Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
Exploring the Clinical Characteristics, Chromosomal
Analysis, and Emotional and Social Considerations in
Parents of Children with Down Syndrome
Dr. Sachin Padman, Dr. Kusuma Sachin Dr. Venugopal Reddy I.
Director of Pediatric and Neonatal Medical Officer, Sunrise Medical Director & Consultant
Divison, Sunrise Hospital, Hospital, Kanhangad, Pediatrician, Ovum Hospital,
Kanhangad, Kerala Kerala Bangalore, Karnataka
Abstract:- Down syndrome, also known as trisomy 21, is All patients with Down syndrome have three copies of
a common chromosomal disorder that affects one in chromosome 21.95% have 47chromosome with trisomy of
every 750/1000 live births. It is characterized by delayed 21 chromosome.5% have 46 chromosomes with abnormally
milestones and repeated chest infections, with most translocated 21st chromosome. Robertsonian translocation
children having microcephaly, low set ears, flat nasal involves transfer of chromosomal materials from
bridge, simian crease, umbilical hernia, CVS findings, chromosome 21 to chromosome 13,14 or 15.
and repeated ear infections. The risk of Down syndrome
increases to 1:20 for mothers over 40 years old. A study Having a child with mental retardation is considered a
examined 30 children with phenotype suggestive of stigma in society and parents have to undergo a lot of
Down syndrome, with a male to female ratio of 0.76:1. mental and financial stress. Hence it was decided to take up
The median age at presentation was 7 years, with a the study to know the psychosocial aspects of parents as
minimum of 3 years and a maximum of 12 years. The well as to correlate the clinical profile with genetics.
mean maternal age at child birth was 32 years, with
13.3% of the children born out of consanguineous The study also analyses the knowledge the parents
marriage. have, their perceptions about the condition, the issues after
the diagnosis like the course, outcome, treatment options
The study found that none of the mothers had a etc and the need to address the specific issues of individual
history of abortions, and 6.7% had complications families during counselling.
during pregnancy. The most common complaint was
delay in attainment of mile stones (96.7%) followed by II. MATERIALS AND METHODS
recurrent LRTI & URTI (13.2%), with 2 having heart
disease and 1 having family history of asthma. Thirty children with phenotypic features of Down
syndrome attending paediatric outpatient department of
Physical characteristics included microcephaly Government Wenlock Hospital and KMC Hospital, Attavar,
(86.7%), low set ears, a flat nasal bridge (96.7%), half of Mangalore from November 2007 to August 2008, aged 3 to
the children had simian crease and umbilical hernia 14yrs were included in the study. Children were enrolled
(50%), excessive skin on the back (76.7%), muscular into the study as and when they approached either the OPD
hypotonia (66.7%), dermatoses (26.7%), and or IPD.
hypothyroidism (10%). Cerebral findings were found in
15 children (50%), with endocardial cushion defects A written consent was taken after explaining the
being the most common. ASD (13.04%) was most procedure to the parents Data concerning the clinical details
common in 12 children, followed by VSD (10.86%), and were obtained from medical records of the study group.
PDA (4.3%) was present in 4.3%.
During the visit, height was recorded on the
Keywords: - Down Syndrome, Abortions, Heart, Diseases, stadiometer to the nearest 0.5 cm and weight on an
Hypothyroidism. electronic weighing machine to nearest 5 Gms. Head
circumference was measured to the nearest millimeter using
I. INTRODUCTION non stretchable fiberglass tape.
Down syndrome or trisomy 21 was first reported by Microcephaly was defined as head circumference less
Langdon Downin 1866. It is one of the most common than 3 standard deviation of mean for age. Blood pressure
chromosomal disorders occurring one in every 750/1000 was measured in appropriate sized cuff covering 2/3 rd of
live births. In mothers less than 25 years the risk is 1:2000, arm circumference in upper limb.
over 40 years the risk increases to 1:20.
IJISRT24MAR2090 www.ijisrt.com 3016
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
Blood samples were drawn and sent to genetic lab of Table 3: The Number of Pregnancies in Mothers of the
KMC, Manipal for karyotyping for those children who had children with down syndrome 36% mothers were gravida 3
not undergone karyotyping before. and 3.3% were Gravida 6.
