You might also like
- Starving Cancer Cells: Evidence-Based Strategies to Slow Cancer Progression: A Selection of Readings for Health Services ProvidersFrom EverandStarving Cancer Cells: Evidence-Based Strategies to Slow Cancer Progression: A Selection of Readings for Health Services ProvidersNo ratings yet
- Molecular Diagnostics and Treatment of Pancreatic Cancer: Systems and Network Biology ApproachesFrom EverandMolecular Diagnostics and Treatment of Pancreatic Cancer: Systems and Network Biology ApproachesNo ratings yet
- MainDocument17 pagesMainMohammed KhalidNo ratings yet
- Targeting The Gut Microbiome An Emerging Trend in Hematopoietic StemDocument14 pagesTargeting The Gut Microbiome An Emerging Trend in Hematopoietic Stemeliseoo8ortegaNo ratings yet
- Human Gut Microbiota and Gastrointestinal CancerDocument39 pagesHuman Gut Microbiota and Gastrointestinal Canceryalocim666No ratings yet
- Articulo de Disbiosis en Ca Colorectal 2018Document12 pagesArticulo de Disbiosis en Ca Colorectal 2018Jenny Abad DermatologaNo ratings yet
- Vip CVD Con ImagenesDocument22 pagesVip CVD Con ImagenesMarc Vilalta ParraNo ratings yet
- The gut-liver axis and the intersection with the microbiomeDocument36 pagesThe gut-liver axis and the intersection with the microbiomeRafly AndiNo ratings yet
- Microorganisms 09 01021Document24 pagesMicroorganisms 09 01021Alice de MoraesNo ratings yet
- Drobner Et Al 2023 Examining The Role of Microbiota Centered Interventions in Cancer Therapeutics Applications ForDocument10 pagesDrobner Et Al 2023 Examining The Role of Microbiota Centered Interventions in Cancer Therapeutics Applications Fordr.tonichenNo ratings yet
- Intestinal phages interact with bacteria and are involved in human diseasesDocument24 pagesIntestinal phages interact with bacteria and are involved in human diseasesafyyynyhNo ratings yet
- Microbiota Manipulation With Prebiotics and Probiotics in Patients Undergoing Stem Cell TransplantationDocument10 pagesMicrobiota Manipulation With Prebiotics and Probiotics in Patients Undergoing Stem Cell TransplantationAlexa CofréNo ratings yet
- Fonc 12 897330Document7 pagesFonc 12 897330ads asdNo ratings yet
- Cancers 11 00038Document26 pagesCancers 11 00038JK NUTRISIERVICENo ratings yet
- Ol 18 1 487 PDFDocument12 pagesOl 18 1 487 PDFCasiana GuiNo ratings yet
- Gut Microbiota-Derived Epigenetic Alterations During Onset of DiseasesDocument11 pagesGut Microbiota-Derived Epigenetic Alterations During Onset of DiseasesDiamondChuNo ratings yet
- Biomedicines 12 00703 v2Document19 pagesBiomedicines 12 00703 v2jamel-shamsNo ratings yet
- Ajpgi 00008 2022Document18 pagesAjpgi 00008 2022Jéssica Thandara GosseNo ratings yet
- Biliary Tract Cancers: Epidemiology, Molecular Pathogenesis and Genetic Risk AssociationsDocument31 pagesBiliary Tract Cancers: Epidemiology, Molecular Pathogenesis and Genetic Risk AssociationsleartaNo ratings yet
- Critical Reviews in Oncology / Hematology: F. Bozzetti, Z. Stanga TDocument12 pagesCritical Reviews in Oncology / Hematology: F. Bozzetti, Z. Stanga TshangrilaNo ratings yet
- Scorpion Venom Shows Promise in Cancer TreatmentDocument11 pagesScorpion Venom Shows Promise in Cancer TreatmentSaifuddin SidikiNo ratings yet
- Bacteroides, Butyric Acid and t10, c12 CLA: Changes in Colorectal Adenomatous Polyp PatientsDocument9 pagesBacteroides, Butyric Acid and t10, c12 CLA: Changes in Colorectal Adenomatous Polyp PatientsMuhammad Haksan PratamaNo ratings yet
- Gut Microbiome Modulates Efficacy of Immune Checkpoint InhibitorsDocument10 pagesGut Microbiome Modulates Efficacy of Immune Checkpoint InhibitorsGusti FerriNo ratings yet
