You might also like
- Khodayari, 2011Document5 pagesKhodayari, 2011KharismaNisaNo ratings yet
- Calcifying Odontogenic Cyst With Atypica PDFDocument5 pagesCalcifying Odontogenic Cyst With Atypica PDFHerminaElenaNo ratings yet
- Management of Infected Radicular Cyst by Marsupialization: Case ReportDocument5 pagesManagement of Infected Radicular Cyst by Marsupialization: Case Reportvivi hutabaratNo ratings yet
- Semen ToDocument4 pagesSemen ToyesikaichaaNo ratings yet
- Ams 5 108Document4 pagesAms 5 108Alice EmailsNo ratings yet
- Articulo ProtodonciaDocument5 pagesArticulo ProtodonciaMilton David Rios SerratoNo ratings yet
- Journal of Orthopaedic Science: Chin-Kai Huang, Chih-Kai Hong, Fa-Chuan Kuan, Wei-Ren Su, Kai-Lan HsuDocument4 pagesJournal of Orthopaedic Science: Chin-Kai Huang, Chih-Kai Hong, Fa-Chuan Kuan, Wei-Ren Su, Kai-Lan Hsuanasofia.vargas22No ratings yet
- The Influence of Cortical Bone Perforation On Guided Bone Regeneration in HumansDocument6 pagesThe Influence of Cortical Bone Perforation On Guided Bone Regeneration in Humanspin.to.teethNo ratings yet
- Osteomielitis PatelarDocument3 pagesOsteomielitis PatelarAlexander DanielNo ratings yet
- Jurnal Utama ProstoDocument5 pagesJurnal Utama ProstoParlin BrutuNo ratings yet
- Ramus Onlay Bone Graft For Maxillary Alveolar Ridge Augmentation-A Case ReportDocument9 pagesRamus Onlay Bone Graft For Maxillary Alveolar Ridge Augmentation-A Case ReportIJAR JOURNALNo ratings yet
- 2005 Laster Width Distraction OsteogenesisDocument7 pages2005 Laster Width Distraction Osteogenesislisal1saNo ratings yet
- E Ect FF of Intra-Articular Injection of Mesenchymal Stem Cells in Cartilage Repair in Experimental AnimalsDocument9 pagesE Ect FF of Intra-Articular Injection of Mesenchymal Stem Cells in Cartilage Repair in Experimental AnimalsPKNo ratings yet
- Articulo en Inglés 2Document8 pagesArticulo en Inglés 2Luis Ramirez BenaventeNo ratings yet
- Aneurysmal Bone Cyst of The Mandible: Case Presentation and Review of The LiteratureDocument3 pagesAneurysmal Bone Cyst of The Mandible: Case Presentation and Review of The LiteratureCarolina RomeroNo ratings yet
- Resumen Ingles Proyección 2Document5 pagesResumen Ingles Proyección 2valentinaNo ratings yet
- Controversiesin Traditionaloraland MaxillofacialreconstructionDocument13 pagesControversiesin Traditionaloraland MaxillofacialreconstructionSheetal HNo ratings yet
- Buccal-Lingual Bone Remodeling in Immediately Loaded Fresh Socket Implants A Cone Beam Computed Tomography StudyDocument8 pagesBuccal-Lingual Bone Remodeling in Immediately Loaded Fresh Socket Implants A Cone Beam Computed Tomography StudyYuki MuraNo ratings yet
- Osteoblastoma of The JawsDocument3 pagesOsteoblastoma of The JawsAngelia PratiwiNo ratings yet
- Contour Determination For Ovate Pontics: Tim J. Dylina, DDSDocument7 pagesContour Determination For Ovate Pontics: Tim J. Dylina, DDSShabbir HasanNo ratings yet
- Journal of Cranio-Maxillo-Facial Surgery: Yehuda Zadik, Alper Aktas, Scott Drucker, Dorrit W. NitzanDocument6 pagesJournal of Cranio-Maxillo-Facial Surgery: Yehuda Zadik, Alper Aktas, Scott Drucker, Dorrit W. Nitzan刘雨樵No ratings yet
