You might also like
- Community Health Nursing Answer KeyDocument9 pagesCommunity Health Nursing Answer Keyjeshema87% (45)
- MIDTERM Community Nursing 2Document24 pagesMIDTERM Community Nursing 2Will Garcia100% (2)
- CHNC StandardsDocument44 pagesCHNC StandardshamdanaNo ratings yet
- Burmen B, Mutai K: Abstract-Linkage of Newly Diagnosed HIV Positive IndividualsDocument9 pagesBurmen B, Mutai K: Abstract-Linkage of Newly Diagnosed HIV Positive IndividualsJASH MATHEWNo ratings yet
- Sample PresentationDocument36 pagesSample Presentationmuhammed essaNo ratings yet
- CCM Talk Template With Citations Copy1Document58 pagesCCM Talk Template With Citations Copy1Balraj RandhawaNo ratings yet
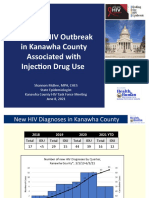
- Update: HIV Outbreak in Kanawha County Associated With Injection Drug UseDocument10 pagesUpdate: HIV Outbreak in Kanawha County Associated With Injection Drug UseJune LefflerNo ratings yet
- 156 - A - Further Information RECIPEDocument6 pages156 - A - Further Information RECIPEKeith userNo ratings yet
- Translate AnakDocument12 pagesTranslate AnakAndikNo ratings yet
- Explorative Study To Assess The Knowledge & Attitude Towards NABH Accreditation Among The Staff Nurses Working in Bombay Hospital, Indore. India.Document2 pagesExplorative Study To Assess The Knowledge & Attitude Towards NABH Accreditation Among The Staff Nurses Working in Bombay Hospital, Indore. India.International Organization of Scientific Research (IOSR)No ratings yet
- POC Testing For HCV at CBOsDocument1 pagePOC Testing For HCV at CBOsRobert G. Gish, MDNo ratings yet
- IDSPDocument56 pagesIDSPitsdheeraj2002No ratings yet
- Week3 PDFDocument37 pagesWeek3 PDFdyah ayu shinta lesmanawatiNo ratings yet
- WHO Consultation On Positive Synergies Between Health Systems and Global Health Initiatives Jim Yong Kim M.D., PH.DDocument22 pagesWHO Consultation On Positive Synergies Between Health Systems and Global Health Initiatives Jim Yong Kim M.D., PH.DLeonel NkwetiNo ratings yet
- Adherence Counseling and Reminder Text Messages Improve Uptake of Antiretroviral Therapy in A Tertiary Hospital in NigeriaDocument7 pagesAdherence Counseling and Reminder Text Messages Improve Uptake of Antiretroviral Therapy in A Tertiary Hospital in NigeriaRiska Resty WasitaNo ratings yet
- Literature Review On Hiv Counselling and TestingDocument4 pagesLiterature Review On Hiv Counselling and Testingwopugemep0h3100% (1)
- Hospital Outcomes For Paediatric Pneumonia and Diarrhoea Patients Admitted in A Tertiary Hospital On Weekdays Versus Weekends: A Retrospective StudyDocument9 pagesHospital Outcomes For Paediatric Pneumonia and Diarrhoea Patients Admitted in A Tertiary Hospital On Weekdays Versus Weekends: A Retrospective StudyZidni Arifa LuthfiNo ratings yet
- Hospital-Based ACT Intervention To Improve Retention in Care For Persons With HIV - 2021Document18 pagesHospital-Based ACT Intervention To Improve Retention in Care For Persons With HIV - 2021Ashik RahamanNo ratings yet
- Pediatrics 2012 Fu E496 503jnnjnjnjDocument10 pagesPediatrics 2012 Fu E496 503jnnjnjnjDyera JessenskyNo ratings yet
- Ahmed Linkage PresentationDocument15 pagesAhmed Linkage PresentationKRUSU ISAACNo ratings yet
- DSD ART Recommendations Module 4 enDocument13 pagesDSD ART Recommendations Module 4 enAbay BiruNo ratings yet
- Does A Clinical Guideline Change Chlamydia Testing?Document7 pagesDoes A Clinical Guideline Change Chlamydia Testing?gt_shadowNo ratings yet
- Understanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiDocument34 pagesUnderstanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- Cyprien Nioble, Jhpiego-Cote Divoire, IAS2012 Poster, MNH Quality ImprovementDocument1 pageCyprien Nioble, Jhpiego-Cote Divoire, IAS2012 Poster, MNH Quality ImprovementJhpiegoNo ratings yet
- Darren L. Mungcal BSN 123 Group 92 Evidence Based NursingDocument6 pagesDarren L. Mungcal BSN 123 Group 92 Evidence Based NursingRowena MungcalNo ratings yet