- Nihms 1768792Document35 pagesNihms 1768792Mohammed KhalidNo ratings yet
- Human Gastric Cancer, Helicobacter Pylori and Bracken CarcinogensDocument9 pagesHuman Gastric Cancer, Helicobacter Pylori and Bracken CarcinogensJorge Luis Avila NúñezNo ratings yet
- Role of Gut Microbiota in Cardiovascular DiseasesDocument14 pagesRole of Gut Microbiota in Cardiovascular DiseasesElson TavaresNo ratings yet
- Nutri GenomicDocument8 pagesNutri Genomicmiguel salasNo ratings yet
- Molecular Systems Biology - 2022 - Niu - Dynamic Human Liver Proteome Atlas Reveals Functional Insights Into DiseaseDocument24 pagesMolecular Systems Biology - 2022 - Niu - Dynamic Human Liver Proteome Atlas Reveals Functional Insights Into DiseaseImteaz Ahmed MinhazNo ratings yet
- Mikroba KankerDocument32 pagesMikroba KankerSilpi HamidiyahNo ratings yet
- The Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringDocument5 pagesThe Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringMariaNo ratings yet
- Metabolic Reprogramming Due To Hypoxia in Pancreatic Can - 2021 - BiomedicineDocument14 pagesMetabolic Reprogramming Due To Hypoxia in Pancreatic Can - 2021 - BiomedicineAkhmad BajuriNo ratings yet
- HHS Public Access: The Role of Intestinal Bacteria in The Development and Progression of Gastrointestinal Tract NeoplasmsDocument22 pagesHHS Public Access: The Role of Intestinal Bacteria in The Development and Progression of Gastrointestinal Tract NeoplasmsRita FauziaNo ratings yet
- Assessment of clinical variables as predictive markers in the development and progression of colorectal cancer BY Sulayman WaquarDocument11 pagesAssessment of clinical variables as predictive markers in the development and progression of colorectal cancer BY Sulayman WaquarsulaymanwaquarNo ratings yet
- Bile Acids at The Cross-Roads of Gut Microbiome-Host Cardiometabolic InteractionsDocument12 pagesBile Acids at The Cross-Roads of Gut Microbiome-Host Cardiometabolic Interactionskarimsamihaddad1234No ratings yet
- Using Data Science For Medical Decision Making Case: Role of Gut Microbiome in Multiple SclerosisDocument11 pagesUsing Data Science For Medical Decision Making Case: Role of Gut Microbiome in Multiple SclerosisUhtredNo ratings yet
- nihms-942943Document27 pagesnihms-942943Wojciech WawrętyNo ratings yet
- 10 1016@j Biopha 2019 109142Document13 pages10 1016@j Biopha 2019 109142CoNo ratings yet
- BBA - Reviews On Cancer: ReviewDocument22 pagesBBA - Reviews On Cancer: ReviewAnonymous iyEXSANo ratings yet
- R4. 2020 Critical Reviews in OncogenesisDocument14 pagesR4. 2020 Critical Reviews in OncogenesissathishNo ratings yet
- Fcimb 10 587628Document16 pagesFcimb 10 587628pandi pandNo ratings yet
- 2018 Article 193Document31 pages2018 Article 193pedroNo ratings yet
- Fimmu 13 932228Document25 pagesFimmu 13 932228Liliana SiriteanuNo ratings yet
- Cancer and the Gut Microbiota LinkDocument10 pagesCancer and the Gut Microbiota LinkEmilio AlaquàsNo ratings yet
- Seminario 2Document7 pagesSeminario 2andreaNo ratings yet
- Using Gut Microbiota As A Diagnostic Tool For Colorectal Cancer Machine Learning Techniques Reveal Promising Results CompressDocument12 pagesUsing Gut Microbiota As A Diagnostic Tool For Colorectal Cancer Machine Learning Techniques Reveal Promising Results CompressphopicsignerNo ratings yet
- tmp90DB TMPDocument7 pagestmp90DB TMPFrontiersNo ratings yet
- Microbiota in Mesenteric Adipose Tissue From Crohn 'S Disease Promote Colitis in MiceDocument14 pagesMicrobiota in Mesenteric Adipose Tissue From Crohn 'S Disease Promote Colitis in Mice柳奕诚No ratings yet
- Pancreatic CancerDocument13 pagesPancreatic CancerFA MonterNo ratings yet
- Jurnal ManggisDocument22 pagesJurnal ManggisAyundaNo ratings yet
