You might also like
- Trigger Point Therapy for Myofascial Pain: The Practice of Informed TouchFrom EverandTrigger Point Therapy for Myofascial Pain: The Practice of Informed TouchRating: 4 out of 5 stars4/5 (5)
- Neuro Developmental Treatment (NDT) : Prepared By: Akhi Mony Clinical Physiotherapist (CPT) CRP-MirpurDocument24 pagesNeuro Developmental Treatment (NDT) : Prepared By: Akhi Mony Clinical Physiotherapist (CPT) CRP-MirpurAkhi MonyNo ratings yet
- Risk Assessment TemplateDocument3 pagesRisk Assessment TemplateGus VanGeijtenbeekNo ratings yet
- Manual Therapy For TMJ Dysfunction Furto Joshua WhitmanDocument9 pagesManual Therapy For TMJ Dysfunction Furto Joshua WhitmanYoan PereiraNo ratings yet
- Therapy in Temporomandibular DisorderDocument6 pagesTherapy in Temporomandibular DisorderHaryono zhuNo ratings yet
- Science Module 2q1Document16 pagesScience Module 2q1Michael Jorge BernalesNo ratings yet
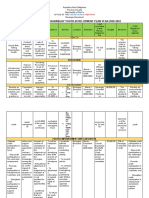
- Comprehensive Barangay Youth Development Plan Year 2020-2022Document7 pagesComprehensive Barangay Youth Development Plan Year 2020-2022ralf100% (1)
- NDT FinalDocument8 pagesNDT Finalapi-228136529No ratings yet
- Badel Michigan Splint and Treatment PDFDocument9 pagesBadel Michigan Splint and Treatment PDF謎超人No ratings yet
- Chapter 25Document63 pagesChapter 25Jœnríčk AzueloNo ratings yet
- Oral Myofunctional Therapy For The Treatment DTMDocument8 pagesOral Myofunctional Therapy For The Treatment DTMmartaNo ratings yet
- Natural History of Disease FINALDocument13 pagesNatural History of Disease FINALnadia nisarNo ratings yet
- STUDY MANUAL Planning Your Career in Business (V3)Document56 pagesSTUDY MANUAL Planning Your Career in Business (V3)Cristina IsbășescuNo ratings yet
- 1 (3) Effectivenes of Manual Therapy and Home Physical Therapy in Patients With Temporomandibular Disorders A Randomized Controlled Trial PDFDocument7 pages1 (3) Effectivenes of Manual Therapy and Home Physical Therapy in Patients With Temporomandibular Disorders A Randomized Controlled Trial PDFNur Azryani NaimNo ratings yet
- Interprofessional Collaboration in Dentistry: Role of Physiotherapists To Improve Care and Outcomes For Chronic Pain Conditions and Sleep DisordersDocument9 pagesInterprofessional Collaboration in Dentistry: Role of Physiotherapists To Improve Care and Outcomes For Chronic Pain Conditions and Sleep DisordersANTONIO ROMERONo ratings yet
- Management of TMJ DisorderDocument35 pagesManagement of TMJ DisorderSanjanaa ZadNo ratings yet
- Effects of Exercise Therapy On Painful Temporomandibular DisordersDocument7 pagesEffects of Exercise Therapy On Painful Temporomandibular DisordersLaura Espejo SalamancaNo ratings yet
- Management TMD by TRANSDocument14 pagesManagement TMD by TRANSnabila puspitaNo ratings yet
- FT. en EspasticidadDocument6 pagesFT. en Espasticidadrocioag87No ratings yet
- Iwasaki 2018Document10 pagesIwasaki 2018Natalie JaraNo ratings yet
- Calixtre 2015Document15 pagesCalixtre 2015Anderson RodriguesNo ratings yet
- Armijo-Olivo, 2016Document16 pagesArmijo-Olivo, 2016Jenniffer RamosNo ratings yet
- Manual Therapy: Systematic ReviewDocument8 pagesManual Therapy: Systematic ReviewArlen EvelyNo ratings yet
- Efficacy of Musculoeskeletal Manual Approach in The Treatment of Temporomandibulaar Joint DisorderDocument8 pagesEfficacy of Musculoeskeletal Manual Approach in The Treatment of Temporomandibulaar Joint DisorderLaura Espejo SalamancaNo ratings yet
