You might also like
- Snippets in Surgery Vol 1: Illustrated Essentials of General SurgeryFrom EverandSnippets in Surgery Vol 1: Illustrated Essentials of General SurgeryRating: 5 out of 5 stars5/5 (1)
- Policy For Patients Requiring One To One ObservationDocument25 pagesPolicy For Patients Requiring One To One ObservationAshraf MullaNo ratings yet
- SOP-10-008 Suction July 20 2010 PDFDocument23 pagesSOP-10-008 Suction July 20 2010 PDFSalsabilla KimikoNo ratings yet
- Pi Is 0196064418301148Document5 pagesPi Is 0196064418301148Anonymous 0WHX7nNo ratings yet
- Patient Identification PolicyDocument20 pagesPatient Identification PolicyZahwa DhiyanaNo ratings yet
- WACHS Mental Health Seclusion Policy: 1. BackgroundDocument11 pagesWACHS Mental Health Seclusion Policy: 1. BackgroundFauziahNo ratings yet
- HSE Guidance Re CPR and DNAR Decision Making During The COVID 19 PandemicDocument15 pagesHSE Guidance Re CPR and DNAR Decision Making During The COVID 19 PandemicSANDHYANo ratings yet
- Restraint Policy 201107Document25 pagesRestraint Policy 201107nurhayatiNo ratings yet
- Clinical Handover UHL PolicyDocument13 pagesClinical Handover UHL PolicyOlaya ElgharinyNo ratings yet
- Covid 19 Guideline For Nutrition ManagementDocument17 pagesCovid 19 Guideline For Nutrition ManagementEdoardo Dalla NoraNo ratings yet
- CDC Guidance Correctional DetentionDocument26 pagesCDC Guidance Correctional DetentionEd PraetorianNo ratings yet
- Palliative Care Guidelines-20 November2013Document69 pagesPalliative Care Guidelines-20 November2013Olga ŢiuNo ratings yet
- PMM 58976644Document127 pagesPMM 58976644Neil OsborneNo ratings yet
- PD2014 025Document13 pagesPD2014 025brookie8868No ratings yet
- 1.1.1.4 Sedation PolicyDocument34 pages1.1.1.4 Sedation PolicyNguyen Duy ThanhNo ratings yet
- Mhareport1516 WebDocument68 pagesMhareport1516 WebRedNo ratings yet
- "DNR'' Do Not Resuscitate Status: Division: Department: SectionDocument8 pages"DNR'' Do Not Resuscitate Status: Division: Department: SectionKathleen Sharmaine S. CatubigNo ratings yet
- Infection Prevention and Control Guidance January 2021Document49 pagesInfection Prevention and Control Guidance January 2021saepulloh bin amingNo ratings yet
- SOP For Discharge Planning (Nursing)Document2 pagesSOP For Discharge Planning (Nursing)enumula kumar100% (1)
- C0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchDocument4 pagesC0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchKevo VillagranNo ratings yet
- N34 Roles of The RN by BRNDocument8 pagesN34 Roles of The RN by BRNhameunjungNo ratings yet
- UK - Rapid Guideline Critical Care in AdultsDocument13 pagesUK - Rapid Guideline Critical Care in AdultsAlexRázuriNo ratings yet
- COVID 19 Physicians GuideDocument4 pagesCOVID 19 Physicians GuidenilrmNo ratings yet
- OCA Circular No. 222-2023Document5 pagesOCA Circular No. 222-2023Branch 98 Regional Trial CourtNo ratings yet
- End of Life CareDocument34 pagesEnd of Life CareDhelche SarampangNo ratings yet
- 15 - DHA Telehealth Clinical Guidelines For Virtual Management of Acute Low Back PainDocument23 pages15 - DHA Telehealth Clinical Guidelines For Virtual Management of Acute Low Back PainMurilo GermanoNo ratings yet
- Standards of Good Practice For Spinal Interventional ProceduresDocument20 pagesStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaNo ratings yet
- ICU Criteria DuringDocument5 pagesICU Criteria DuringBaebee LouNo ratings yet
- Icu Survival Guide Sjuh 2nd EditionDocument27 pagesIcu Survival Guide Sjuh 2nd Edition吳任爵No ratings yet
- Use of Seclusion in DetentionDocument9 pagesUse of Seclusion in DetentionpaulfarrellNo ratings yet
- Safeguarding Alerts PolicyDocument16 pagesSafeguarding Alerts PolicyAgnieszka WaligóraNo ratings yet
- CCO GuidanceCOVIDmay152020Document9 pagesCCO GuidanceCOVIDmay152020jklNo ratings yet
- Administrative Policy & Procedure (App) Institutional Policy and Procedure (Ipp) Interdepartmental InternalDocument7 pagesAdministrative Policy & Procedure (App) Institutional Policy and Procedure (Ipp) Interdepartmental InternalKathleen Sharmaine S. CatubigNo ratings yet
- Refferal PolicyDocument19 pagesRefferal Policysabbo morsNo ratings yet
