You might also like
- Mucusless-Diet Healing System - A Complete Course for Those Who Desire to Learn How to Control Their HealthFrom EverandMucusless-Diet Healing System - A Complete Course for Those Who Desire to Learn How to Control Their HealthNo ratings yet
- 5 2015 Farmako-ToxicologyDocument71 pages5 2015 Farmako-ToxicologyIkhzan PriolaksanaNo ratings yet
- Occupational Toxicology: Threshold Limit Values (TLVS) Environmental ToxicologyDocument7 pagesOccupational Toxicology: Threshold Limit Values (TLVS) Environmental ToxicologyJustin Victor AngNo ratings yet
- General ToxicologyDocument57 pagesGeneral ToxicologyOhoodNo ratings yet
- Endogenous Intoxication in SurgeryDocument5 pagesEndogenous Intoxication in SurgeryJonah Seeni100% (1)
- Lecture Pharma Part 1 - 2011-2012Document34 pagesLecture Pharma Part 1 - 2011-2012Harley Justiniani Dela CruzNo ratings yet
- Pharmacology ReviewDocument28 pagesPharmacology ReviewKathy Wollschleger100% (1)
- Principles of Pharmacology FFU-1Document168 pagesPrinciples of Pharmacology FFU-1anisa ahmedNo ratings yet
- F ToxicologyDocument17 pagesF Toxicologyempress venus bonillaNo ratings yet
- ToxicologyDocument3 pagesToxicologyDiah MarianoNo ratings yet
- Toxicology IntroductionDocument26 pagesToxicology IntroductionPlayersbattle Ground100% (1)
- TOXICOLOGY NotesDocument4 pagesTOXICOLOGY NotesAlexandra RullanNo ratings yet
- General Pharmacology 1Document24 pagesGeneral Pharmacology 1ismailaiaibrahimNo ratings yet
- #General Toxicology PDFDocument11 pages#General Toxicology PDFsarahabdullahNo ratings yet
- Chapter 34Document4 pagesChapter 34monster40lbsNo ratings yet
- ToxicologyDocument19 pagesToxicologyPEARL THERESE SUDARIONo ratings yet
- Acute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDDocument76 pagesAcute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDSamapriya Pasan Hewawasam100% (1)
- Principles of Toxicology: Medical PharmacologyDocument20 pagesPrinciples of Toxicology: Medical PharmacologyRani PuspitaNo ratings yet
- General ToxicologyDocument44 pagesGeneral ToxicologySachin SonawaneNo ratings yet
- General Considerations On Toxicology - To Send For 2021admDocument66 pagesGeneral Considerations On Toxicology - To Send For 2021admhadiyaNo ratings yet
- Copy ofDocument94 pagesCopy ofPreetibah PatelNo ratings yet
- Basic PharmacologyDocument5 pagesBasic PharmacologyAngela CancinoNo ratings yet
- Clinical Toxicology - Lecture 03Document17 pagesClinical Toxicology - Lecture 03Muhammad ZubairNo ratings yet
- Poison Intro GaseousDocument73 pagesPoison Intro GaseouspikachuNo ratings yet
- Pharmacologic PrinciplesDocument57 pagesPharmacologic PrinciplesYousef Jafar100% (1)
- Routes of Drug AdministrationDocument37 pagesRoutes of Drug AdministrationkeitoumaNo ratings yet
- Poisoning and ManagementDocument53 pagesPoisoning and ManagementYusuf Nawaz KhanNo ratings yet
- Pharma Module 1Document8 pagesPharma Module 1Neugene CuNo ratings yet
- Principles of Toxicology: The Study of PoisonsDocument23 pagesPrinciples of Toxicology: The Study of PoisonsnitishkjhaNo ratings yet
- Toxicology Practical 1Document3 pagesToxicology Practical 1Sharmila SeeralanNo ratings yet
- Toxicology For Activists: Romeo F. Quijano, M.DDocument87 pagesToxicology For Activists: Romeo F. Quijano, M.DRomeo QuijanoNo ratings yet
- Basic Clinical ToxicologyDocument21 pagesBasic Clinical ToxicologyPana NicolaeNo ratings yet
- T o X I C o L o G yDocument7 pagesT o X I C o L o G yDennis ValdezNo ratings yet
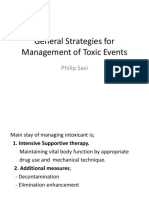
- General Strategies For Management of Toxic EventsDocument78 pagesGeneral Strategies For Management of Toxic EventsMusa yohanaNo ratings yet
- Basic Principles of Toxicology NotesDocument15 pagesBasic Principles of Toxicology NotesKoki KingNo ratings yet
- CLINICAL ToxicologyDocument29 pagesCLINICAL Toxicologykkrriissyy_0625No ratings yet
- Poisoning in ChildrenDocument44 pagesPoisoning in ChildrenYohanes FirmansyahNo ratings yet
- Week 10 - Forensic ChemistryDrugsToxicologyDocument120 pagesWeek 10 - Forensic ChemistryDrugsToxicologycuambyahoo100% (1)
- Nursing PcolDocument34 pagesNursing PcolRazell Jean ArazaNo ratings yet
