You might also like
- Weisfeldt 2002Document4 pagesWeisfeldt 2002GRACE VICTORIA TINJACA CARDONANo ratings yet
- HHS Public Access: Cardiac Arrest: Resuscitation and ReperfusionDocument17 pagesHHS Public Access: Cardiac Arrest: Resuscitation and Reperfusionagus indrawanNo ratings yet
- A Case of Refractory Ventricular Fibrillation Successfully Treated With Low-Dose EsmololDocument5 pagesA Case of Refractory Ventricular Fibrillation Successfully Treated With Low-Dose EsmolollucaspfreitassNo ratings yet
- Three Phases ArrestDocument5 pagesThree Phases ArrestDaniel PradenasNo ratings yet
- 3 Fase Henti JantungDocument8 pages3 Fase Henti JantungtrimardiyanaisyanNo ratings yet
- The Physiology of Cardiopulmonary Resuscitation (CPR) - ECG & ECHODocument9 pagesThe Physiology of Cardiopulmonary Resuscitation (CPR) - ECG & ECHOUrgencias La RazaNo ratings yet
- Evolution of The Stone HeartDocument6 pagesEvolution of The Stone HeartHeitor PóvoasNo ratings yet
- CPR First? or Defibrillation First?: Re-AffirmedDocument4 pagesCPR First? or Defibrillation First?: Re-AffirmedangelNo ratings yet
- ACLS AlgorithmDocument12 pagesACLS AlgorithmwildionNo ratings yet
- Analysis and Results of Prolonged Resuscitation in Cardiac Arrest Patients Rescued by Extracorporeal Membrane OxygenationDocument7 pagesAnalysis and Results of Prolonged Resuscitation in Cardiac Arrest Patients Rescued by Extracorporeal Membrane OxygenationMuhammad RizqiNo ratings yet
- Cardiac ArrestDocument4 pagesCardiac Arrestapi-648401824No ratings yet
- Resuscitation After Cardiac Arrest A 3-Phase Time PDFDocument5 pagesResuscitation After Cardiac Arrest A 3-Phase Time PDFGabriela PachecoNo ratings yet
- Post Resuscitation CareDocument3 pagesPost Resuscitation CareprashsubbuNo ratings yet
- 1 s2.0 S0022522303007396 MainDocument9 pages1 s2.0 S0022522303007396 MainAna Maria Muñoz GonzalezNo ratings yet
- Acls Seminar MeDocument62 pagesAcls Seminar MeAbnet Wondimu100% (1)
- Cardioversion, and Pacing Part 5: Electrical Therapies: Automated External Defibrillators, DefibrillationDocument13 pagesCardioversion, and Pacing Part 5: Electrical Therapies: Automated External Defibrillators, DefibrillationAndy XiaoNo ratings yet
- Minimally Invasive Direct Cardiac MassagDocument13 pagesMinimally Invasive Direct Cardiac MassagTM AnNo ratings yet
- Cardiorespiratory ArrestDocument5 pagesCardiorespiratory Arrestore wa IzzampNo ratings yet
- Medip, IJAM-724 CDocument3 pagesMedip, IJAM-724 CKhalilSemlaliNo ratings yet
- Determinants of Delayed Preconditioning Against Myocardial PDFDocument19 pagesDeterminants of Delayed Preconditioning Against Myocardial PDFSol SolNo ratings yet
- Brain Death Provokes Acute Alteration in Myocardial Morphology Transplant Int 2011Document7 pagesBrain Death Provokes Acute Alteration in Myocardial Morphology Transplant Int 2011Marisol Gallego DuqueNo ratings yet
- Amniotic Fluid Embolism: Principles of Early Clinical ManagementDocument5 pagesAmniotic Fluid Embolism: Principles of Early Clinical Management16.11Hz MusicNo ratings yet
- CardioversiaDocument13 pagesCardioversiaMihai GRIGORENo ratings yet
- Wiga 2011Document9 pagesWiga 2011S4lNo ratings yet
- ECG Description:: Ventricular FibrillationDocument2 pagesECG Description:: Ventricular FibrillationpsyNo ratings yet