Psychosocial assessment of the parents was done with Gravida
a predetermined semi structured pro forma. Frequency Percent
G1 2 6.7
The collected data was fed into the computer and G2 11 36.7
analysis was done using SPSS version 11(Statistical G3 9 30.0
Package for Social Sciences) statistical test chi square was G4 4 13.3
used for analysing the qualitative data and for the G5 3 10.0
quantitative variables student t test will be done. P< 0.05 G6 1 3.3
will be taken as statistically significant. Total 30 100.0
III. RESULTS AND ANALYSIS Table 4: Frequency of Previous still birth and Abortion in
the mothers 96.7% of mothers had no previous history of
Table 1: Total Children Including in the study were 30, Out stillbirth and no history of abortion.
of which 13 are Male and 17 are Females
Still Birth
Sex Frequency Percent
2 1 3.3
Frequency Percent Nill 29 96.7
M 13 43.3 Total 30 100.0
F 17 56.7
Total 30 100.0 Abortion
Frequency Percent
Age & Sex Distribution Nil 30 100.0
Sex Total Table 5: Frequency of Previous Childbirth with Down
M F Syndrome Only one Mother (3.3%) had a Child with
Less than 5 yrs 9 10 19 Down Syndrome in Previous Birth
Count % 47.4% 52.6% 100.0%
5-6 yrs 4 5 9 Previous Birth with Down
Count % 44.4% 55.6% 100.0% Frequency Percent
Gtr/eql 0 2 2 Nil 29 96.7
Count % 0% 100.0% 100.0% Normal 1 3.3
Total 13 17 30 Total 30 100.0
Count % 43.3% 56.7% 100.0%
Table 6: Type of Delivery in the Mothers 26 (86.7%) of the
Table 2: Consanguinity Mothers had Delivered Normally and 4 (13.3%) had
Frequency Percent Undergone LSCS
2nd Degree Consanguinity 1 3.3
3rd Degree Consanguinity 3 10.0 Delivery Type
Nil 26 86.7 Frequency Percent
Total 30 100.0 LSCS 4 13.3
Normal 26 86.7
1 (3.3%) of children had history of second degree Total 30 100.0
Consanguinity.
3 (10%) children had history of Consanguinity among Table 7: Complications during delivery 96.7% of mothers
Parents. had no complications
Any Complications
Frequency Percent
Yes 1 3.3
No 29 96.7
Total 30 100.0
IJISRT24MAR2090 www.ijisrt.com 3017
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
Table 8: Complications in the Down Children after Table 10: Clinical Features of Down Syndrome Observed
Delivery in the children during presentation in the OPD
EYE
Delayed Meconium yes % No %
Frequency Percent Upward Slanting 29 96.7 1 3.3
Yes 4 13.3 Brushfield spots 6 20 24 80
No 26 86.7 Anyother 28 93.3 2 6.7
Total 30 100.0
ENT
Constipation Yes % No %
Frequency Percent Ear Infection 6 20 24 80
Yes 5 16.7 Flat Nasal 29 96.7 1 3.3
No 25 83.3 Bridge
Total 30 100.0 Small Mouth 28 93.3 2 6.7
Protruding 22 73.3 8 26.7
Prolonged Jaundice Tongue
Frequency Percent High Arched 27 90 3 10
Yes 9 30.0 Palate
No 21 70.0 Low set ears 29 96.7 1 3.3
Total 30 100.0
Other Features Observed in the Down Children
Respiratory Distress
Frequency Percent Skin Dermatoses
Yes 3 10.0 Frequency Percent
No 27 90.0 No 22 73.3
Total 30 100.0 Yes 8 26.7
Total 30 100.0
Cardiac Complications
Frequency Percent Excessive Skin on the Back
Yes 4 13.3 Frequency Percent
No 26 86.7 No 9 30.0
Total 30 100.0 Yes 21 70.0
Total 30 100.0
Table 9: Chief Complaints in the children when presenting
in the OPD 30% of the children presented to the OPD with Muscular Hypotonia
complaints of delayed milestones 50% of the children had Frequency Percent
Umbilical hernia No 10 33.3
Yes 20 66.7
Chief Complaints Total 30 100.0
Frequency Percent
No Complaints 14 46.7 Hyper Flexibility
Cold/Fever 2 6.7 Frequency Percent
Delayed Milestones 9 30.0 No 7 23.3
Development 1 3.3 Yes 23 76.7
Loose Stools & Vomiting 1 3.3 Total 30 100.0
Recurrent Chest Infection 2 6.7
Recurrent cold / Chest 1 3.3 Simian Crease
Infection 30 100.0 Frequency Percent
Total No 15 50.0
Yes 15 50.0
Umbilical Hernia Total 30 100.0
Frequency Percent
No 15 50.0 Hypothyroidism on Treatment
