You might also like
- Endocrine - BoardsDocument9 pagesEndocrine - BoardsSoojung Nam100% (4)
- Ultrasound of Thyroid, Parathyroid Glands and Neck Lymph NodesDocument64 pagesUltrasound of Thyroid, Parathyroid Glands and Neck Lymph Nodesnaga999100% (2)
- EndocrinologyDocument46 pagesEndocrinology[161]Shuaib AktherNo ratings yet
- Adrenal Gland DisordersDocument7 pagesAdrenal Gland Disorderscn351073No ratings yet
- Congenital HypothyroidismDocument44 pagesCongenital Hypothyroidismnayabrizvi1No ratings yet
- Hypo Thyroids MDocument26 pagesHypo Thyroids MBridget NjambiNo ratings yet
- The Role of Hormones in The Female and MALE REPRODUCTIVE SYSTEMDocument10 pagesThe Role of Hormones in The Female and MALE REPRODUCTIVE SYSTEMBryan Bries100% (3)
- Hashimoto ThyroiditisDocument19 pagesHashimoto ThyroiditisPaulina Maria PaciejNo ratings yet
- HypothyroidismDocument49 pagesHypothyroidismBahaa ShaabanNo ratings yet
- Name: Mohammad Farez Sayfoo Student Number: 310300440Document21 pagesName: Mohammad Farez Sayfoo Student Number: 310300440mohammadsayfooNo ratings yet
- Cushing's DiseaseDocument1 pageCushing's DiseaseAdeline N. OmeneNo ratings yet
- Iugr FinalDocument35 pagesIugr Finalsanthiyasandy100% (4)
- Thyroid Disorders During PregnancyDocument25 pagesThyroid Disorders During PregnancyA.H.ANo ratings yet
- Congenital HypothyroidismDocument21 pagesCongenital HypothyroidismDanna GarcíaNo ratings yet
- Thyroid DisordersDocument55 pagesThyroid DisordersNsubuga Ivan100% (1)
- IUGRDocument22 pagesIUGRSairindri SahooNo ratings yet
- Midterms-NCM-109-Pedia-Lec-Dean (Repaired)Document28 pagesMidterms-NCM-109-Pedia-Lec-Dean (Repaired)Drannel FajardoNo ratings yet
- A CASE REPORT: Hyperthyroidism in PregnancyDocument46 pagesA CASE REPORT: Hyperthyroidism in PregnancyIrma Permata sariNo ratings yet
- Congenital HypothyroidismDocument50 pagesCongenital HypothyroidismG VenkateshNo ratings yet
- Pediatric Endocrinology Review MCQsDocument104 pagesPediatric Endocrinology Review MCQsTirou100% (1)
- Congenital Hypothyroidism (CH)Document44 pagesCongenital Hypothyroidism (CH)Rachel SepthyNo ratings yet
- Newborn ScreeningDocument6 pagesNewborn ScreeningJeralyn GabagatNo ratings yet
- FINALS AutoImmune Disorders and Nueromuscular Disorders 1Document101 pagesFINALS AutoImmune Disorders and Nueromuscular Disorders 1Lindley Pamela OlazoNo ratings yet
- Congenital Hypothyroidism2Document4 pagesCongenital Hypothyroidism2sectioNo ratings yet
- DR - Rihab Pediatrics 04.hypothyroidismDocument7 pagesDR - Rihab Pediatrics 04.hypothyroidismMujtaba JawadNo ratings yet
- Hypothyroidism: By: Judhaimah Mardhiah BT Mat Tari 0810544Document23 pagesHypothyroidism: By: Judhaimah Mardhiah BT Mat Tari 0810544Jujue MardhiahNo ratings yet
- The Child With Endocrine/Metabolic Dysfunction: Thyroid Gland DisordersDocument17 pagesThe Child With Endocrine/Metabolic Dysfunction: Thyroid Gland DisordersMeccanazaren Susvilla BojorqueNo ratings yet