- A R A A C L S B C I C B G: Lveolar Idge Ugmentation: Omparative Ongitudinal Tudy Etween Alvaria and Liac Rest ONE RaftsDocument7 pagesA R A A C L S B C I C B G: Lveolar Idge Ugmentation: Omparative Ongitudinal Tudy Etween Alvaria and Liac Rest ONE RaftsDr. Jalisson VicenteNo ratings yet
- Mandible by Injection of Autogeneic BloodDocument4 pagesMandible by Injection of Autogeneic BloodRodolpho VilelaNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars.Document11 pagesA Long-Term Study of 370 Autotransplanted Premolars.jing.zhao222No ratings yet
- Reconstrução de Severa Reabsorção Maxilar Com Distração OsteogenicaDocument7 pagesReconstrução de Severa Reabsorção Maxilar Com Distração OsteogenicaNelson UzunNo ratings yet
- 2010 Miniscrew Assisted Nonsurgical PalatalDocument10 pages2010 Miniscrew Assisted Nonsurgical PalatalMariana SantosNo ratings yet
- Schwarz, Richard - Medial Plantar ArteryDocument5 pagesSchwarz, Richard - Medial Plantar ArteryGrant DotulongNo ratings yet
- Unilateral Mandibular Swelling in A Young Female Patient A Case ReportDocument4 pagesUnilateral Mandibular Swelling in A Young Female Patient A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Tranmucosal FixationDocument4 pagesTranmucosal Fixationlippincott2011No ratings yet
- Anehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesDocument7 pagesAnehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesHenry Adhy SantosoNo ratings yet
- Jurnal 22 PDFDocument4 pagesJurnal 22 PDFsriwahyuutamiNo ratings yet
- The Effect of Complete Dentures On Alveolar MucosaDocument8 pagesThe Effect of Complete Dentures On Alveolar MucosaZachary DuongNo ratings yet
- Bilateral Maxillary Buccal Bone Exostosis: Rare Case ReportDocument4 pagesBilateral Maxillary Buccal Bone Exostosis: Rare Case Reportegi007No ratings yet
- Mandibular Reconstruction With Free Fibula Flap For Medication-Related Osteonecrosis of The Jaw in Patients With Multiple MyelomaDocument4 pagesMandibular Reconstruction With Free Fibula Flap For Medication-Related Osteonecrosis of The Jaw in Patients With Multiple MyelomaRicky Aris FandikaNo ratings yet
- 20 DR Arvind UDDocument7 pages20 DR Arvind UDJohn SmithNo ratings yet
- Fotos OclusalesDocument6 pagesFotos OclusalesMarco Antonio García LunaNo ratings yet
- JBSTDocument4 pagesJBSTmjlovesNo ratings yet
- Osteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingDocument5 pagesOsteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingAnonymous Qt31LLO1lNo ratings yet
- Australian Dental Journal - 2018 - Spencer - Implant Based Rehabilitation Options For The Atrophic Edentulous JawDocument8 pagesAustralian Dental Journal - 2018 - Spencer - Implant Based Rehabilitation Options For The Atrophic Edentulous JawAswathi RaghuthamanNo ratings yet
- Artículo 1 - OstectomíaDocument10 pagesArtículo 1 - OstectomíaEmilio RodríguezNo ratings yet
- Journal of Surgical Oncology - 2023 - Cevolani - Aneurysmal Bone Cyst Is Selective Arterial Embolization Effective AsDocument9 pagesJournal of Surgical Oncology - 2023 - Cevolani - Aneurysmal Bone Cyst Is Selective Arterial Embolization Effective AsReyes Ivan García CuevasNo ratings yet