Yes 15 50.0 Frequency Percent
Total 30 100.0
No 27 90.0
Yes 3 10.0
Total 30 100.0
IJISRT24MAR2090 www.ijisrt.com 3018
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
Microcephaly Knowledge about cause of the condition
Frequency Percent Frequency Percent
Microcephaly 26 86.7 Excess of work 2 6.7
Normal 4 13.3 during Pregnancy 2 6.7
Total 30 100.0 A curse of the Gods 26 86.7
A Medical Cause 30 100.0
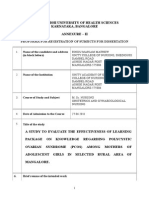
Table 11 Karyotyping Results Total
Report of Chromosome analysis and Karyotype Reaction to the Diagnosis
Frequency Percent
Patient Name: Abhay Krishna Depressed 15 50.0
Case Name: L003361 Felt Guilty 5 16.7
Age: 6 yrs Fraustrated/Worried 5 16.7
Date of Birth: 8/03/08 Acceptance 5 16.7
Specimen Type: Peripheral Blood Total 30 100.0
Referral Reason: D.S
Result: Chroosome analysis by blood Microculture and Source of Help approached
GTG branding shows 47, XY, + 21 in all the 20 Frequency Percent
metaphase plates analysed. Doctor 25 83.3
Case Comment: 1 Cytogenetically this is a case of free Faith Healer 3 10.0
trisomy 21 indicating Down syndrome. 2 Genetic Counselor 0 0
counselling advised. 3. Prenatal diagnosis can be Religious Leader 2 6.7
offered in cause of future pregnancies. Total 30 100.0
Karyotyping Support for the Family and Child
Frequency Percent Frequency Percent
Mosaicism Robertsonian 1 3.3 Family Support 25 83.0
Translocation 1 3.3 Emotional & Financial 0 0
Trisomy 21 28 93.3 No, No Support from 5 17
Total 30 100.0 family members 0 0
Support from social 30 100.0
Table 12: Showing Details of Psychosocial Issues in Organisations
Parents of the Down’s Children Any other
Total
Mothers Occupation
Frequency Percent Telling the family about the condition and needs of children
Homemaker 27 90.0 Frequency Percent
Tailor 1 3.3 Have Told 24 80.0
Teacher 2 6.6 Haven’t Told 2 7.0
Total 30 100.0 Have told, but 4 13
interpersonal
Mothers Education Relationship 30 100.0
Frequency Percent affected
Graduate 5 16.6 Total
PUC 15 50.0
SSLC 10 33.3 Relationship of the Child with Siblings
Total 30 100.0 Frequency Percent
Patient and caring towards 18 60.00
How Parents Came to know the Condition of the Child the child 2 6.70
Frequency Percent Don’t involve in the 10 33.30
Appearance of Child 14 46.7 activities of the child 0 00
She was not able to 12 40.0 Get frustrated at times 30 100.0
sit/crawl. 4 13.3 Make fun of the child
Doctor diagnosed. 30 100.0 total
Total
IJISRT24MAR2090 www.ijisrt.com 3019
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
Time Spent by Child during the Day Letting child play with other children in the neighbourhood
Frequency Percent Frequency Percent
At home 20 66.7 Often 11 36.70
Special School 10 33.3 Sometimes 18 60.00
Normal School 0 0 Don’t let child Play 1 3.30
Others 0 0 Total 30 100.0
Total 30 100.0
Special Quality do Recognised in Child
Frequent Change of School Frequency Percent
Frequency Percent Music and dance 21 70.00
Cannot learn or play 0 0 Drawing using colors 2 6.70
Other children do not join him in play 0 0 Both 7 23.30
Doesn’t change schools often 11 37.3 Total 30 100.0
Stays at home 19 63.3
Total 30 100.0 Encouraging Child to Participate in Games and Sports
Frequency Percent
Does Parent Get Time for Leisure Activities No 10 33.30
Frequency Percent Yes 4 13.30
Most of time is spent with child 9 30.0 Cant say 16 53.30
Get enough time for self 16 53.0 Total 30 100.0
Gets time and involves child too 5 17
in recreational activities 30 100.0 Worry about Future of Child When He/She Grows Up
Total Frequency Percent
Child can never be independent 10 33.30
Situation at home when there are visitors Child will be able to earn his living on 9 30.00
Frequency Percent his own
Child kept away from visitors 25 83.3 Cant say 11 36.70
Visitors don’t interact with child 2 6.7 Total 30 100.00