- O Dfen 2012152 P 202Document26 pagesO Dfen 2012152 P 202Nugraha AnggaNo ratings yet
- Evaluación de La Eficacia A Corto Plazo de La Terapia Dolor MiofascialDocument8 pagesEvaluación de La Eficacia A Corto Plazo de La Terapia Dolor MiofascialGabriel DelgadoNo ratings yet
- A Comparative Study of Thai Massage and Muscle Energy - 2021 - Journal of BodywoDocument7 pagesA Comparative Study of Thai Massage and Muscle Energy - 2021 - Journal of BodywoDmytro ChopovskyiNo ratings yet
- 5Document10 pages5doctorhealthNo ratings yet
- Trestornos TemporomandibularesDocument6 pagesTrestornos TemporomandibularesESTEFANIA MATTOS MARINNo ratings yet
- 2021 Article 87265Document12 pages2021 Article 87265Anthony VillafañeNo ratings yet
- Journal of Bodywork & Movement Therapies: Søren T. Skou, Jonas B. ThorlundDocument6 pagesJournal of Bodywork & Movement Therapies: Søren T. Skou, Jonas B. ThorlundainunNo ratings yet
- Effectiveness of Manual Therapy and Cervical Spine Stretching Exercises On Pain and Disability in Myofascial Temporomandibular Disorders Accompanied by Headaches: A Single-Center Cohort StudyDocument11 pagesEffectiveness of Manual Therapy and Cervical Spine Stretching Exercises On Pain and Disability in Myofascial Temporomandibular Disorders Accompanied by Headaches: A Single-Center Cohort StudyJulioCesarGuillenNo ratings yet
- Odontogenic PainDocument6 pagesOdontogenic Painbnbmiller3100% (3)
- Case Report: Manual Therapy and Exercise To Improve Outcomes in Patients With Muscle Tension Dysphonia: A Case SeriesDocument12 pagesCase Report: Manual Therapy and Exercise To Improve Outcomes in Patients With Muscle Tension Dysphonia: A Case SeriesNicolas DiaconoNo ratings yet
- Cranio®: The Journal of Craniomandibular & Sleep PracticeDocument11 pagesCranio®: The Journal of Craniomandibular & Sleep PracticeAnthony VillafañeNo ratings yet
- Simona Tecco, D.D.S. Sergio Caputi, D.D.S. Stefano Teté, D.D.S. Giovanna Orsini, D.D.S. Felice Festa, M.D., D.D.S., M.S., PH.DDocument11 pagesSimona Tecco, D.D.S. Sergio Caputi, D.D.S. Stefano Teté, D.D.S. Giovanna Orsini, D.D.S. Felice Festa, M.D., D.D.S., M.S., PH.DFreddy BenalcázarNo ratings yet
- Fphar 11 596099Document17 pagesFphar 11 596099germanNo ratings yet
- 2002 - RCT - Nicolakis, P - Effectiveness of Exercise Therapy in Patients With Myofascial Pain Dysfunction SyndromeDocument7 pages2002 - RCT - Nicolakis, P - Effectiveness of Exercise Therapy in Patients With Myofascial Pain Dysfunction SyndromeAmaia MeiNo ratings yet
- Thai MassageDocument13 pagesThai MassageRima SekarNo ratings yet
- Journal of Electromyography and Kinesiology: M. Saccucci, S. Tecco, G. Ierardoa, V. Luzzi, F. Festa, A. PolimeniDocument7 pagesJournal of Electromyography and Kinesiology: M. Saccucci, S. Tecco, G. Ierardoa, V. Luzzi, F. Festa, A. PolimeniManena RivoltaNo ratings yet
- Soft Occlusal Splint Therapy in The Management of Myofascial Pain Dysfunction Syndrome: A Follow-Up Study in Kashmiri PopulationDocument7 pagesSoft Occlusal Splint Therapy in The Management of Myofascial Pain Dysfunction Syndrome: A Follow-Up Study in Kashmiri PopulationfilzahNo ratings yet
- Effectiveness of Direct Vs Indirect Technique Myofascial Release in The Management of Tensiontype HeadacheDocument5 pagesEffectiveness of Direct Vs Indirect Technique Myofascial Release in The Management of Tensiontype Headachekapturzak100% (1)
- Physical Therapy in Sport: Literature ReviewDocument8 pagesPhysical Therapy in Sport: Literature ReviewDaniel GuevaraNo ratings yet