- Artigo MedeirosDocument6 pagesArtigo MedeirosEugénio MartinsNo ratings yet
- Recurrent Peripheral Odontogenic Keratocyst: A Case ReportDocument3 pagesRecurrent Peripheral Odontogenic Keratocyst: A Case ReportthedocperuNo ratings yet
- 13b Collagen 1Document7 pages13b Collagen 1María Fernanda EstévezNo ratings yet
- 98 IJPRD BioOssDocument12 pages98 IJPRD BioOssinamboy7No ratings yet
- Mandibular Reconstruction With Tissue EngineeringDocument5 pagesMandibular Reconstruction With Tissue EngineeringtamisatnamNo ratings yet
- Ab 2019Document7 pagesAb 2019Dome CárdenasNo ratings yet
- Rehabilitation of Severely Resorbed Edentulous Mandible Using The Modified Visor Osteotomy TechniqueDocument5 pagesRehabilitation of Severely Resorbed Edentulous Mandible Using The Modified Visor Osteotomy TechniqueSaurabh SatheNo ratings yet
- 9230 Case ReportDocument3 pages9230 Case ReportrajaniNo ratings yet
- Tissueengineeringfor Verticalridge Reconstruction: Neel Patel,, Beomjune Kim,, Waleed Zaid,, Daniel SpagnoliDocument23 pagesTissueengineeringfor Verticalridge Reconstruction: Neel Patel,, Beomjune Kim,, Waleed Zaid,, Daniel SpagnoliAB MISHRANo ratings yet
- Reconstruction of Mandible by Free Fibular Flap: Original ArticleDocument5 pagesReconstruction of Mandible by Free Fibular Flap: Original ArticleSani Solihatul FitriNo ratings yet
- Schlund 2019Document3 pagesSchlund 2019mesescuNo ratings yet
- Osteoblastoma A Spectrum of Presentation and TreatDocument10 pagesOsteoblastoma A Spectrum of Presentation and TreatmandetoperdiyuwanNo ratings yet
- Immediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportDocument6 pagesImmediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportBagis Emre GulNo ratings yet
- Case Report Odontogenic KeratocystDocument3 pagesCase Report Odontogenic KeratocystIsty SakulNo ratings yet
- Fsurg 08 662720Document6 pagesFsurg 08 662720Deborah SalinasNo ratings yet
- Bonegraftingforimplant Surgery: Ladi Doonquah,, Pierre-John Holmes,, Laxman Kumar Ranganathan,, Hughette RobertsonDocument19 pagesBonegraftingforimplant Surgery: Ladi Doonquah,, Pierre-John Holmes,, Laxman Kumar Ranganathan,, Hughette RobertsonJason LeeNo ratings yet
- Early Recurrence of Mandibular Torus Following SurDocument4 pagesEarly Recurrence of Mandibular Torus Following SurPaola GillNo ratings yet
- Bradley M. Lamm 2019Document5 pagesBradley M. Lamm 2019DziaulMuizAl'ArifNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument23 pagesAcyanotic Congenital Heart DiseasePernel Jose Alam MicuboNo ratings yet
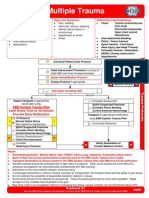
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 pageMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNo ratings yet
- JOURNAL CLUB Presentation: Presented by Phatcharaporn Dangtongdee 583150152-4 Section 3Document21 pagesJOURNAL CLUB Presentation: Presented by Phatcharaporn Dangtongdee 583150152-4 Section 3Phatcharaporn DangtongdeeNo ratings yet
- Irish Dela Cruz Saludares: Summary QualificationsDocument3 pagesIrish Dela Cruz Saludares: Summary QualificationsLudwig Santos-Mindo De Varona-LptNo ratings yet
- Practical PPT TDV Mod 2Document27 pagesPractical PPT TDV Mod 2Teja DvNo ratings yet