Child involved in interaction with 3 10
visitors 30 100.0 Ways Tried to Make Child Confident like any other Normal
Total Child
Frequency Percent
Family Participation in Socio Religious Functions/Family Encourage to speak to people/Take 11 36.70
Gatherings? child our with the family 8 26.70
Frequency Percent Make child feel like a normal child 11 36.70
Participate with the child 25 83.3 Unable to instill confidence in child 30 100.0
Participate without the child 2 6.7 Total
Don’t participate in family 3 10
functions 30 100.0 Leaving the Child by Himself
Total Frequency Percent
Yes, Most of the time 2 6.7
Relationship of child with neighbours Feel Embrassed when child gets into 2 6.7
Frequency Percent trouble with others
No Interaction with Child 5 16.70 Afraid child will hurt himself/others will 26 86.7
Problems in the 23 76.70 hurt him
neighbourhood 0 00 Total 30 100.0
Children in neighbourhood 2 6.70
play with child 30 100.0 Getting Annoyed and Impatient when Teaching Child
Total Frequency Percent
Often 0 00
Involvement in Child’s School Activities Sometimes 14 46.70
Frequency Percent Don’t get annoyed 16 53.30
Visit School and PTA 10 33.30 Total 30 100.00
Help with homework 8 26.70
and teach at home 12 40.00 Attempt Made to Improve Vocabulary of Child
Don’t involve with 30 100.00 Frequency Percent
school activities Speak to child and explain 3 10.0
Total Child able to understand & Speaks 10 33.3
day to day things
Difficuly to speak as child cannot 17 56.7
IJISRT24MAR2090 www.ijisrt.com 3020
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
understand Physical characteristics included microcephaly
Total 30 100.0 (86.7%), low set ears and a flat nasal bridge (96.7%). Half
of the children had simian crease and umbilical hernia
The Risk Child Faces the Most (50%), excessive skin on the back (76.7%), muscular
Frequency Percent hypotonia (66.7%), dermatoses (26.7%), and
Social Rejection and Loneliness 11 36.7 hypothyroidism (10%).
Scholastic Backwardness and 18 60.0
Dependence 1 3.3 Cerebral findings were found in 15 children (50%),
Child Abuse 30 100.0 with endocardial cushion defects being the most common.
Total ASD (13.04%) was most common in 12 children, followed
by VSD (10.86%), and PDA (4.3%) was present in 4.3%.
Monthly Expenditure on the Child (in Rupees) Mental IQ assessment revealed that 18 out of 92 children
Frequency Percent had mild mental retardation (IQ 50-70), most were in the
Greater 500 0 0 moderate group (IQ ranging from 35 to 50), 60 children had
500-1000 21 70.0 moderate mental retardation, and 14 children had severe
Less 1000 9 30.0 mental retardation (IQ 20-35).
Total 30 100.0
The study reveals that 93.3% of children with Down
Bearing the Expenses of Child syndrome have trisomy 21 with non dysjunction, while
Frequency Percent 3.3% have Robertsonian translocation and mosaicism. Out
Parents 24 80.0 of the 30 children, 90% are homemakers, 33.3% are
educated up to the tenth standard, 50% are graduates, and
Voluntary 6 20.0
organisation 0 0 10% are employed. Parents come to know their child's
Government 30 100.0 condition by appearance, 40% by delayed milestones, and
13.3% are diagnosed by a doctor. 86.7% of parents are
Total
aware of the condition, while 6.7% believe it is caused by
excess work during pregnancy.
Professional Counselling Being Done for the Child
Frequency Percent
50% of parents are depressed when they know their
No 9 30.0 child has Down syndrome, while 6.7% feel guilty and 6.7%
Monthly 3 10.0
accept the condition. 83.3% of parents approach a doctor,
Only When need 18 60.0 10% seek a faith healer, and 6.7% go to a religious leader
arises 30 100.0 when they first learn about the condition. 83% of parents
Total have support from family members and 17% have support
from social organizations.
