuwailiNo ratings yet
- 2017 OmrDocument4 pages2017 Omrcalmua1234No ratings yet
- Bone Mineral Status in Imigrant Indo-Asian WomenDocument6 pagesBone Mineral Status in Imigrant Indo-Asian WomenchachaNo ratings yet
- The Genome Loading Model For The Origin and MainteDocument13 pagesThe Genome Loading Model For The Origin and MainteShopnil SarkarNo ratings yet
- Ang Mat Teme Za Ustni Del 08Document25 pagesAng Mat Teme Za Ustni Del 08Biologija BiologyNo ratings yet
- Seasonal Flooding in The Okavango Delta, Botswana - Recent History and Future ProspectsDocument9 pagesSeasonal Flooding in The Okavango Delta, Botswana - Recent History and Future ProspectsBiologija BiologyNo ratings yet
- Chemistry With ADF: Journal of Computational Chemistry July 2001Document38 pagesChemistry With ADF: Journal of Computational Chemistry July 2001Biologija BiologyNo ratings yet
- The Contributions of Authors To Multiauthored Biomedical Research PapersDocument15 pagesThe Contributions of Authors To Multiauthored Biomedical Research PapersBiologija BiologyNo ratings yet
- OVA37066E: Product Data SheetDocument2 pagesOVA37066E: Product Data SheetFred BionNo ratings yet
- ASCE 7 ASD Basic Load CombosDocument1 pageASCE 7 ASD Basic Load CombosAamirShabbirNo ratings yet
- W.R. Klemm (Auth.) - Atoms of Mind - The - Ghost in The Machine - Materializes-Springer Netherlands (2011)Document371 pagesW.R. Klemm (Auth.) - Atoms of Mind - The - Ghost in The Machine - Materializes-Springer Netherlands (2011)El equipo de Genesis ProjectNo ratings yet
- Quantities Survey MethodsDocument73 pagesQuantities Survey MethodsparvezNo ratings yet
- All Graphs and Charts Available in Show MeDocument16 pagesAll Graphs and Charts Available in Show MeGANGA TAGRANo ratings yet
- Differential Pr. Gauges Bellow Type 1Document2 pagesDifferential Pr. Gauges Bellow Type 1Vara PrasadNo ratings yet
- Design of Helical Pier Foundations in Frozen GroundDocument6 pagesDesign of Helical Pier Foundations in Frozen GroundCortesar ManuNo ratings yet
- Design of Water Supply System-High Rise BLDGDocument108 pagesDesign of Water Supply System-High Rise BLDGcris bunagNo ratings yet
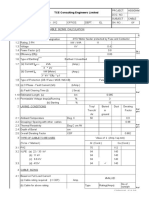
- Cable Sizing CalculationDocument72 pagesCable Sizing CalculationHARI my songs100% (1)
- The Power of Adventure in Your Hand: Product Catalog Volume 4 2019Document20 pagesThe Power of Adventure in Your Hand: Product Catalog Volume 4 2019Michael ShelbyNo ratings yet
- Elecon GearboxDocument19 pagesElecon GearboxShirley Farrace100% (3)
- OcrDocument16 pagesOcrBeena JaiswalNo ratings yet
- Improving of Transient Stability of Power Systems Using UPFCDocument6 pagesImproving of Transient Stability of Power Systems Using UPFCTana AzeezNo ratings yet
- Processing of Synthetic Aperture Radar Images - H. Maitre (Wiley, 2008) WWDocument411 pagesProcessing of Synthetic Aperture Radar Images - H. Maitre (Wiley, 2008) WWbehzad100% (4)
- PR100 BrochureDocument28 pagesPR100 Brochuregus289No ratings yet
- Mohamad Fakhari Mehrjardi - 1Document18 pagesMohamad Fakhari Mehrjardi - 1Hilmi SanusiNo ratings yet
- Numbers (0, 1, 2, 3,... ) Are Defined To Be Natural Numbers, Including Zero, That Does Not ContainDocument9 pagesNumbers (0, 1, 2, 3,... ) Are Defined To Be Natural Numbers, Including Zero, That Does Not ContainRomela EspedidoNo ratings yet
- Full U-Band Rectangular Waveguide-to-Microstrip Transition Using E-Plane ProbeDocument4 pagesFull U-Band Rectangular Waveguide-to-Microstrip Transition Using E-Plane ProbeSanjib MandalNo ratings yet
- en Product OverviewDocument81 pagesen Product OverviewShakeel AhmedNo ratings yet
- Clinical Study: The Effects of Uncomplicated Cataract Surgery On Retinal Layer ThicknessDocument7 pagesClinical Study: The Effects of Uncomplicated Cataract Surgery On Retinal Layer ThicknessJohn ElfranNo ratings yet
- 3AP1 DTC en - V9 - Epost PDFDocument8 pages3AP1 DTC en - V9 - Epost PDFjoan75No ratings yet
- Teaching and Learning Plan (TLP) : S. P. Mandali'S Prin L. N. Welingkar Institute of Management Development & ResearchDocument6 pagesTeaching and Learning Plan (TLP) : S. P. Mandali'S Prin L. N. Welingkar Institute of Management Development & ResearchBhagath VarenyaNo ratings yet
- Fundamentals of Physics Sixth Edition: Halliday Resnick WalkerDocument4 pagesFundamentals of Physics Sixth Edition: Halliday Resnick WalkerAhmar KhanNo ratings yet
- Organic Chemistry - Some Basic Principles and Techniques-1Document195 pagesOrganic Chemistry - Some Basic Principles and Techniques-1aditya kumar Agarwal100% (1)
- 100 TOP Real Time Objective C Multiple Choice Questions and Answers PDF DownloadDocument22 pages100 TOP Real Time Objective C Multiple Choice Questions and Answers PDF DownloadNayan BariNo ratings yet
- PLX7100A Digital Mobile C-Arm X-Ray Machine: 1. Technical SpecificationDocument3 pagesPLX7100A Digital Mobile C-Arm X-Ray Machine: 1. Technical SpecificationAbdalhakeem AlturkyNo ratings yet
- Semi Conductors: The Start of Information AgeDocument15 pagesSemi Conductors: The Start of Information AgeMarvin LabajoNo ratings yet
- WhiteLED1 8Document12 pagesWhiteLED1 8Smyle KatariaNo ratings yet
- Unit 6 - EarthingDocument26 pagesUnit 6 - Earthinggautam100% (1)
- Italy CasestudyDocument21 pagesItaly CasestudylozaNo ratings yet