- Congenital Hypothyroidism: Vijivs Lecturer Kims College of NursingDocument21 pagesCongenital Hypothyroidism: Vijivs Lecturer Kims College of NursingVijiNo ratings yet
- Эндокринологическая патология и беременность 2018Document50 pagesЭндокринологическая патология и беременность 2018Med PoxNo ratings yet
- Endo FinalsDocument10 pagesEndo FinalsMary Reigns BuhatNo ratings yet
- Guidelines For Management of Congenital Hypothyroidism1Document8 pagesGuidelines For Management of Congenital Hypothyroidism1Firdaus AzinunNo ratings yet
- The Child With An Endocrine or Metabolic Alteration: University of Maryland School of NursingDocument54 pagesThe Child With An Endocrine or Metabolic Alteration: University of Maryland School of NursingGelsey Gelsinator JianNo ratings yet
- Update of Newborn Screening and Therapy For Congenital HypothyroidismDocument14 pagesUpdate of Newborn Screening and Therapy For Congenital HypothyroidismMauricio HurtadoNo ratings yet
- Pediatrics Endocrine DisordersDocument33 pagesPediatrics Endocrine DisordersfatimaNo ratings yet
- Precocious Puberty With Primary Hypothyroidism Due To Autoimmune ThyroiditisDocument3 pagesPrecocious Puberty With Primary Hypothyroidism Due To Autoimmune ThyroiditisShohel RanaNo ratings yet
- CONGENITAL HYPOTHYROIDISM Lec 5th Year 1Document17 pagesCONGENITAL HYPOTHYROIDISM Lec 5th Year 1Alokh Saha RajNo ratings yet
- Thyroid and NewbornDocument5 pagesThyroid and NewbornxanderaleNo ratings yet
- CRETENISMDocument2 pagesCRETENISMPhilip Gene II MalacasNo ratings yet
- Newborn Screening: Diseases That Can Be Assessed in Newborn ScreeningDocument5 pagesNewborn Screening: Diseases That Can Be Assessed in Newborn ScreeningJHONESSA LAYOSNo ratings yet
- ThyroidDocument16 pagesThyroidnawaNo ratings yet
- Etiology: Ongenital Hypothyroidism (CH) Is A Condition ofDocument4 pagesEtiology: Ongenital Hypothyroidism (CH) Is A Condition ofgheyahNo ratings yet
- Obg PPT 1Document27 pagesObg PPT 1yash myatraNo ratings yet
- Common EndocrinopathiesDocument50 pagesCommon EndocrinopathiesHamza AliNo ratings yet
- Hipotiroidism Diaz 2014Document17 pagesHipotiroidism Diaz 2014Achmad ArrizalNo ratings yet
- Congenital HypothyroidismDocument43 pagesCongenital HypothyroidismJolmajas JoharNo ratings yet
- Congenital HypothyroidismDocument36 pagesCongenital HypothyroidismRandi DwiyantoNo ratings yet
- Hippo EM Foundations - Pediatric Emergencies Written SummaryDocument31 pagesHippo EM Foundations - Pediatric Emergencies Written Summarykaylawilliam01No ratings yet
- English3 With DR - EllenDocument10 pagesEnglish3 With DR - EllenRandi DwiyantoNo ratings yet
- Congenital Hypothyroidism: Titis Prawitasari Dept. Ilmu Kesehatan Anak Fkui-RscmDocument25 pagesCongenital Hypothyroidism: Titis Prawitasari Dept. Ilmu Kesehatan Anak Fkui-RscmAC ACNo ratings yet
- Congenital Hypothyroidism: Practice EssentialsDocument15 pagesCongenital Hypothyroidism: Practice EssentialsTonang Dwi ArdyantoNo ratings yet