- Clin Psychology and Psychoth - 2017 - Durá Ferrandis - Confirming The Mechanisms Behind Cognitive Behavioural TherapyDocument7 pagesClin Psychology and Psychoth - 2017 - Durá Ferrandis - Confirming The Mechanisms Behind Cognitive Behavioural TherapyNatalie JaraNo ratings yet
- Temporomandibular Joint Dysfunctions: A Systematic Review of Treatment ApproachesDocument13 pagesTemporomandibular Joint Dysfunctions: A Systematic Review of Treatment Approachesnabila puspitaNo ratings yet
- Wright 2000Document9 pagesWright 2000Renan MassarentiNo ratings yet
- Efficacy of Prolotherapy in Temporomandibular Joint Disorders: An Exploratory StudyDocument6 pagesEfficacy of Prolotherapy in Temporomandibular Joint Disorders: An Exploratory StudyAmadea EmanuelaNo ratings yet
- Temporomandibular Disorder and Headache Prevalence - A Systematic Review and Meta-AnalysisDocument18 pagesTemporomandibular Disorder and Headache Prevalence - A Systematic Review and Meta-AnalysisJorge CaserioNo ratings yet
- Mobilisation and ManipulationDocument10 pagesMobilisation and ManipulationAbhijit SharmaNo ratings yet
- Al Badawi2004Document11 pagesAl Badawi2004aladim lamieraNo ratings yet
- 2010 - RCT - Maluf SA - Global Postural Reeducation and Static Stretching Exercises in The Treatment of Myogenic Temporomandibular DisordersDocument8 pages2010 - RCT - Maluf SA - Global Postural Reeducation and Static Stretching Exercises in The Treatment of Myogenic Temporomandibular DisordersAmaia MeiNo ratings yet
- Shockwave Treatment For Denerved MuscleDocument6 pagesShockwave Treatment For Denerved MuscleMauricio PinalNo ratings yet
- 6 Various Treatment Modalities in TMJ Disorders (Autosaved)Document52 pages6 Various Treatment Modalities in TMJ Disorders (Autosaved)Supriya ShuklaNo ratings yet
- Effects of Oral Motor Exercises and Laser Therapy On Chronic Temporomandibular DisordersDocument10 pagesEffects of Oral Motor Exercises and Laser Therapy On Chronic Temporomandibular DisordersLaura Espejo SalamancaNo ratings yet
- Tprelease PDFDocument6 pagesTprelease PDFtvmNo ratings yet
- Buyukturan 2018Document8 pagesBuyukturan 2018Eka BagaskaraNo ratings yet
- 2001 - RCT - Nicolakis, P - Effectiveness of Exercise Therapy in Patients With Internal Derangement of The Temporomandibular JointDocument7 pages2001 - RCT - Nicolakis, P - Effectiveness of Exercise Therapy in Patients With Internal Derangement of The Temporomandibular JointAmaia MeiNo ratings yet
- 1 s2.0 S1746068923000500 MainDocument9 pages1 s2.0 S1746068923000500 MainBruno GonçalvesNo ratings yet
- 00-Effectiveness of Conservative Therapeutic Modalities For Temporomandibular Disorders-Related PDocument13 pages00-Effectiveness of Conservative Therapeutic Modalities For Temporomandibular Disorders-Related PVALESKA FARIÑA ESPINOSANo ratings yet
- Materi PIR - Dr. Lydia Arfianti, SP - KFR-K The Strategies in Rehabilitation of Pathologic Fracture of The SpineDocument30 pagesMateri PIR - Dr. Lydia Arfianti, SP - KFR-K The Strategies in Rehabilitation of Pathologic Fracture of The SpineGhea Putri HendrianiNo ratings yet
- Atm Seminario 4Document9 pagesAtm Seminario 4LAURA MARCELA BARRENECHE CALLENo ratings yet
- Effect of Cyclic Loading On The Temporomandibular Joint: Janith Muhandiram, Bin Wang, Mahmoud ChizariDocument4 pagesEffect of Cyclic Loading On The Temporomandibular Joint: Janith Muhandiram, Bin Wang, Mahmoud ChizariOromax OhmRajaniNo ratings yet
- Ijerph 20 02777Document14 pagesIjerph 20 02777Paola ClaudetNo ratings yet