- Florida Task Force Report 9.1.20Document14 pagesFlorida Task Force Report 9.1.20ABC Action NewsNo ratings yet
- Telehealth Attending Provider Manual: University of Washington MedicineDocument36 pagesTelehealth Attending Provider Manual: University of Washington MedicinePsydocNo ratings yet
- Guide To Health PrivacyDocument65 pagesGuide To Health PrivacyRooney SamirNo ratings yet
- In-Service Education VirginiaDocument25 pagesIn-Service Education Virginiaapi-234162801No ratings yet
- PD2014 028Document30 pagesPD2014 028Inne Milagros FransienDimpudusNo ratings yet
- COVID19 IPCProtocolSurgicalProceduresAdultDocument16 pagesCOVID19 IPCProtocolSurgicalProceduresAdultwatimelawatiNo ratings yet
- Sop Number Title of SOP Author Consultation With StakeholdersDocument23 pagesSop Number Title of SOP Author Consultation With StakeholdersMr. BamsNo ratings yet
- Venepuncture Policy 3.0Document34 pagesVenepuncture Policy 3.0wenyNo ratings yet
- Adapting Community-Based Management of Acute Malnutrition in The Context of COVID-19Document19 pagesAdapting Community-Based Management of Acute Malnutrition in The Context of COVID-19Maharu MathewosNo ratings yet
- CFOP - Clinical Obeservations 8-1-11Document16 pagesCFOP - Clinical Obeservations 8-1-11sterlingcorryNo ratings yet
- New Eready - HmoaDocument13 pagesNew Eready - HmoaEngilbert MaqueraNo ratings yet
- COVID-19 Rapid Guideline: Managing Symptoms (Including at The End of Life) in The CommunityDocument19 pagesCOVID-19 Rapid Guideline: Managing Symptoms (Including at The End of Life) in The CommunityDoriNo ratings yet
- Lecture - TCC Operating ManualDocument15 pagesLecture - TCC Operating ManualMagr Esca100% (1)
- 433 Medical Aid and ResponseDocument6 pages433 Medical Aid and ResponseThe Columbus DispatchNo ratings yet
- NWLHT Incident Reporting Policy NewDocument64 pagesNWLHT Incident Reporting Policy Newmorrissey27No ratings yet
- NaharDocument42 pagesNahargrace0122rnNo ratings yet
- Outpatient Setting: Nurses PresentDocument2 pagesOutpatient Setting: Nurses PresentNatalie FanNo ratings yet
- Medical Board - Guidelines - Registered Health Practitioners and Students in Relation To Blood Borne VirusesDocument57 pagesMedical Board - Guidelines - Registered Health Practitioners and Students in Relation To Blood Borne Virusesddavies69No ratings yet
- Covid19 Rapid Guideline Pneumonia in Adults in The CommunityDocument15 pagesCovid19 Rapid Guideline Pneumonia in Adults in The CommunityDusan OrescaninNo ratings yet
- Home Health Care Medical Standards: An OverviewDocument108 pagesHome Health Care Medical Standards: An OverviewSouheil DamajNo ratings yet
- 2 Ethico-Legal Issues On IVTDocument81 pages2 Ethico-Legal Issues On IVT4LetterLie31No ratings yet
- NG163Document24 pagesNG163Tim BrownNo ratings yet
- COVID 19 Home Care GuidelinesDocument35 pagesCOVID 19 Home Care GuidelinesNeenNo ratings yet
- DNRDocument3 pagesDNRAak CeyeNo ratings yet
- Sri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034Document49 pagesSri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034dhir.ankur100% (1)
- Flowchart For Monitoring Rapid Response Team Performance - Healthcare Projects - Tao's TipsDocument7 pagesFlowchart For Monitoring Rapid Response Team Performance - Healthcare Projects - Tao's Tipshatem newishyNo ratings yet
- Protocol 014Document19 pagesProtocol 014hatem newishyNo ratings yet
- Absconding Policy and ProcedureDocument3 pagesAbsconding Policy and Procedurehatem newishyNo ratings yet
- 2775 BrowseDocument11 pages2775 Browsehatem newishyNo ratings yet
- Module 13b Absconding and Missing PatientsDocument32 pagesModule 13b Absconding and Missing Patientshatem newishyNo ratings yet
- PD2019 020Document11 pagesPD2019 020hatem newishyNo ratings yet
- Clinical Handover UHL PolicyDocument13 pagesClinical Handover UHL PolicyOlaya ElgharinyNo ratings yet
- Handover PolicyDocument19 pagesHandover Policyhatem newishyNo ratings yet
- VTE - Prophylaxis - PROTOCOL - V1.1 - With Forms - 07 - Dec - 2023Document20 pagesVTE - Prophylaxis - PROTOCOL - V1.1 - With Forms - 07 - Dec - 2023hatem newishyNo ratings yet