- Resuscitation Guide Lines 2005: Aries PerdanaDocument36 pagesResuscitation Guide Lines 2005: Aries PerdanaLa Ode RinaldiNo ratings yet
- Cardiopulmonary Resuscitation: Unusual Techniques For Unusual Situations ConclusionDocument8 pagesCardiopulmonary Resuscitation: Unusual Techniques For Unusual Situations ConclusionIlham AkbarNo ratings yet
- 10 FullDocument7 pages10 FullWinda Ayu SholikhahNo ratings yet
- Postoperative Atrial Fibrillation: The Role of The Inflammatory ResponseDocument9 pagesPostoperative Atrial Fibrillation: The Role of The Inflammatory ResponseHendrik AbrahamNo ratings yet
- Franzini 2016Document1 pageFranzini 2016RicardoNo ratings yet
- Percussion Pacing - An Almost Forgotten Procedure For Haemodynamically Unstable Bradycardias A Report of Three Case Studies and Review of The LiteratureDocument5 pagesPercussion Pacing - An Almost Forgotten Procedure For Haemodynamically Unstable Bradycardias A Report of Three Case Studies and Review of The LiteratureLilianneNo ratings yet
- Cardiac Arrest and CardiopulmonaryDocument14 pagesCardiac Arrest and CardiopulmonaryCarlos UrquijoNo ratings yet
- Advanced Life Support Algorithm: Learning OutcomesDocument12 pagesAdvanced Life Support Algorithm: Learning OutcomesAljeirou AlcachupasNo ratings yet
- Nejmcp 2023658Document9 pagesNejmcp 2023658bbraitsilvaNo ratings yet
- DEFIBrilatorDocument43 pagesDEFIBrilatoranon_632568468No ratings yet
- 1 s2.0 S0735109705028111 MainDocument7 pages1 s2.0 S0735109705028111 MainDista ArifanyNo ratings yet
- Management of Cardiac ArrestDocument10 pagesManagement of Cardiac ArrestAhmed VelićNo ratings yet
- Physiology of Closed Chest CompressionsDocument3 pagesPhysiology of Closed Chest CompressionsAriniDwiLestariNo ratings yet
- Ventricular Fibrillation and Defibrillation: ReviewDocument6 pagesVentricular Fibrillation and Defibrillation: ReviewIrfan AchmadNo ratings yet
- Cardiopulmonary Resuscitation (CPR) : Treatment & Medication MultimediaDocument2 pagesCardiopulmonary Resuscitation (CPR) : Treatment & Medication Multimediapreet kaurNo ratings yet
- Jam IsolaDocument11 pagesJam IsolaCAMOMILLE ROSE JAMISOLANo ratings yet
- 2019 Journal of Thoracic and Cardiovascular SurgeryDocument10 pages2019 Journal of Thoracic and Cardiovascular SurgeryFernando ZanoniNo ratings yet
- Referensi 7Document8 pagesReferensi 7Nophy NapitupuluNo ratings yet
- Advance Cardiac SuppDocument32 pagesAdvance Cardiac SuppVijith.V.kumarNo ratings yet
- CardiorespiratoryDocument10 pagesCardiorespiratoryEdi Saputra SNo ratings yet
- Airway Management in Cardiac ArrestDocument14 pagesAirway Management in Cardiac ArrestInternos UrgenciasNo ratings yet
- Changes in Myocardial Function and Perfusion After Acute Myocardial InfarctionDocument3 pagesChanges in Myocardial Function and Perfusion After Acute Myocardial InfarctionFederico OchoaNo ratings yet
- Gasping During Cardiac Arrest in Humans Is Frequent and Associated With Improved SurvivalDocument5 pagesGasping During Cardiac Arrest in Humans Is Frequent and Associated With Improved SurvivalCarla Eliberta ColodroNo ratings yet
- Pericardiocentesis in Cardiac Tamponade: A Case For "Less Is More"Document7 pagesPericardiocentesis in Cardiac Tamponade: A Case For "Less Is More"Natalindah Jokiem Woecandra T. D.No ratings yet