- Occurrence and Outcome of Delirium in Medical In-Patients: A Systematic Literature ReviewDocument15 pagesOccurrence and Outcome of Delirium in Medical In-Patients: A Systematic Literature ReviewJoao CabralNo ratings yet
- Vestine PPT Work DefenseDocument17 pagesVestine PPT Work Defenseshyaka jean claudeNo ratings yet
- RCH - Reproductive and Child Health Part 2Document32 pagesRCH - Reproductive and Child Health Part 2Dr. Rakshit SolankiNo ratings yet
- Key Steps To Improve and Measure Clinical Outcomes RyanDocument25 pagesKey Steps To Improve and Measure Clinical Outcomes RyansaphyqNo ratings yet
- SOP - HIV Care Patient Follow-Up ProgrammeDocument23 pagesSOP - HIV Care Patient Follow-Up ProgrammeParwatiNo ratings yet
- Comprehensive Discharge Planning-Ebp PowerpointDocument45 pagesComprehensive Discharge Planning-Ebp Powerpointapi-24187790No ratings yet
- Kozar MiniposterDocument1 pageKozar Miniposterapi-277743817No ratings yet
- Kumpulan Jurnal InternasionalDocument15 pagesKumpulan Jurnal InternasionalTIKANo ratings yet
- Family Testing Day CDC - Index - Case - BriefDocument4 pagesFamily Testing Day CDC - Index - Case - BriefNephtalie MESIDORNo ratings yet
- 5.pradeep MK Nair Et Al.Document5 pages5.pradeep MK Nair Et Al.International Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Colorectal Cancer Screening and Quality MeasuresDocument10 pagesColorectal Cancer Screening and Quality MeasuresmnovemberNo ratings yet
- Improving Human Resources Capacity Through Evidence-Based TrainingDocument14 pagesImproving Human Resources Capacity Through Evidence-Based TrainingIDCAP2011No ratings yet
- Hiv Fix 2Document7 pagesHiv Fix 2Wulan CerankNo ratings yet
- Nurses' Knowledge On Nosocomial Infections Preventive Measures and Its Associated Factors in Ghana A Cross-Sectional Study BMDocument1 pageNurses' Knowledge On Nosocomial Infections Preventive Measures and Its Associated Factors in Ghana A Cross-Sectional Study BMahilhamza55No ratings yet
- By Danish LatifDocument43 pagesBy Danish LatifShimmering MoonNo ratings yet
- CareMore: Innovative Healthcare DeliveryDocument30 pagesCareMore: Innovative Healthcare DeliveryPartnership to Fight Chronic DiseaseNo ratings yet
- National Aids Control ProgDocument45 pagesNational Aids Control ProgGirishkumar KrishnaNo ratings yet
- Approaches To Self Management ResearchDocument50 pagesApproaches To Self Management ResearchFakir TajulNo ratings yet
- Underserved Does Not Mean Undeserved: Unfurling The HCV Care in The Safety NetDocument3 pagesUnderserved Does Not Mean Undeserved: Unfurling The HCV Care in The Safety NetmotorpenggerakNo ratings yet
- Development and Validation of PACICDocument9 pagesDevelopment and Validation of PACICKristen LynchNo ratings yet
- Data SaturationDocument8 pagesData SaturationmakmgmNo ratings yet
- Medical Home: Care Coordination: The Patient-CenteredDocument23 pagesMedical Home: Care Coordination: The Patient-CenteredDwi Suranto100% (1)
- Quality of Care: Eze Chukwu NwoyeDocument22 pagesQuality of Care: Eze Chukwu Nwoyeeze NwoyeNo ratings yet
- Women's Perception of Antenatal Care Services in Public and Private Clinics in The GambiaDocument6 pagesWomen's Perception of Antenatal Care Services in Public and Private Clinics in The GambiaakindunnidanielNo ratings yet
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- Journal ClubDocument18 pagesJournal Clubapi-532604536No ratings yet
- 281 FullDocument9 pages281 FullReRe DomilaNo ratings yet
- Pfe101 508Document85 pagesPfe101 508Basma AzazNo ratings yet
- Pharmacy 07 00083Document18 pagesPharmacy 07 00083alfinadyaNo ratings yet
- Das (2018) Universal Delivery of HealthcareDocument5 pagesDas (2018) Universal Delivery of HealthcareWaqasRabbaniNo ratings yet
- Health-Care Reform in Georgia: Irakli TortladzeDocument26 pagesHealth-Care Reform in Georgia: Irakli TortladzeShubham TanwarNo ratings yet
- Leveraging QI To Integrate FP Services Into Postpartum Care in AfghanistanDocument13 pagesLeveraging QI To Integrate FP Services Into Postpartum Care in AfghanistanMaternal and Child Survival Program (MCSP)No ratings yet