Have the Parents Enrolled in any Support Group
Frequency Percent 80% of parents have told their family members about
Yes 5 16.7 the condition, while 7% have not. In 13% of cases, the
No 25 83.3 interpersonal relationships of family members have been
Total 30 100.0 affected. Siblings are patient and caring towards the Down
child, while 61% get frustrated and 6.7% do not involve in
IV. DISCUSSION any of the child's activities.
Down syndrome is a common autosomal abnormality 66.7% of Down's children spend most of the day at
in humans, affecting 1 in 750 live births. In this study, 30 home, and 33.3% attend special school. Parents have
children with phenotype suggestive of Down syndrome enough time for leisure activities, and 83.3% participate in
were studied, with a male to female ratio of 0.76:1. The family functions with the child. Visitors who come home do
median age at presentation was 7 years, with a minimum of not interact with the child.
3 years and a maximum of 12 years. The mean maternal
age at child birth was 32 years, with 13.3% of the children 76.7% of children face problems in the neighborhood,
born out of consanguineous marriage. and 16.7% have no interaction with the child. 40% of
parents do not involve in school activities, while the rest
The study found that none of the mothers had a participate in PTA meets and help with homework.
history of abortions, and 6.7% had complications during
pregnancy. The most common complaint was delay in 53.3% of parents teach the child basic skills like
attainment of mile stones (96.7%) followed by recurrent brushing and bathing, and 33.3% teach them small moral
LRTI & URTI (13.2%), with 2 having heart disease and 1 lessons. Only 60% of parents let their child play with other
having family history of asthma. children in the neighborhood.
IJISRT24MAR2090 www.ijisrt.com 3021
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
Most parents believe that their child will face [6]. Pueschel SM, Sassaman EA, scola PS, Sark AM,
academic backwardness and dependance, social rejection Horrobin M: Biomedical Aspect In Down
and loneliness, and child abuse. Monthly expenses for the Syndrome: Down syndrome Advances in
child range from 500-1000 rupees, with 80% of parents Biomedicine and the Behavioural sciences
bearing the costs themselves. Cambridge , MA, ware press 1982; p169
[7]. Thomas fogle T, Goldman C.A: study of genetics of
V. CONCLUSIONS compliestrait using dernatoglyphics from Down
Syndromeand studypopulation pages 12-150
The study examined 30 children with Down [8]. Hall B: Mongolism in new born infants clinic
syndrome, focusing on their clinical features, karyotyping pediatrics (phila) 1966; 5:4-12
results, and psychosocial issues. The most common [9]. Rowe Rd, uchida IA: cardiac malformations in
complaint was delayed milestones and repeated chest mongolism: A prospective study of 184 children Am
infections. Most children had microcephaly, low set ears, J med 1961; 31; 726-35
flat nasal bridge, simian crease, umbilical hernia, CVS [10]. Borowski A, Zeuchner: Pediatric Cardiology 1966;
findings, and repeated ear infections. Karyotyping results 17 (6): 375-81
showed that 93.3% of the children had trisomy 21 with non [11]. Wilson Sk, Hutchins GM, Neil CA: Hypertensive
dysjunction, Robertsonian translocation, and mosaicism, pulmana vascular discase in Down syndrome J of
making trisomy 21 nondysjunction the most common Pediatrics 1979;95 7 22
chromosomal anomaly among the three variants. [12]. Green wood RD, Nadas AS: The clinical course of
cardiac discase in down syndrome. Pediatrics 1976;
Parents' psychosocial issues depend on their 58 93-97
knowledge about the condition, family relationships, [13]. Morgan SB: Development and distribution of
parental adjustment to the child's demands, financial status, intellectual and adaptive skills in Down syndrome
facilities available for the child, and support from extended children; Implications of early intervention: Mental
family and social groups. Parents who were well-informed retard 1979; 17 247
about Down syndrome showed improved adjustment, less [14]. Sinhell RR: Psychomotor Development in pueschell
stress, and a more positive perception of their child. Quality SM (ed): The young child with Down syndrome
of life for the child was better in families where members new York Human sciences press 1984,207
felt connected and supported by each other. [15]. TU J.B Zellweger H: Blood serotonin deficiency in
Down syndrome lancet 1965; 2:715
Sibling relationships were also crucial for children [16]. Wuse P, Koch R, snow KF, Ronenfeld MJ The use
with Down syndrome. Most children faced neighborhood of 5-HTP in the treatment of Down syndrome.