- Hydrogen Inhibits The Proliferation and Migration of Gastric Cancer Cells by Modulating Lncrna Malat1/Mir-124-3P/ Ezh2 AxisDocument10 pagesHydrogen Inhibits The Proliferation and Migration of Gastric Cancer Cells by Modulating Lncrna Malat1/Mir-124-3P/ Ezh2 AxisGermán Isacc PazmiñoNo ratings yet
- R3. 2020 Liver Cancer InternationalDocument10 pagesR3. 2020 Liver Cancer InternationalsathishNo ratings yet
- 0300060520925693Document11 pages0300060520925693Narjes Sharif AskariNo ratings yet
- Erc EndocrinologyDocument11 pagesErc EndocrinologyEsti Nur EkasariNo ratings yet
- Biomedicines 05 00058Document17 pagesBiomedicines 05 00058heidyNo ratings yet
- (Current Cancer Research) Erle S. Robertson - Microbiome and Cancer-Springe PDFDocument406 pages(Current Cancer Research) Erle S. Robertson - Microbiome and Cancer-Springe PDFmariomgNo ratings yet
- Nanoparticle-Induced Vascular Blockade in Human Prostate CancerDocument11 pagesNanoparticle-Induced Vascular Blockade in Human Prostate CancerMr-Mohamed AliNo ratings yet
- Colorectal CarcinomaDocument9 pagesColorectal CarcinomaKantona FrankNo ratings yet
- Koosha DKK., 2016Document12 pagesKoosha DKK., 2016Yunus Abdullah FatahNo ratings yet
- Ijph 48 632Document12 pagesIjph 48 632Reni WulandariNo ratings yet
- Microbiota Effects On Cancer: From Risks To Therapies: Oncotarget, 2018, Vol. 9, (No. 25), PP: 17915-17927Document13 pagesMicrobiota Effects On Cancer: From Risks To Therapies: Oncotarget, 2018, Vol. 9, (No. 25), PP: 17915-17927mutia gondrongNo ratings yet
- Widespread protein lysine acetylation in gut microbiome and its alterations in patients with Crohn’s diseaseDocument12 pagesWidespread protein lysine acetylation in gut microbiome and its alterations in patients with Crohn’s diseaseMartinaNo ratings yet
- Safety, Clinical Response, and Microbiome Findings Following Fecal Microbiota Transplant in Children With Inflammatory Bowel DiseaseDocument12 pagesSafety, Clinical Response, and Microbiome Findings Following Fecal Microbiota Transplant in Children With Inflammatory Bowel DiseaseMartinaNo ratings yet
- Fecal microbiota transplant for Crohn disease_ ADocument8 pagesFecal microbiota transplant for Crohn disease_ AMartinaNo ratings yet
- Microbiome in Sjögren’s syndrome_ here we areDocument2 pagesMicrobiome in Sjögren’s syndrome_ here we areMartinaNo ratings yet
- Iron fortification adversely affects the gut ..Document12 pagesIron fortification adversely affects the gut ..MartinaNo ratings yet
- The relationship between fecal bile acids and microbiome counityDocument12 pagesThe relationship between fecal bile acids and microbiome counityMartinaNo ratings yet
- A Comparative Proteomic Analysis of Erinacine A’s Inhibition of Gastric Cancer Cell Viability and InvasivenessDocument14 pagesA Comparative Proteomic Analysis of Erinacine A’s Inhibition of Gastric Cancer Cell Viability and InvasivenessMartinaNo ratings yet
- A Microbiome Foundation for the Study of Crohn’s DiseaseDocument4 pagesA Microbiome Foundation for the Study of Crohn’s DiseaseMartinaNo ratings yet
- Decreased Fecal Calprotectin Levels in Cystic Fibrosis Patients After Antibiotic Treatment for Respiratory ExacerbationDocument3 pagesDecreased Fecal Calprotectin Levels in Cystic Fibrosis Patients After Antibiotic Treatment for Respiratory ExacerbationMartinaNo ratings yet
- Assessment of complementary feeding of Canadian infants_ effects on microbiome & oxidative stress, a randomized controlled trialDocument12 pagesAssessment of complementary feeding of Canadian infants_ effects on microbiome & oxidative stress, a randomized controlled trialMartinaNo ratings yet
