You might also like
- High Yield PsychiatryDocument44 pagesHigh Yield PsychiatryAntony Awad100% (2)
- Comquest NotesDocument58 pagesComquest NotesBhumiShahNo ratings yet
- HighYieldPsychiatry PDFDocument43 pagesHighYieldPsychiatry PDFYay100% (4)
- Step 3 DiagramDocument11 pagesStep 3 DiagramJorge Luis Lopez100% (2)
- Step-2-Ck-Notes-Syrian-Student - HTML: Cardiology UWDocument15 pagesStep-2-Ck-Notes-Syrian-Student - HTML: Cardiology UWLoyla RoseNo ratings yet
- Usmle Step 2 CsDocument70 pagesUsmle Step 2 CsAlvi MuldaniNo ratings yet
- 11 Blues Piano Voicings AnalysisDocument11 pages11 Blues Piano Voicings AnalysisBHNo ratings yet
- Skan's Step 3 CocktailDocument82 pagesSkan's Step 3 CocktailVS100% (6)
- USMLE Step 2 CK Bible 2nd EdDocument435 pagesUSMLE Step 2 CK Bible 2nd EdShyama SharmaNo ratings yet
- Sports MedicineDocument32 pagesSports Medicinersimranjit100% (1)
- Sports MedicineDocument32 pagesSports Medicinersimranjit100% (1)
- PracticeExam CCSDocument12 pagesPracticeExam CCSBehrouz Yari75% (4)
- The Weill Cornell Clerkship Guide - FinalDocument24 pagesThe Weill Cornell Clerkship Guide - FinalDavid Chang100% (1)
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Application For Post-Conviction Relief, State of Louisiana vs. Vincent SimmonsDocument54 pagesApplication For Post-Conviction Relief, State of Louisiana vs. Vincent SimmonsThe Town TalkNo ratings yet
- Step 3 NotesDocument20 pagesStep 3 NotesHunter Ross100% (1)
- USMLE STEP 3 EXAM GuideDocument5 pagesUSMLE STEP 3 EXAM Guidekwpang10% (3)
- Objectives IMDocument104 pagesObjectives IMlaraNo ratings yet
- Jean Genet - Deathwatch-Faber & Faber (1961) PDFDocument38 pagesJean Genet - Deathwatch-Faber & Faber (1961) PDFValentin MarcosNo ratings yet
- CCS RheumatologyDocument3 pagesCCS RheumatologyMostafa Mahmoud ElsebeyNo ratings yet
- 2009 Pearl SheetDocument19 pages2009 Pearl Sheetmikez100% (1)
- Combank NotesDocument7 pagesCombank NotesVee MendNo ratings yet
- Preventive MedicineDocument17 pagesPreventive MedicinersimranjitNo ratings yet
- Preventive MedicineDocument17 pagesPreventive MedicinersimranjitNo ratings yet
- Step 3 Lecture Notes - CompleteDocument834 pagesStep 3 Lecture Notes - CompletetreezeeMD100% (3)
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Step 3 CCS OutlineDocument10 pagesStep 3 CCS OutlineDuncan Jackson100% (2)
- Step 2 CKDocument92 pagesStep 2 CKazankhan99No ratings yet
- My NotesDocument24 pagesMy NotesrsimranjitNo ratings yet
- Kripal, Debating The Mystical As The Ethical: An Indological Map, in Crossing Boundaries: Essays On The Ethical Status of Mysticism (2002) : 15-69Document28 pagesKripal, Debating The Mystical As The Ethical: An Indological Map, in Crossing Boundaries: Essays On The Ethical Status of Mysticism (2002) : 15-69Keren MiceNo ratings yet
- Biostatistics Step 3 NotesDocument17 pagesBiostatistics Step 3 Notesrsimranjit100% (1)
- An Insight Into Step 3Document4 pagesAn Insight Into Step 3SpencerNo ratings yet
- Step 2 CK PT SafetyDocument3 pagesStep 2 CK PT SafetyAhmed100% (3)