problems and less interaction with visitors, but parents Pediatrics 1974; 54; 165
played a significant role in their child's development and [17]. Coleman M: Infantile spasms induced by 5
family functioning. Many parents taught basic skills like Hydroxytryptophan in patients with Down
brushing, bathing, and moral lessons, and recognized their syndrome: Neurology 1971; 21: 911
interest in music and dance. [18]. Wang PP S Hess link JR: Callosal morphology
concurs with neurobehavioral and neuropathological
Approximately 80% of parents were not involved in findings in neuropdevelopmental disorders Arch
any support group and only sought counseling when neurol 1992; 49(4): 407-14
needed. There was less awareness about services and [19]. Folsom Rc, Widen JE, W Wilson WR: Auditory
support available to children with Down syndrome. Early brain stem responses in infants with Down
intervention programs, pre-school nurseries, and inclusive Syndrome Arch otolaryngology 1983; 109:609
special education strategies positively influenced children's [20]. Squires N, Olloc AR: Auditory brain stem retarded
overall functioning. children: Audiometry 1986; 7: 83.responses in
mentally
REFERENCES [21]. Fabia J, Drolette M: Malformation and leukemia in
children with Down syndrome: pediatrics 1970; 45:
[1]. Down JLH: Observations on an ethnic 60-4
classifications of idiotsLondon Hospclinlects Reps [22]. Buchin PJ, Schillinger JW: Down syndrome and the
1866; 3:259 gastrointestinal trait J clinical Gastroenterology
[2]. Polani PE, Briggs JH et al: A Mongol girl with 46 1986:8:111
chromosomes Lancet 1960; 1:721-24 [23]. Milunasky A, Fisher JH: Annular pancreas in Down
[3]. Penrose LS, Ellis JR, Delhanty JDA: chromosome syndrome: Lancet 1968; 2:575
translocation in mongolism and in normal relative [24]. Shapiro MB, France TD. The ocular features of
lancet 1960; 2:409-10 Down syndrome: AM J opthalmology 1985; 659-63
[4]. Clarke CM Edward JH: 21 trisomy / normal [25]. Eissler R, Logenecker LP: The common eye
mosaicism in an intelligent girt with some findings in Mongolism Am J opthalmol 1962; 54;
mongoloid characters Lancet 1961; 1; 1028 30 398-40
[5]. Han hart E, Delhanty JDA, Penrose LS: trisomy in
mother and child Lancet 1961; 1:403
IJISRT24MAR2090 www.ijisrt.com 3022
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR2090
[26]. Wong V, Ho A ocular abnormalities in down
syndrome an analysis of 140 cleanse children
pediatrneurol 1997; 16(4):3 11-4
[27]. American Academy of pediatrics committee on
genetics: Health supervision of children with Down
syndrome. Pediatrics 2001 107;442-49
[28]. Roizen NJ, Wolters C, Nicole T, Blondis T: Hearing
loss in children with down syndrome. Paediatrics
1992; 123: 59
[29]. Marcus CL, Keens TG, Bauesa DB et al: Oral
Hygiene in children with Down syndrome pediatrics
1991; 88; 132
[30]. Baxter RG master FIR Myles K: Down syndrome
and thyroid function in adults lancet 1975;2:794
[31]. Davis RH, Pitkow HS, Hill HG: Down syndrome
and thyroid function Lancet 1975; 2: 1308
[32]. Peuschel SM, Puzzullo JC: Thyroid dysfunction in
down syndrome AM J Dis child 1985; 139:636
[33]. Cuter AT, Benezra, Obiter R, Brink SJ: Thyroid
function in child with Down syndrome: Am J Dis
child 1986; 140 479
[34]. La franchi SH: Pediatric clinic of North America;
Hypothyroidism: Kaplan SA (ED) 1979; 26(1): 46.