- Branch Retinal Vein OcclusionDocument8 pagesBranch Retinal Vein OcclusionTasya BhatoNo ratings yet
- Mallet Finger Advice: Emergency DepartmentDocument8 pagesMallet Finger Advice: Emergency DepartmentTJPlayzNo ratings yet
- Alzheimer's Disease (Mini Presentation)Document51 pagesAlzheimer's Disease (Mini Presentation)Tiger KneeNo ratings yet
- Helicobacter Pylori EradicationDocument190 pagesHelicobacter Pylori EradicationMaca Vera RiveroNo ratings yet
- Apical: Elixir Terpin HydrateDocument3 pagesApical: Elixir Terpin Hydrateailene agustinNo ratings yet
- Fascial FractureDocument6 pagesFascial FractureAmeena RamzanNo ratings yet
- Adverse Events Associated With Melatonin For The Treatment of Primary or Secondary Sleep Disorders: A Systematic ReviewDocument20 pagesAdverse Events Associated With Melatonin For The Treatment of Primary or Secondary Sleep Disorders: A Systematic ReviewZach Segmuel MiñanoNo ratings yet
- VascularDocument40 pagesVascularOmar MohammedNo ratings yet
- NursingCareAfterKidneyTransplantCaseReport PDFDocument7 pagesNursingCareAfterKidneyTransplantCaseReport PDFJohn Louie SolitarioNo ratings yet
- Surgery of The Adrenal GlandsDocument24 pagesSurgery of The Adrenal GlandsRafal SmolinskiNo ratings yet
- Fungal Infections of The Oral CavityDocument56 pagesFungal Infections of The Oral CavityAkash Anilkumar Malini100% (1)
- Case Study OF Hypokalemia Periodic ParalysisDocument34 pagesCase Study OF Hypokalemia Periodic ParalysisVivian Montesena BreganzaNo ratings yet
- CF Host Dept List 2023 24 v10 1Document99 pagesCF Host Dept List 2023 24 v10 1Antal Dorin CristianNo ratings yet
- Tyrese Carter EDPM SBADocument50 pagesTyrese Carter EDPM SBAArisha Nichols0% (1)
- General Survey Vital Signs: Donniedex P. Parrocha JD, MSN (C), RNDocument26 pagesGeneral Survey Vital Signs: Donniedex P. Parrocha JD, MSN (C), RNRamzen Raphael DomingoNo ratings yet
- NCLEX PracticeDocument18 pagesNCLEX Practiceandrew504777No ratings yet
- A5 - Sudden Cardiac DeathDocument61 pagesA5 - Sudden Cardiac DeathMedhat SabriNo ratings yet
- Radiation Oncology - Toxicity - RTOG - Wikibooks, Open Books For An Open WorldDocument15 pagesRadiation Oncology - Toxicity - RTOG - Wikibooks, Open Books For An Open WorldJosep GamarraNo ratings yet
- Physical Examination Pediatric: By: Erni Setiyorini, S.Kep.,NsDocument68 pagesPhysical Examination Pediatric: By: Erni Setiyorini, S.Kep.,NsReka DwiNo ratings yet
- PainDocument1 pagePainDANICA CALOMADRENo ratings yet
- The Allergy Report - The American Academic of Allergy, Asthma & Immunology - Diseases of The ADocument196 pagesThe Allergy Report - The American Academic of Allergy, Asthma & Immunology - Diseases of The ABogdan ClujNo ratings yet
- Photovoice Paper Obscured Gynecological AbnormalitiesDocument11 pagesPhotovoice Paper Obscured Gynecological Abnormalitiesapi-534841603No ratings yet
- Ankylosing Spondylitis PresentationDocument12 pagesAnkylosing Spondylitis Presentationapi-390014321No ratings yet
- Mood DisorderDocument18 pagesMood Disorderbemina jaNo ratings yet
- Cluster HeadachesDocument2 pagesCluster HeadachesMaple YuehNo ratings yet