- High Yield Surgery Compatible VersionDocument77 pagesHigh Yield Surgery Compatible VersionManish K100% (1)
- Uw Ccs Blog CasesDocument5 pagesUw Ccs Blog Cases808kailuaNo ratings yet
- Step3 Sample ItemsDocument81 pagesStep3 Sample Itemsedi büdü100% (1)
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- Brosencephalon's Internal MedicineDocument340 pagesBrosencephalon's Internal Medicinejtsk2100% (1)
- How To Score 99 On Step 3 UsmleDocument2 pagesHow To Score 99 On Step 3 Usmlepreepree190% (3)
- All Notes Prepared Summed Up PDFDocument326 pagesAll Notes Prepared Summed Up PDFrsimranjitNo ratings yet
- Arlete S Notes PDFDocument28 pagesArlete S Notes PDFjrabeNo ratings yet
- KHALIL High Yeild Usmle Step 2 CS Mnemonic PDFDocument19 pagesKHALIL High Yeild Usmle Step 2 CS Mnemonic PDFPok LyhongNo ratings yet
- Dr. Waqas Ayubian Notes For Step 3Document772 pagesDr. Waqas Ayubian Notes For Step 3Muhammad HammadNo ratings yet
- My Step 3 228 Experience:: Materials UsedDocument2 pagesMy Step 3 228 Experience:: Materials UsedRicardoMelendez0% (1)
- CardiologyDocument8 pagesCardiologykhalidzubairiNo ratings yet
- Medical Students AmnesiaDocument37 pagesMedical Students AmnesiaMarie SantoroNo ratings yet
- Business Combination 2Document3 pagesBusiness Combination 2Jamie RamosNo ratings yet
- Pages From First Aid (USMLE Step1) (2019)Document6 pagesPages From First Aid (USMLE Step1) (2019)George Russell0% (1)
- Rotating Machinery 3d TutorialDocument14 pagesRotating Machinery 3d Tutorialأسامةبوعزيز100% (1)
- Previous Exam by System FullDocument26 pagesPrevious Exam by System FullMostafa Mahmoud ElsebeyNo ratings yet
- Step 3 General Medicine Part 1 of 2Document10 pagesStep 3 General Medicine Part 1 of 2Bhavin ChoksiNo ratings yet
- USMLE Step 2 CK: CMS: Psychiatry Form 3Document17 pagesUSMLE Step 2 CK: CMS: Psychiatry Form 3usmleaddict pro57% (7)
- High Yield Pediatrics: Shelf Exam Review Emma Holliday RamahiDocument78 pagesHigh Yield Pediatrics: Shelf Exam Review Emma Holliday Ramahiskeebs230% (1)
- Form 1Document108 pagesForm 1Asim MohamedNo ratings yet
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3Rating: 5 out of 5 stars5/5 (1)
- Step3 Sample ItemsDocument71 pagesStep3 Sample ItemsxiaojianNo ratings yet
- Psych Notes For The ShelfDocument1 pagePsych Notes For The Shelfbostickdrew16No ratings yet
- CK in 10 Weeks - Sara A K 261Document3 pagesCK in 10 Weeks - Sara A K 261Muhammad Bilal100% (2)
- Divine Interventions - Military Podcast 231Document1 pageDivine Interventions - Military Podcast 231María Camila Pareja ZabalaNo ratings yet
- USMLE Step 2 Treatment NotesDocument13 pagesUSMLE Step 2 Treatment NotesKatherine SullivanNo ratings yet
- CMS NBME IM 4 With AnswersDocument52 pagesCMS NBME IM 4 With AnswersZen PrepNo ratings yet
- USPSTF RecommendationsDocument3 pagesUSPSTF RecommendationsKevinMathewNo ratings yet
- Main ICM Shelf Exam (2012 Nov MUA)Document8 pagesMain ICM Shelf Exam (2012 Nov MUA)mentawistNo ratings yet
- 2015 Step2CK SampleItemsDocument40 pages2015 Step2CK SampleItemspreethamNo ratings yet