IJISRT24MAR2090 www.ijisrt.com 3023
You might also like
- Anders Olsen, Matthew S. Gill Eds. Ageing Lessons From C. Elegans PDFDocument433 pagesAnders Olsen, Matthew S. Gill Eds. Ageing Lessons From C. Elegans PDFPhil BoileauNo ratings yet
- General Pharmacology MCQs PDFDocument41 pagesGeneral Pharmacology MCQs PDFTaonga Zulu90% (21)
- Renal SystemDocument85 pagesRenal SystemFerasKarajehNo ratings yet
- Cloning Vectors: Types & CharacteristicsDocument18 pagesCloning Vectors: Types & Characteristicsayush100% (1)
- Virology MCQ 1Document21 pagesVirology MCQ 1Robert Edwards100% (9)
- Quiz 1A Hema LecDocument17 pagesQuiz 1A Hema LecAngela ReyesNo ratings yet
- Etiology of The Psychopathic Serial KillerDocument10 pagesEtiology of The Psychopathic Serial KillercomplinotionNo ratings yet
- Inheritance Biology IGCSE WorksheetDocument2 pagesInheritance Biology IGCSE WorksheetJia Ru100% (2)
- Immunology of Transplant RejectionDocument8 pagesImmunology of Transplant Rejectionxplaind100% (1)
- Haplogroup R1a As The Proto Indo Europeans and The Legendary Aryans As Witnessed by The DNA of Their Current Descendants A.KlyosovDocument13 pagesHaplogroup R1a As The Proto Indo Europeans and The Legendary Aryans As Witnessed by The DNA of Their Current Descendants A.KlyosovSanja Jankovic100% (1)
- HydroxyureaDocument2 pagesHydroxyureaBigBoostingNo ratings yet
- Adolescents With Tuberculosis-A Review of 145 Cases, 2016Document5 pagesAdolescents With Tuberculosis-A Review of 145 Cases, 2016Yoseph Arif Putra100% (1)
- Maternal and Fetal Outcome of Placenta PDocument5 pagesMaternal and Fetal Outcome of Placenta Pfamelalusu eaNo ratings yet
- HHS Public Access: Spontaneous Resolution and Timing of Intervention in Congenital Nasolacrimal Duct ObstructionDocument11 pagesHHS Public Access: Spontaneous Resolution and Timing of Intervention in Congenital Nasolacrimal Duct Obstructionmono1144No ratings yet
- Advances in Prenatal Screening For Down Syndrome - General Principles and Second Trimester TestingDocument16 pagesAdvances in Prenatal Screening For Down Syndrome - General Principles and Second Trimester TestingMáthé AdriennNo ratings yet
- Migliore 2005Document7 pagesMigliore 2005Ruxandra CretuNo ratings yet
- Scenario of Retinoblastoma Among Bangladeshi Children - A Single Center Experience of 10 YearsDocument5 pagesScenario of Retinoblastoma Among Bangladeshi Children - A Single Center Experience of 10 YearsBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- J Semperi 2006 01 001Document9 pagesJ Semperi 2006 01 001Máthé AdriennNo ratings yet
- Epidemiological Predictors of Metabolic SyndromeDocument3 pagesEpidemiological Predictors of Metabolic SyndromeAnonymous izrFWiQNo ratings yet
- Chromosomal Analysis of Mentally Retarded Children With MicrocephalyDocument12 pagesChromosomal Analysis of Mentally Retarded Children With MicrocephalyWiyosa RusdiNo ratings yet
- Conclusions: Background:: Oral Abstracts / J Pediatr Adolesc Gynecol (2013) E47ee53 E49Document2 pagesConclusions: Background:: Oral Abstracts / J Pediatr Adolesc Gynecol (2013) E47ee53 E49fujimeisterNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofSuwandi ChangNo ratings yet
- Study of The Frequency of Down Syndrome in A North East Indian PopulationDocument4 pagesStudy of The Frequency of Down Syndrome in A North East Indian PopulationeditorijmrhsNo ratings yet
- Comp 1 SSCDocument9 pagesComp 1 SSCRoberto Peter Joseph DarkeNo ratings yet
- Written Speech NewDocument5 pagesWritten Speech NewMUHAMMAD FAIZ BIN ABDUL HALIMNo ratings yet
- Risk Factor For Relapse in Childhood Nephrotic SynDocument6 pagesRisk Factor For Relapse in Childhood Nephrotic Syndody abdullahNo ratings yet
- Down'S Syndrome: DR Sarah MaclennanDocument6 pagesDown'S Syndrome: DR Sarah MaclennanElison J PanggaloNo ratings yet
- Guía Trisomía 13Document7 pagesGuía Trisomía 13Galy Crt FlzNo ratings yet
- Presentation, Complications and Management Outcome of Community Acquired Pneumonia in Hospitalized Children in Maiduguri, NigeriaDocument4 pagesPresentation, Complications and Management Outcome of Community Acquired Pneumonia in Hospitalized Children in Maiduguri, NigeriaklaukakoNo ratings yet