- Fecal calprotectin and fecal indole predict outcome of fecalDocument4 pagesFecal calprotectin and fecal indole predict outcome of fecalMartinaNo ratings yet
- Molecules: Ffects of Rich in B-Glucans Edible MushroomsDocument25 pagesMolecules: Ffects of Rich in B-Glucans Edible Mushroomsharry potterNo ratings yet
- Blastocystis Gut MicrobiomeDocument18 pagesBlastocystis Gut MicrobiomeFreddy FranklinNo ratings yet
- The Gut Microbiome as a Target for IBD Treatment_ Are We There YetDocument12 pagesThe Gut Microbiome as a Target for IBD Treatment_ Are We There YetMartinaNo ratings yet
- A223 THE GEM PROJECT_ ASSOCIATIONS OF DIETARY PATTERNS WITH MICROBIOME AND FECAL CALPROTECTIN IN HEALTHY FIRST-DEGREE RELATIVES OF CROHN’S DISEASE PATIENTSDocument2 pagesA223 THE GEM PROJECT_ ASSOCIATIONS OF DIETARY PATTERNS WITH MICROBIOME AND FECAL CALPROTECTIN IN HEALTHY FIRST-DEGREE RELATIVES OF CROHN’S DISEASE PATIENTSMartinaNo ratings yet
- Microbiome risk profiles as biomarkers for inflammatory and metabolic disordersDocument15 pagesMicrobiome risk profiles as biomarkers for inflammatory and metabolic disordersMartinaNo ratings yet
- Hericium erinaceus, an amazing medicinal mushroomDocument24 pagesHericium erinaceus, an amazing medicinal mushroomMartinaNo ratings yet
- Polysaccharides from natural resources exhibit great potential in the treatment of ulcerative colitis_ A reviewDocument12 pagesPolysaccharides from natural resources exhibit great potential in the treatment of ulcerative colitis_ A reviewMartinaNo ratings yet
- Clinical and Physiological Perspectives of βGlucans in The Past, Present, and FutureDocument48 pagesClinical and Physiological Perspectives of βGlucans in The Past, Present, and FutureQualityMattersNo ratings yet
- the researchers to design, research, and develop new drugs forDocument19 pagesthe researchers to design, research, and develop new drugs forMartinaNo ratings yet
- Molecules: Ffects of Rich in B-Glucans Edible MushroomsDocument25 pagesMolecules: Ffects of Rich in B-Glucans Edible Mushroomsharry potterNo ratings yet
- izab277Document10 pagesizab277MartinaNo ratings yet
- the researchers to design, research, and develop new drugs forDocument19 pagesthe researchers to design, research, and develop new drugs forMartinaNo ratings yet
- A Review of the Effects of Natural compounds, medical plants, mushrooms on thegut microbiota and colitis and cancerDocument8 pagesA Review of the Effects of Natural compounds, medical plants, mushrooms on thegut microbiota and colitis and cancerMartinaNo ratings yet
- The Role of Gut Microbiota Biomodulators on mucosal imuniti and intestinal inflamationDocument24 pagesThe Role of Gut Microbiota Biomodulators on mucosal imuniti and intestinal inflamationMartinaNo ratings yet
- A Review of Mushrooms in Human Nutrition and HealthDocument14 pagesA Review of Mushrooms in Human Nutrition and HealthBegoña MartinezNo ratings yet
- Health benefits of edible mushroom polysaharidesand associated gut microbiota regulationDocument19 pagesHealth benefits of edible mushroom polysaharidesand associated gut microbiota regulationMartinaNo ratings yet
- Internal connections between dietary intake and gut microbiota homeostasis in disease progression of ulcerative colitis_a reviewDocument12 pagesInternal connections between dietary intake and gut microbiota homeostasis in disease progression of ulcerative colitis_a reviewMartinaNo ratings yet
- Recent developments in Hericium erinaceus polysaccharides_ extraction, purifacion,structur characterist and biology activityDocument21 pagesRecent developments in Hericium erinaceus polysaccharides_ extraction, purifacion,structur characterist and biology activityMartinaNo ratings yet