- Pcol 211 Prelims ALL inDocument413 pagesPcol 211 Prelims ALL inPaula LouiseNo ratings yet
- Revision of PharmacokineticsDocument135 pagesRevision of Pharmacokineticsahmd25sfNo ratings yet
- ToxicologyDocument8 pagesToxicologybernalhoneylethjhoy06No ratings yet
- GENERAL PHARMACOLOGY - Part 1 PDFDocument49 pagesGENERAL PHARMACOLOGY - Part 1 PDFMohamad Mostafa100% (4)
- PoisoningDocument89 pagesPoisoningrosana james100% (1)
- PHPY 304 Study MidtermDocument31 pagesPHPY 304 Study Midtermbimal06khanalNo ratings yet
- CHP 1Document9 pagesCHP 1Nida RidzuanNo ratings yet
- TOXICOLOGYDocument26 pagesTOXICOLOGYPrashant Meena100% (1)
- Forensic Toxicology: By: Rosemarie D. Cosue, Ed.DDocument18 pagesForensic Toxicology: By: Rosemarie D. Cosue, Ed.DAubreyNo ratings yet
- Unit 2 Poisons FinalDocument12 pagesUnit 2 Poisons FinalNived K KNo ratings yet
- Toxicology: WEEK 6-8Document29 pagesToxicology: WEEK 6-8Cariza Anda0% (1)
- Tutorial Report 1 Scenario: Wivan Havilian Djohan 1418011223Document16 pagesTutorial Report 1 Scenario: Wivan Havilian Djohan 1418011223Wivan Havilian DjohanNo ratings yet
- Homo ToxicologyDocument279 pagesHomo ToxicologyRafael MontavaNo ratings yet
- PharmacologyDocument52 pagesPharmacologyKris Ann Yap-BonillaNo ratings yet
- Pharm Overview Flashcards - QuizletDocument7 pagesPharm Overview Flashcards - QuizletJulianaMorallesNo ratings yet
- Classification of PoisonsDocument73 pagesClassification of PoisonspikachuNo ratings yet
- Tuberculosis: Robert L. Copeland, JR., PH.DDocument43 pagesTuberculosis: Robert L. Copeland, JR., PH.Dkristine umamingNo ratings yet
- Group Interative Art TherapyDocument225 pagesGroup Interative Art TherapyRibeiro CatarinaNo ratings yet
- Positioning Strategy - Mineral WaterDocument2 pagesPositioning Strategy - Mineral WaterRakesh SelvamNo ratings yet
- (Jill E. Thistlethwaite) Values-Based Interprofess (B-Ok - CC)Document192 pages(Jill E. Thistlethwaite) Values-Based Interprofess (B-Ok - CC)Ria Qadariah AriefNo ratings yet
- Economics Half Yearly Question PaperDocument6 pagesEconomics Half Yearly Question PaperBhumika MiglaniNo ratings yet
- NFPA 25 2011 Sprinkler Inspection TableDocument2 pagesNFPA 25 2011 Sprinkler Inspection TableHermes VacaNo ratings yet
- MPX-200 Service Manual PDFDocument90 pagesMPX-200 Service Manual PDFvivijaNo ratings yet
- Continuous Microbiological Environmental Monitoring For Process Understanding and Reduced Interventions in Aseptic ManufacturingDocument44 pagesContinuous Microbiological Environmental Monitoring For Process Understanding and Reduced Interventions in Aseptic ManufacturingTorres Xia100% (1)
- Expressions of QuantityDocument5 pagesExpressions of Quantitybenilde bastidaNo ratings yet
- HOME TECH - HOME TEXTILE REVIEW. Ayman SatopayDocument12 pagesHOME TECH - HOME TEXTILE REVIEW. Ayman SatopayAyman SatopayNo ratings yet
- Dig Inn Early Summer MenuDocument2 pagesDig Inn Early Summer MenuJacqueline CainNo ratings yet
- Executive SummaryDocument2 pagesExecutive Summarykulsoomalam100% (1)
- Labor EstimateDocument26 pagesLabor EstimateAngelica CabreraNo ratings yet
- Ott OTT Ecolog 1000 Water Level LoggerDocument3 pagesOtt OTT Ecolog 1000 Water Level LoggerNedimZ1No ratings yet
- Guarantor Indemnity For Illness or DeathDocument2 pagesGuarantor Indemnity For Illness or Deathlajaun hindsNo ratings yet
- LTHE Comments On APG's Proposal No. 9090/3181-L&T-Detailed Engineering Services For EPCC-1-AVU Unit, Barauni RefineryDocument9 pagesLTHE Comments On APG's Proposal No. 9090/3181-L&T-Detailed Engineering Services For EPCC-1-AVU Unit, Barauni RefineryajayNo ratings yet
- Research Essay Final Draft 1Document4 pagesResearch Essay Final Draft 1api-614550036No ratings yet
- Contoh Reflection PaperDocument2 pagesContoh Reflection PaperClaudia KandowangkoNo ratings yet
- Diagnostic Evaluation and Management of The Solitary Pulmonary NoduleDocument21 pagesDiagnostic Evaluation and Management of The Solitary Pulmonary NoduleGonzalo Leal100% (1)
- Employee Leave PolicyDocument3 pagesEmployee Leave Policyladdu30No ratings yet