- Atrial Fibrillation: Clinical PracticeDocument9 pagesAtrial Fibrillation: Clinical PracticeenesNo ratings yet
- 1tDn nNUqdJMD2ylVCoKmvQ7GfkQ8iGdRDocument8 pages1tDn nNUqdJMD2ylVCoKmvQ7GfkQ8iGdRRossy Viviana Bernabé CastilloNo ratings yet
- J Vet Emergen Crit Care - 2012 - Rozanski - RECOVER Evidence and Knowledge Gap Analysis On Veterinary CPR Part 4 AdvancedDocument21 pagesJ Vet Emergen Crit Care - 2012 - Rozanski - RECOVER Evidence and Knowledge Gap Analysis On Veterinary CPR Part 4 Advancedsebastian Jimenez PNo ratings yet
- Fibrilacioni Atrial Trajtimi Dhe Diagnoza e TijDocument8 pagesFibrilacioni Atrial Trajtimi Dhe Diagnoza e TijMarsiano QendroNo ratings yet
- Acute Medicine & SurgeryDocument5 pagesAcute Medicine & SurgeryImaniar VitasariNo ratings yet
- Reply To Letter Continuous Chest Compression ResuDocument2 pagesReply To Letter Continuous Chest Compression ResuJorge CamarilloNo ratings yet
- Application of Ultrasound in Pulseless Electrical Activity (PEA) Cardiac ArrestDocument3 pagesApplication of Ultrasound in Pulseless Electrical Activity (PEA) Cardiac ArrestKelvin AKNo ratings yet
- Percutaneous Cardiac Support During Myocardial Infarction Drastically Reduces Mortality: Perspectives From A Swine ModelDocument7 pagesPercutaneous Cardiac Support During Myocardial Infarction Drastically Reduces Mortality: Perspectives From A Swine ModelAdrian BratuNo ratings yet
- 6-CPR Techniques and DevicesDocument4 pages6-CPR Techniques and Devicesapi-3835927No ratings yet
- The Blalock and Taussig Shunt Revisited: Review ArticleDocument8 pagesThe Blalock and Taussig Shunt Revisited: Review ArticlearwitarahayuNo ratings yet
- Continuous Chest Compression Resuscitation in ArreDocument1 pageContinuous Chest Compression Resuscitation in ArreJorge CamarilloNo ratings yet
- Recibo Manual Proveedor BlsDocument1 pageRecibo Manual Proveedor BlsJorge CamarilloNo ratings yet
- Cardiac Output Measurement During Mechanical CPR IDocument1 pageCardiac Output Measurement During Mechanical CPR IJorge CamarilloNo ratings yet
- Certificate: Jorge GarciaDocument1 pageCertificate: Jorge GarciaJorge CamarilloNo ratings yet
- Bryan Williams Clin Med 2022 22:499-505: © Royal College of Physicians 2022. All Rights ReservedDocument1 pageBryan Williams Clin Med 2022 22:499-505: © Royal College of Physicians 2022. All Rights ReservedJorge CamarilloNo ratings yet
- Publicar Un Estado 2Document1 pagePublicar Un Estado 2Jorge CamarilloNo ratings yet
- Refinery Project ProposalDocument47 pagesRefinery Project ProposalAlhikmal MardiansahNo ratings yet
- MMC 1Document7 pagesMMC 1Jorge CamarilloNo ratings yet
- EpinefrinaDocument10 pagesEpinefrinaJorge CamarilloNo ratings yet
- Reply To Letter Continuous Chest Compression ResuDocument2 pagesReply To Letter Continuous Chest Compression ResuJorge CamarilloNo ratings yet
- Chapter 26 Management of Patients With Dysrhythmias and Conduction ProblemsDocument22 pagesChapter 26 Management of Patients With Dysrhythmias and Conduction ProblemsAbel C. Idusma Jr.No ratings yet
- Shanghai Score System For Diagnosis of Brugada Syndrome PDFDocument7 pagesShanghai Score System For Diagnosis of Brugada Syndrome PDFFendy WellenNo ratings yet