- Hipo HiperthyroidDocument49 pagesHipo HiperthyroidMuhammad Bilal Bin AmirNo ratings yet
- Photosynthesis, Cell Respiration, HomeostasisDocument9 pagesPhotosynthesis, Cell Respiration, HomeostasisTravis SatnarineNo ratings yet
- ClassificationDocument83 pagesClassificationDisha SharmaNo ratings yet
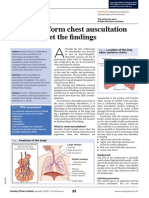
- Assessment On Respiratory ProblemsDocument7 pagesAssessment On Respiratory ProblemsSetiaty PandiaNo ratings yet
- MCQ HTNDocument18 pagesMCQ HTNmohamed mowafeyNo ratings yet
- © Kenneth Todar, PHD: (This Chapter Has 5 Pages)Document2 pages© Kenneth Todar, PHD: (This Chapter Has 5 Pages)sarahinaNo ratings yet
- Hema I Chapter 11 - RBC IndicesDocument15 pagesHema I Chapter 11 - RBC IndicesKumneger DereseNo ratings yet
- ORS Package InsertDocument2 pagesORS Package InsertJan Aira Almazan100% (1)
- VasectomyDocument1 pageVasectomyThyataira chuaNo ratings yet
- New PMDC Neb Format 2011Document28 pagesNew PMDC Neb Format 2011AliHazratNo ratings yet
- Slid CH13Document93 pagesSlid CH13Senior TitopecNo ratings yet
- Vanguard ROCC BrochureDocument2 pagesVanguard ROCC BrochureBobNo ratings yet
- Alere Cholestech LDX System User ManualDocument50 pagesAlere Cholestech LDX System User ManualRoberto NutiNo ratings yet
- Review Test For Final Exam PSY 250 Abnormal PsychologyDocument11 pagesReview Test For Final Exam PSY 250 Abnormal PsychologyJen CalaquiNo ratings yet
- 2nd Quarter PE NotesDocument9 pages2nd Quarter PE Notescasey lNo ratings yet
- AppendectomyDocument8 pagesAppendectomyDark AghanimNo ratings yet
- Learning TaskDocument4 pagesLearning TaskAngelica GuillermoNo ratings yet
- 2018 Non-Clinical Interventions For Reducing Unnecessary Caesarean Chen - Et - Al-2018-Cochrane - Database - of - Systematic - ReviewsDocument130 pages2018 Non-Clinical Interventions For Reducing Unnecessary Caesarean Chen - Et - Al-2018-Cochrane - Database - of - Systematic - ReviewsAli BahadırlıNo ratings yet
- Psych MedicationsDocument5 pagesPsych MedicationsKalesha Jones100% (2)
- Oxoid UTIDocument2 pagesOxoid UTISicoe AdrianNo ratings yet
- Occupational Therapy's Role in Managing ArthritisDocument2 pagesOccupational Therapy's Role in Managing ArthritisThe American Occupational Therapy AssociationNo ratings yet
- AMBU Mark IV e Mark IV Baby Partes e AcessoriosDocument1 pageAMBU Mark IV e Mark IV Baby Partes e AcessoriosNícolasNo ratings yet
- DownloadDocument1 pageDownloadsathish KumarNo ratings yet
- Unit Wise Question Will Come in Final Exam Unit 1: Q 2 ObjectivesDocument54 pagesUnit Wise Question Will Come in Final Exam Unit 1: Q 2 ObjectivesPoonam Yadav roll no.53No ratings yet
- Emma Sconyers, "I Carry You in My Heart: Facing An Incurable Prenatal Diagnosis"Document40 pagesEmma Sconyers, "I Carry You in My Heart: Facing An Incurable Prenatal Diagnosis"MIT Comparative Media Studies/WritingNo ratings yet
- Csa Book MRCGP Csa Cases MRCGP CourseDocument22 pagesCsa Book MRCGP Csa Cases MRCGP CourseEshtiag43% (7)
- Pediatric MCQ Questions on Neuropathies, Genitalia, Heart Defects and MoreDocument17 pagesPediatric MCQ Questions on Neuropathies, Genitalia, Heart Defects and MoreAhmed Kassem100% (1)
- Dr. Ralph Moss Interview: Medical Writer, Author, and FilmmakerDocument27 pagesDr. Ralph Moss Interview: Medical Writer, Author, and FilmmakerRosa AlvarezNo ratings yet
- 2021 - Neonatal Dermatology The Normal, The Common and The SeriousDocument14 pages2021 - Neonatal Dermatology The Normal, The Common and The SeriousnancyerlenNo ratings yet
- Histopathological and Biochemical, BhawnaDocument8 pagesHistopathological and Biochemical, BhawnaBhaskar ReddyNo ratings yet