- Neurology Shelf Exam Review - Part 4Document11 pagesNeurology Shelf Exam Review - Part 4CoolrobertizNo ratings yet
- Michael W, Comat ImDocument63 pagesMichael W, Comat ImSeanNo ratings yet
- Unfilled Programs by State: Reproduction Is Prohibited Without The Written Consent of The NRMP ®Document18 pagesUnfilled Programs by State: Reproduction Is Prohibited Without The Written Consent of The NRMP ®rsimranjitNo ratings yet
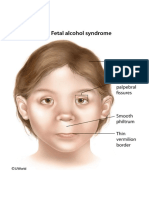
- Fetal Alcohol SyndromeDocument1 pageFetal Alcohol SyndromersimranjitNo ratings yet
- USMLE World BlocksDocument1 pageUSMLE World BlocksrsimranjitNo ratings yet
- Coping Mechanism IIDocument7 pagesCoping Mechanism IIEllaNo ratings yet
- NovelDocument2 pagesNovelBlnd RahimNo ratings yet
- De La Salle University Manila: EthicsDocument16 pagesDe La Salle University Manila: EthicsMelyssa Dawn GullonNo ratings yet
- 1-Data UnderstandingDocument21 pages1-Data UnderstandingMahander OadNo ratings yet
- What Is Decision Making - McKinseyDocument10 pagesWhat Is Decision Making - McKinseyPhuc ThienNo ratings yet
- Crimson Wine GroupDocument8 pagesCrimson Wine Groupnikhil_shamapantNo ratings yet
- 04.chapter 1 What For Business EthicsDocument36 pages04.chapter 1 What For Business EthicsSorina SirbuNo ratings yet
- Trump Presidency 38 - June 20th, 2018 To July 14th, 2018Document501 pagesTrump Presidency 38 - June 20th, 2018 To July 14th, 2018FW040No ratings yet
- Food Fantasy Food Soul GuideDocument8 pagesFood Fantasy Food Soul GuideanakinNo ratings yet
- Competency Checklist For CparDocument2 pagesCompetency Checklist For CparChristine Marie A Llanera-CadalloNo ratings yet
- ECS 202301 Lecture 5 2Document35 pagesECS 202301 Lecture 5 2Rhinndhi SakthyvelNo ratings yet
- Maldigestion/malabsorption Syndromes: Fecal AnalysisDocument2 pagesMaldigestion/malabsorption Syndromes: Fecal AnalysisMonica DomingoNo ratings yet
- London Property BondDocument40 pagesLondon Property BondhyenadogNo ratings yet
- CBSE Class 2 EVS Our FestivalsDocument3 pagesCBSE Class 2 EVS Our FestivalsRakesh Agarwal100% (1)
- Personal Case Analysis StructureDocument6 pagesPersonal Case Analysis Structureapi-563430228No ratings yet
- 4.-Content Based LearningDocument3 pages4.-Content Based LearningLuis Paz100% (1)
- Income and Cross Elasticity of DemandDocument14 pagesIncome and Cross Elasticity of DemandSayam Roy100% (1)
- Gateway Electronics vs. AsianbankDocument26 pagesGateway Electronics vs. Asianbankpoiuytrewq911550% (2)
- Evaluation Form MSCDocument5 pagesEvaluation Form MSCvikash kumarNo ratings yet
- Dicision MakingDocument34 pagesDicision MakingArpita PatelNo ratings yet
- PerceptionDocument17 pagesPerceptionAnuj SharmaNo ratings yet
- Leif Eriksson-Annotated BibDocument7 pagesLeif Eriksson-Annotated Bibapi-308958050No ratings yet
- 2023 BWIA 121 ReaderDocument293 pages2023 BWIA 121 ReaderIrfaan CassimNo ratings yet
- SNS CFE 102 0830 Religious Involvement 1 Paraan JoshuaDocument1 pageSNS CFE 102 0830 Religious Involvement 1 Paraan JoshuaLara May BasiladNo ratings yet