- Common Newborn Problems (2) C1Document39 pagesCommon Newborn Problems (2) C1ZmNo ratings yet
- Approach To Delay PubertyDocument33 pagesApproach To Delay PubertyRaja Iqbal Mulya HarahapNo ratings yet
- Thyroid DiseaseDocument30 pagesThyroid Diseasemy Lord JesusNo ratings yet
- Case Presentation Ob MaternityDocument44 pagesCase Presentation Ob MaternityRodean Andrew NonatoNo ratings yet
- Pemicu 3: Siklus Hidup 2014Document54 pagesPemicu 3: Siklus Hidup 2014exxxxooooNo ratings yet
- Hypo ToniaDocument56 pagesHypo ToniaKRITHIKA A/P PALANNY MoeNo ratings yet
- Amenorrhea: DR - Raveendra MVDocument23 pagesAmenorrhea: DR - Raveendra MVRaveendra M.vNo ratings yet
- Sample Case: EndocrinologyDocument42 pagesSample Case: EndocrinologyCoy NuñezNo ratings yet
- NCM 109 High Risk PregnancyDocument11 pagesNCM 109 High Risk PregnancyLea BorceNo ratings yet
- DR - Nazar 1Document15 pagesDR - Nazar 1Rm98No ratings yet
- Sexual Precocity PDFDocument5 pagesSexual Precocity PDFmist73No ratings yet
- Etiology: Congenital Hypothyroidism (CH) Is A Condition of Thyroid Hormone Deficiency Present at BirthDocument3 pagesEtiology: Congenital Hypothyroidism (CH) Is A Condition of Thyroid Hormone Deficiency Present at BirthRandi DwiyantoNo ratings yet
- Thyroid Disorders in ChildrenDocument30 pagesThyroid Disorders in ChildrenZm100% (1)
- Kuliah ThyroidDocument36 pagesKuliah ThyroidMita Erna WatiNo ratings yet
- Dr.Russell Pediatrics 01.Child Developmental Milestones (2)Document6 pagesDr.Russell Pediatrics 01.Child Developmental Milestones (2)Mujtaba JawadNo ratings yet
- Dr.Russell Pediatrics 01.Child Developmental Milestones (2)Document6 pagesDr.Russell Pediatrics 01.Child Developmental Milestones (2)Mujtaba JawadNo ratings yet
- E-Dr.Russell Pediatrics 04.Cerebral Palsy & AtaxiasDocument5 pagesE-Dr.Russell Pediatrics 04.Cerebral Palsy & AtaxiasMujtaba JawadNo ratings yet
- E-Dr.Russell Pediatrics 05.CNS InfectionDocument13 pagesE-Dr.Russell Pediatrics 05.CNS InfectionMujtaba JawadNo ratings yet
- E-Dr.russell Pediatrics 03.Seizure Part TwoDocument7 pagesE-Dr.russell Pediatrics 03.Seizure Part TwoMujtaba JawadNo ratings yet
- Dr.Russell Pediatrics 02.Seizure Part OneDocument10 pagesDr.Russell Pediatrics 02.Seizure Part OneMujtaba JawadNo ratings yet
- E-Dr.Russell Pediatrics 04.Cerebral Palsy & AtaxiasDocument5 pagesE-Dr.Russell Pediatrics 04.Cerebral Palsy & AtaxiasMujtaba JawadNo ratings yet
- E-Dr.Russell Pediatrics 05.CNS InfectionDocument13 pagesE-Dr.Russell Pediatrics 05.CNS InfectionMujtaba JawadNo ratings yet
- E-Dr.Russell Pediatrics 04.Cerebral Palsy & AtaxiasDocument5 pagesE-Dr.Russell Pediatrics 04.Cerebral Palsy & AtaxiasMujtaba JawadNo ratings yet
- Dr.Russell Pediatrics 01.Child Developmental Milestones (2)Document6 pagesDr.Russell Pediatrics 01.Child Developmental Milestones (2)Mujtaba JawadNo ratings yet
- E-Dr.russell Pediatrics 03.Seizure Part TwoDocument7 pagesE-Dr.russell Pediatrics 03.Seizure Part TwoMujtaba JawadNo ratings yet