- VTE Prophylaxis PROTOCOL V1.2 Withforms 31 Dec 2023Document19 pagesVTE Prophylaxis PROTOCOL V1.2 Withforms 31 Dec 2023hatem newishyNo ratings yet
- Nice 2023Document3 pagesNice 2023hatem newishyNo ratings yet
- Skills in Clinical NursingDocument18 pagesSkills in Clinical Nursinghatem newishyNo ratings yet
- Pracactical Session of CVS ModuleDocument18 pagesPracactical Session of CVS Modulehatem newishyNo ratings yet
- MS& Poc Cbahi 3RD EditionDocument23 pagesMS& Poc Cbahi 3RD Editionhatem newishyNo ratings yet
- National TB ProgramDocument188 pagesNational TB Programhatem newishyNo ratings yet
- Right of DisabledDocument28 pagesRight of DisabledsarayooNo ratings yet
- Statutory Forms PDFDocument4 pagesStatutory Forms PDFWorkrelated UniworkNo ratings yet
- (1990) 2 A.C. 1 PDFDocument84 pages(1990) 2 A.C. 1 PDFBruce BeeNo ratings yet
- Case Scenario JasonDocument6 pagesCase Scenario JasonMaddy HuckelNo ratings yet
- Mental Health: LawDocument65 pagesMental Health: Lawopenid_mdOQtZ3zNo ratings yet
- Mental Health ActDocument43 pagesMental Health Actbaskirathi100% (1)
- Rules: The Ancient Order of Foresters Friendly Society LimitedDocument45 pagesRules: The Ancient Order of Foresters Friendly Society LimitedFuzzy_Wood_PersonNo ratings yet
- New South Wales V TalovicDocument40 pagesNew South Wales V TalovicbobNo ratings yet
- Admission and Discharge Procedure in Psy HospitalDocument37 pagesAdmission and Discharge Procedure in Psy HospitalChandrashekar GajulaNo ratings yet
- CR174Document57 pagesCR174vaidyamNo ratings yet
- Guidance Document On Individual Care PlanningDocument59 pagesGuidance Document On Individual Care Planningkoyote73No ratings yet
- Adult-Inpatient Eating Disorder GuidelinesDocument18 pagesAdult-Inpatient Eating Disorder GuidelinesJuanCarlos Yogi100% (1)
- Legal Issues in Mental Health NursingDocument61 pagesLegal Issues in Mental Health NursingS KANIMOZHINo ratings yet
- Voluntary AdmissionDocument1 pageVoluntary Admissionapi-414703292No ratings yet
- Policing Vancouver's Mentally IllDocument35 pagesPolicing Vancouver's Mentally IllVancouver 24 HoursNo ratings yet
- A Guide For Bachelor of Science (Nursing) Licensing ExaminationDocument185 pagesA Guide For Bachelor of Science (Nursing) Licensing ExaminationEVERYTHING TvNo ratings yet
- FARVACE Contracts Unsoundness of MindDocument14 pagesFARVACE Contracts Unsoundness of MindsandeepNo ratings yet
- Health and Privacy PDFDocument40 pagesHealth and Privacy PDFMonika NegiNo ratings yet
- The Mind Guide To Seeking Help For A Mental Health ProblemDocument32 pagesThe Mind Guide To Seeking Help For A Mental Health ProblemRobbieD455No ratings yet
- Refocusing The Care Programme ApproachDocument64 pagesRefocusing The Care Programme ApproachMHRED_UOLNo ratings yet
- Mental Health Act 2001 and Mental Health Regulation 2010Document22 pagesMental Health Act 2001 and Mental Health Regulation 2010Farahim DaudNo ratings yet
- Roles Functions Advice NoteDocument27 pagesRoles Functions Advice NoteCristina Lorena Grasu100% (1)
- London HD Contract of Employment-3Document8 pagesLondon HD Contract of Employment-3Ivana Perisic JanicicNo ratings yet
- Objectives. - The Objectives of This IRR Are, As Follows:: AddictionDocument1 pageObjectives. - The Objectives of This IRR Are, As Follows:: AddictionGreggy LawNo ratings yet
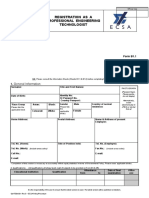
- Registration As A Professional Engineering Technologist: Effective Date: 1 April 2018 Rev No: 0Document41 pagesRegistration As A Professional Engineering Technologist: Effective Date: 1 April 2018 Rev No: 0bra9tee9tiniNo ratings yet
- Extended LeaveDocument1 pageExtended Leaveapi-414703292No ratings yet
- Mental Health Act 2001Document41 pagesMental Health Act 2001Da UsNo ratings yet
- A Comparison of Mental Health Legislation in FiveDocument10 pagesA Comparison of Mental Health Legislation in FivejeniadhyaruNo ratings yet
- 7Th Grade Persuasive Essay TopicsDocument8 pages7Th Grade Persuasive Essay TopicsapgsrfnbfNo ratings yet
- Mental Health and Addiction Recommendations and ResponseDocument9 pagesMental Health and Addiction Recommendations and ResponseStuff NewsroomNo ratings yet