- Clinical Practice Guideline For Management For Rehabilitation of Lower Limb AmputationDocument55 pagesClinical Practice Guideline For Management For Rehabilitation of Lower Limb Amputationburtyx100% (1)
- Recovery From Temporomandibular Joint Dysfunction: An Overview of Different Physiotherapy ApproachesDocument6 pagesRecovery From Temporomandibular Joint Dysfunction: An Overview of Different Physiotherapy ApproachesSports JournalNo ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- Nat BoardDocument93 pagesNat BoardChintan C. Nishar100% (1)
- Alcohol AbuseDocument2 pagesAlcohol AbuseShanice OrtizNo ratings yet
- Womb As OasisDocument18 pagesWomb As OasisMaria Paula SuarezNo ratings yet
- 1, Nurhamlin, Risdayati Dan IndrawatiDocument15 pages1, Nurhamlin, Risdayati Dan IndrawatiSophia Amelia PutriNo ratings yet
- Purple RiceDocument4 pagesPurple Ricemonica lestaryNo ratings yet
- Chapter30 NecropsyMethodsandProceduresDocument9 pagesChapter30 NecropsyMethodsandProceduresFernanda MenezesNo ratings yet
- Prevalence and Pattern of Menstrual Disorders IJARDocument3 pagesPrevalence and Pattern of Menstrual Disorders IJARWilson ThomasNo ratings yet
- Lac NL - Spring 2021Document8 pagesLac NL - Spring 2021Ghassan NajmNo ratings yet
- 1.2. PTI Insurance Benefits - English VersionDocument23 pages1.2. PTI Insurance Benefits - English VersionĐào Duy PhiNo ratings yet
- Promoting Smart Farming, Eco-Friendly and Innovative Technologies For Sustainable Coconut DevelopmentDocument4 pagesPromoting Smart Farming, Eco-Friendly and Innovative Technologies For Sustainable Coconut DevelopmentMuhammad Maulana Sidik0% (1)
- Tpbo Paper 1Document71 pagesTpbo Paper 1RaghuNo ratings yet
- Elliott 2011Document12 pagesElliott 2011oscar eduardo mateus ariasNo ratings yet
- Cass Review Interim Report Final Web AccessibleDocument112 pagesCass Review Interim Report Final Web AccessibleAvril CastañoNo ratings yet
- Daftar Pustaka AsDocument1 pageDaftar Pustaka AsIchsanQuswainNo ratings yet
- Enraf Nonius Eltrac 471 enDocument3 pagesEnraf Nonius Eltrac 471 enMedicare ExelNo ratings yet
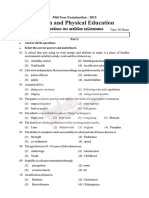
- Eg8 Hea tt2 2015Document3 pagesEg8 Hea tt2 2015enaya de alwisNo ratings yet
- Content: Standard Operating Procedure (SOP) Use and Maintenance of An AutoclaveDocument10 pagesContent: Standard Operating Procedure (SOP) Use and Maintenance of An Autoclaverijulesh karmelNo ratings yet
- Semidirect Vital Tooth Onlay Restoration: A Case ReportDocument5 pagesSemidirect Vital Tooth Onlay Restoration: A Case ReportResa YudhistiNo ratings yet
- Tips and Guidelines For Being A Successful ResearcherDocument11 pagesTips and Guidelines For Being A Successful ResearcherMaria Carmela DomocmatNo ratings yet
- Ebook Benzels Spine Surgery 2 Volume Set Techniques Complication Avoidance and Management PDF Full Chapter PDFDocument67 pagesEbook Benzels Spine Surgery 2 Volume Set Techniques Complication Avoidance and Management PDF Full Chapter PDFgerald.wesolowski623100% (22)
- Medicare Patient Health Risk AssessmentDocument2 pagesMedicare Patient Health Risk AssessmentShobhitNo ratings yet
- Discussion Question No 2Document5 pagesDiscussion Question No 2Vanessa SibayanNo ratings yet
- International Rules For Seed Testing 2022: Introduction To The ISTA RulesDocument14 pagesInternational Rules For Seed Testing 2022: Introduction To The ISTA RulesLolpo KolpoNo ratings yet
- Gaggers and Its ManagementDocument58 pagesGaggers and Its ManagementAwani GuptaNo ratings yet