- Medical Electronics - SKP 116 135Document20 pagesMedical Electronics - SKP 116 135Mohammed Mian ANo ratings yet
- 2019 Catheter Ablation of VA PDFDocument153 pages2019 Catheter Ablation of VA PDFyusupNo ratings yet
- ECG Library PDFDocument98 pagesECG Library PDFJayden WaveNo ratings yet
- Analizador Desfibirlador Da 2006 Series User ManualDocument112 pagesAnalizador Desfibirlador Da 2006 Series User ManualquiqueNo ratings yet
- Diagnostic DefibrillationDocument1 pageDiagnostic DefibrillationRobNo ratings yet
- DefibrillatorDocument85 pagesDefibrillatorDhruv DesaiNo ratings yet
- Cardiac Dysrhythmias ExamDocument4 pagesCardiac Dysrhythmias Exambobtaguba100% (3)
- Spanish Medical GlossaryDocument129 pagesSpanish Medical GlossaryAlex ObandoNo ratings yet
- Why 360j Clinical OverviewDocument8 pagesWhy 360j Clinical OverviewPepperNo ratings yet
- CCPC15 Acute Cardiac Care Workbook PDFDocument42 pagesCCPC15 Acute Cardiac Care Workbook PDFMina Samir BesharaNo ratings yet
- STAR Arrhythmia Monitoring PDFDocument16 pagesSTAR Arrhythmia Monitoring PDFalghashm001No ratings yet
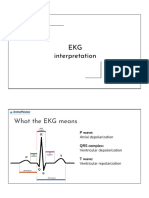
- Ekg InterpretationDocument26 pagesEkg Interpretationpaulzilicous.artNo ratings yet
- Defibrillator TesterDocument4 pagesDefibrillator Testerdenivaldo2009No ratings yet
- Holter Contec TLC9803 User Manual - EnglishDocument53 pagesHolter Contec TLC9803 User Manual - EnglishEdward MoralesNo ratings yet
- Perceived Competence in Cardiopulmonary Resuscitation, Knowledge and Skills, Amongst 50 Qualified NursesDocument6 pagesPerceived Competence in Cardiopulmonary Resuscitation, Knowledge and Skills, Amongst 50 Qualified NursesYannis ZoldenbergNo ratings yet
- Dilated Cardiomyopathy Notes AtfDocument15 pagesDilated Cardiomyopathy Notes AtfSingha ChangsiriwatanaNo ratings yet
- Atrial Fibrillation Slide PresentationDocument12 pagesAtrial Fibrillation Slide Presentationguglielmo2009No ratings yet
- Cardiac Arrhythmias Practice QuizDocument20 pagesCardiac Arrhythmias Practice Quizhahaha100% (1)
- NP3 4Document65 pagesNP3 4Edward Nicko Garcia100% (1)
- Design of An Open Source AED in The Framework of The UBORA ProjectDocument5 pagesDesign of An Open Source AED in The Framework of The UBORA ProjectAwadhNo ratings yet
- Ventricular and Atrial Fibrillation and FlutterDocument21 pagesVentricular and Atrial Fibrillation and Flutteryasir ishaqNo ratings yet
- Antiarrhythmic DrugsDocument42 pagesAntiarrhythmic DrugsRamadi PrameelaNo ratings yet
- Touchcardio HRC Abstracts 2022 Final 3Document149 pagesTouchcardio HRC Abstracts 2022 Final 3Cristina AdamNo ratings yet
- 1 s2.0 S0735109719384530 MainDocument11 pages1 s2.0 S0735109719384530 MainMartin Helguera PeredaNo ratings yet
- The Search For The Physical Cause of Jesus Christ's DeathDocument17 pagesThe Search For The Physical Cause of Jesus Christ's Deathgaborm_23No ratings yet
- Especificaciones TLC5007Document2 pagesEspecificaciones TLC5007rober nunNo ratings yet
- Elsiver NCLEX Critical CareDocument112 pagesElsiver NCLEX Critical CareHasan A AsFour100% (1)
- Rigel Uni Pulse Manual v1.3Document40 pagesRigel Uni Pulse Manual v1.3RandhiMahardhikaNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (26)