- Pour Marzi 2019Document10 pagesPour Marzi 2019Ayu Try WahyuningsihNo ratings yet
- Surveillance: Abdullatif Husseini, MSC, MPH, PHDDocument37 pagesSurveillance: Abdullatif Husseini, MSC, MPH, PHDMayson BaliNo ratings yet
- Demographic Health Health SurveysDocument18 pagesDemographic Health Health SurveysERUSTUS WESANo ratings yet
- A Group Visit Initiative Improves Advance Care Planning Documentation Among Older Adults in Primary CareDocument11 pagesA Group Visit Initiative Improves Advance Care Planning Documentation Among Older Adults in Primary CareAri AzhariNo ratings yet
- Factors Associated With First-Line Antiretroviral Therapy Failure Amongst HIV-Infected African Patients: A Case-Control StudyDocument8 pagesFactors Associated With First-Line Antiretroviral Therapy Failure Amongst HIV-Infected African Patients: A Case-Control Studymeriza dahlia putriNo ratings yet
- Differentiated Service Delivery-Advanced HIV Disease (DSD) : June/ 2023Document48 pagesDifferentiated Service Delivery-Advanced HIV Disease (DSD) : June/ 2023በተግባር ግዛቸውNo ratings yet
- Community Health NursingDocument9 pagesCommunity Health Nursingaiki parkNo ratings yet
- Qualities of Community Health NurseDocument20 pagesQualities of Community Health NurseNeethu Vincent80% (5)
- Nursing Job MotivationDocument10 pagesNursing Job MotivationJosephine FloresNo ratings yet
- Introduction To CHNDocument23 pagesIntroduction To CHNmohammed RAFI100% (1)
- UntitledDocument6 pagesUntitledAnna YepisNo ratings yet
- Home VisitDocument15 pagesHome VisitRosa Villanueva CarrascoNo ratings yet
- 5165 Scaling Up Primary Health Care in The Philippines Lessons From A Systematic Review of Experiences of Community Based Health ProgramsDocument9 pages5165 Scaling Up Primary Health Care in The Philippines Lessons From A Systematic Review of Experiences of Community Based Health ProgramsHanako Sasaki AranillaNo ratings yet
- Concepts in Community Health Nursing - A Family StudyDocument75 pagesConcepts in Community Health Nursing - A Family Studytina_abelloNo ratings yet
- Handouts CHNDocument23 pagesHandouts CHNJames Eugene CaasiNo ratings yet
- Research Proposal Template SampleDocument26 pagesResearch Proposal Template SampleFrace RojoNo ratings yet
- CHN Post Test MT2Document16 pagesCHN Post Test MT2Rika MaeNo ratings yet
- Unit 2Document17 pagesUnit 2Shini SimonNo ratings yet
- 4th Quarter #3 Health Career PathwaysDocument19 pages4th Quarter #3 Health Career PathwaysJEANY BARROZONo ratings yet
- Community Assessment Paper Pasco County - Omar Shaout 2Document8 pagesCommunity Assessment Paper Pasco County - Omar Shaout 2api-679742031No ratings yet
- Unit 1: Community Health NursingDocument56 pagesUnit 1: Community Health NursingNishaAhsinNo ratings yet
- Community Health Nursing - Case PresentationDocument45 pagesCommunity Health Nursing - Case PresentationLev Jasper Alcantara Blanco100% (8)
- NRSG 100 Introduction To NursingDocument104 pagesNRSG 100 Introduction To Nursingchet_sisal7573No ratings yet
- Learning Guide PHC 2Document20 pagesLearning Guide PHC 2Niña Amato100% (1)
- Q4-PPT-Health10 - Lesson 2 (Health Career Pathways)Document34 pagesQ4-PPT-Health10 - Lesson 2 (Health Career Pathways)oliver cusipagNo ratings yet
- Body of Standing For Cho 1 - 9!9!2015Document394 pagesBody of Standing For Cho 1 - 9!9!2015Abidemi EreolaNo ratings yet
- Grade 9 Mapeh HealthDocument5 pagesGrade 9 Mapeh HealthMae Ann PiorqueNo ratings yet
- Study Guide CP PHC IDocument4 pagesStudy Guide CP PHC IChristopher BañezNo ratings yet
- NCM 113 (CHN 2) Lec - Prelim-Part 1Document52 pagesNCM 113 (CHN 2) Lec - Prelim-Part 1rubycubionaNo ratings yet
- CHN 2Document3 pagesCHN 2Patrick Ray TanNo ratings yet
- Unit 1 Introduction To Community Health NursingDocument5 pagesUnit 1 Introduction To Community Health NursingIvyNo ratings yet
- Mobile Health Clinic InitiativeDocument47 pagesMobile Health Clinic InitiativededdyNo ratings yet
- CPH Chap-01Document54 pagesCPH Chap-01SARAH DE LUNANo ratings yet