- Prestress 3.0Document10 pagesPrestress 3.0Jonel CorbiNo ratings yet
- Untitled Form - Google Forms00Document3 pagesUntitled Form - Google Forms00Ericka Rivera SantosNo ratings yet
- 120-202 Lab Manual Spring 2012Document107 pages120-202 Lab Manual Spring 2012evacelon100% (1)
- Kmart PDFDocument105 pagesKmart PDFkaranbhayaNo ratings yet
- Thai Book Lesson From Genius SchoolDocument85 pagesThai Book Lesson From Genius SchoolAlexis L.D (Riker94)No ratings yet
- Canfield FairDocument3 pagesCanfield Fairapi-546463844No ratings yet
- Molarity, Molality, Normality, and Mass Percent Worksheet II Answer Key 11-12 PDFDocument3 pagesMolarity, Molality, Normality, and Mass Percent Worksheet II Answer Key 11-12 PDFGerald KamulanjeNo ratings yet
- Ems em FW Paneel Firetec enDocument2 pagesEms em FW Paneel Firetec enzlatkokrsicNo ratings yet
- ListwarehouseDocument1 pageListwarehouseKautilya KalyanNo ratings yet
- Ryder Quotation 2012.7.25Document21 pagesRyder Quotation 2012.7.25DarrenNo ratings yet
- Art of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionFrom EverandArt of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionRating: 3 out of 5 stars3/5 (1)
- Desperate: An Epic Battle for Clean Water and Justice in AppalachiaFrom EverandDesperate: An Epic Battle for Clean Water and Justice in AppalachiaRating: 4 out of 5 stars4/5 (1)
- Waste: One Woman’s Fight Against America’s Dirty SecretFrom EverandWaste: One Woman’s Fight Against America’s Dirty SecretRating: 5 out of 5 stars5/5 (1)
- The Cyanide Canary: A True Story of InjusticeFrom EverandThe Cyanide Canary: A True Story of InjusticeRating: 4 out of 5 stars4/5 (52)
- Slow Violence and the Environmentalism of the PoorFrom EverandSlow Violence and the Environmentalism of the PoorRating: 4 out of 5 stars4/5 (5)
- Busted!: Drug War Survival Skills and True Dope DFrom EverandBusted!: Drug War Survival Skills and True Dope DRating: 3.5 out of 5 stars3.5/5 (7)
- The Rights of Nature: A Legal Revolution That Could Save the WorldFrom EverandThe Rights of Nature: A Legal Revolution That Could Save the WorldRating: 5 out of 5 stars5/5 (1)
- Exposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle Against DuPontFrom EverandExposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle Against DuPontRating: 4.5 out of 5 stars4.5/5 (18)
- 3rd Grade Science: Life Sciences in Eco Systems | Textbook EditionFrom Everand3rd Grade Science: Life Sciences in Eco Systems | Textbook EditionNo ratings yet
- Reduce, Reuse and Recycle : The Secret to Environmental Sustainability : Environment Textbooks | Children's Environment BooksFrom EverandReduce, Reuse and Recycle : The Secret to Environmental Sustainability : Environment Textbooks | Children's Environment BooksNo ratings yet
- The Intersection of Intellectual Property Law and the “Green” Movement: RIPL’s Green Issue 2010From EverandThe Intersection of Intellectual Property Law and the “Green” Movement: RIPL’s Green Issue 2010Rating: 5 out of 5 stars5/5 (2)
- Environmental Education in Practice: Concepts and ApplicationsFrom EverandEnvironmental Education in Practice: Concepts and ApplicationsNo ratings yet
- Down to the Wire: Confronting Climate CollapseFrom EverandDown to the Wire: Confronting Climate CollapseRating: 4.5 out of 5 stars4.5/5 (8)
- Land Divided by Law: The Yakama Indian Nation as Environmental History, 1840-1933From EverandLand Divided by Law: The Yakama Indian Nation as Environmental History, 1840-1933No ratings yet
- Ecosystem Facts That You Should Know - The Forests Edition - Nature Picture Books | Children's Nature BooksFrom EverandEcosystem Facts That You Should Know - The Forests Edition - Nature Picture Books | Children's Nature BooksNo ratings yet
- Dawn at Mineral King Valley: The Sierra Club, the Disney Company, and the Rise of Environmental LawFrom EverandDawn at Mineral King Valley: The Sierra Club, the Disney Company, and the Rise of Environmental LawRating: 4 out of 5 stars4/5 (334)
- Principles of direct and superior responsibility in international humanitarian lawFrom EverandPrinciples of direct and superior responsibility in international humanitarian lawNo ratings yet