- Dr.Russell Pediatrics 02.Seizure Part OneDocument10 pagesDr.Russell Pediatrics 02.Seizure Part OneMujtaba JawadNo ratings yet
- DR - Rihab Pediatrics 03.short SatureDocument7 pagesDR - Rihab Pediatrics 03.short SatureMujtaba JawadNo ratings yet
- Human Physiology Chapter 4 - EndDocument172 pagesHuman Physiology Chapter 4 - EndEmebet DebissaNo ratings yet
- ENDOCRINE SystemDocument54 pagesENDOCRINE SystemSJO1 G6- Escaro,Shaira JoyNo ratings yet
- Pex 09 06Document5 pagesPex 09 06Maulvi Alfarras YamriNo ratings yet
- Guias Thyroid 2012Document43 pagesGuias Thyroid 2012JoseAbdalaNo ratings yet
- Benign Diseases of ThyroidDocument70 pagesBenign Diseases of ThyroidMounica MekalaNo ratings yet
- Acromegaly & GigantismDocument20 pagesAcromegaly & GigantismTuhinaRajNo ratings yet
- Steroid AbuseDocument7 pagesSteroid Abuseapi-400575655No ratings yet
- Adrenals - Central Metabolic Control SystemTherapy PDFDocument2 pagesAdrenals - Central Metabolic Control SystemTherapy PDFNanuNo ratings yet
- Cc2 l5 EndocrinologyDocument4 pagesCc2 l5 EndocrinologyRose Denisse EstrellaNo ratings yet
- DisfungsiDocument1 pageDisfungsiHandayan HtbNo ratings yet
- Progesterone and Estrogen Thyroid GlandDocument3 pagesProgesterone and Estrogen Thyroid GlandReymark VillanuevaNo ratings yet
- Thyroid Function Test Results: APFCB Masterclass in Interpretative CommentingDocument58 pagesThyroid Function Test Results: APFCB Masterclass in Interpretative CommentingGPNNo ratings yet
- PT No. 2 3rd Quarter Endocrine SystemDocument2 pagesPT No. 2 3rd Quarter Endocrine SystemDarknessNo ratings yet
- Emergencias Tiroideas 2019Document17 pagesEmergencias Tiroideas 2019Marlon UlloaNo ratings yet
- H H H H H M M M M M: Ormone Ormone Ormone Ormone Ormone ET ET ET ET Etabolism Abolism Abolism Abolism AbolismDocument28 pagesH H H H H M M M M M: Ormone Ormone Ormone Ormone Ormone ET ET ET ET Etabolism Abolism Abolism Abolism AbolismHoth HothNo ratings yet
- Integumentary SystemDocument6 pagesIntegumentary SystemJohn Denver BechaydaNo ratings yet
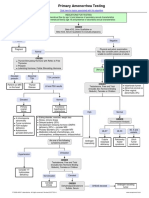
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Case Study On Toxic GoiterDocument5 pagesCase Study On Toxic GoiterRein EstradaNo ratings yet
- Hipertiroidismo en GatosDocument20 pagesHipertiroidismo en GatosBrenda GómezNo ratings yet
- The Endocrine Glands and The Nervous SystemDocument5 pagesThe Endocrine Glands and The Nervous SystemLyanna MormontNo ratings yet
- 3.histology of Skin AppendagesDocument43 pages3.histology of Skin AppendagesdenekeNo ratings yet
- Biology PancreasDocument10 pagesBiology Pancreasjavier orellana mejiaNo ratings yet
- ThyroidDocument43 pagesThyroidchowhan04No ratings yet
- Reproductive Processes: Chapter-34-Lesson-2 Page-961-966Document26 pagesReproductive Processes: Chapter-34-Lesson-2 Page-961-966JanaNo ratings yet
- HypothalamusDocument5 pagesHypothalamusBoneGrissleNo ratings yet