- Prevalence of Tourette Syndrome and Chronic Tics I PDFDocument16 pagesPrevalence of Tourette Syndrome and Chronic Tics I PDFFitriazneNo ratings yet
- Research Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyDocument2 pagesResearch Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyadhastriNo ratings yet
- Cancer EpidemiologyDocument4 pagesCancer Epidemiologyratna puspitasariNo ratings yet
- NIPTDocument3 pagesNIPTUmber AgarwalNo ratings yet
- Arumugam Et Al-Clinical Anatomy 2Document10 pagesArumugam Et Al-Clinical Anatomy 2Kavitha RajaNo ratings yet
- Clinical-Diagnostic Features of Duchenne Muscular Dystrophy in ChildrenDocument3 pagesClinical-Diagnostic Features of Duchenne Muscular Dystrophy in ChildrenFajri MuhammadNo ratings yet
- Pediatric Intracranial Aneurysms. Experience of 47 Cases.: Corresponding AuthorDocument8 pagesPediatric Intracranial Aneurysms. Experience of 47 Cases.: Corresponding AuthorVoicu AndreiNo ratings yet
- Downs SyndromeDocument9 pagesDowns Syndromesig maraNo ratings yet
- Jurnal KustaDocument14 pagesJurnal KustaarrummanantiNo ratings yet
- Nejme2032499 PDFDocument2 pagesNejme2032499 PDFBladimir CentenoNo ratings yet
- Aneurismas Cerebrais Na InfânciaDocument5 pagesAneurismas Cerebrais Na Infânciaarlindodavila2010No ratings yet
- NPE Lupus Early 2009Document8 pagesNPE Lupus Early 2009Maria GarabajiuNo ratings yet
- Bastonero 2012Document1 pageBastonero 2012Ricky SilaenNo ratings yet
- Review of Maternal Mortality at A Tertiary Care Hospital - A One Year StudyDocument5 pagesReview of Maternal Mortality at A Tertiary Care Hospital - A One Year StudyIJAR JOURNALNo ratings yet
- Clinical Study and Management of Hydrocephalus inDocument5 pagesClinical Study and Management of Hydrocephalus inVirajannatiNo ratings yet
- Risk Factors For Sleep-Disordered Breathing in Children: Associations With Obesity, Race, and Respiratory ProblemsDocument6 pagesRisk Factors For Sleep-Disordered Breathing in Children: Associations With Obesity, Race, and Respiratory ProblemsMiral BassNo ratings yet
- Fluconazole Susceptibility Pattern of Candida SP in Pregnant Women in A Tertiary Healthcare CenterDocument8 pagesFluconazole Susceptibility Pattern of Candida SP in Pregnant Women in A Tertiary Healthcare Centerijmb333No ratings yet
- Icbt07i4p369 PDFDocument6 pagesIcbt07i4p369 PDFretNo ratings yet
- Diphtheria ReemergenceDocument5 pagesDiphtheria ReemergenceDatu Nur-Jhun Salik, MDNo ratings yet
- Artikel IlmiahDocument15 pagesArtikel IlmiahDewi PrasetiaNo ratings yet
- Genetic - Down SyndromeDocument11 pagesGenetic - Down Syndromelightning proNo ratings yet
- Grinshpun Cohen Et Al 2015 Health ExpectationsDocument12 pagesGrinshpun Cohen Et Al 2015 Health ExpectationsmaneshaputraNo ratings yet
- SIFILIS Archdischild 2020 320549Document7 pagesSIFILIS Archdischild 2020 320549Ferdi KapisaNo ratings yet
- Validity of A Minimally Invasive Autopsy For CoD Determination On Stillborn Babies and Neonates in MozambiqueDocument17 pagesValidity of A Minimally Invasive Autopsy For CoD Determination On Stillborn Babies and Neonates in MozambiqueDenys PutraNo ratings yet
- High-Grade Cervical Squamous Intraepithelial LesioDocument6 pagesHigh-Grade Cervical Squamous Intraepithelial LesiodiazdianadpNo ratings yet
- Effect of Low Birth Weight On Neonatal Mortality in Preterm and Small For Gestational Age Babies in A Tertiary Neonatal Intensive Care Unit in IndiaDocument4 pagesEffect of Low Birth Weight On Neonatal Mortality in Preterm and Small For Gestational Age Babies in A Tertiary Neonatal Intensive Care Unit in Indiazara irdinaNo ratings yet
- Epidemiology of Dysmenorrhea Among University of Dschang Students (West Region, Cameroon) : A Cross-Sectional StudyDocument6 pagesEpidemiology of Dysmenorrhea Among University of Dschang Students (West Region, Cameroon) : A Cross-Sectional StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- JURNAL MomayyeziDocument14 pagesJURNAL MomayyeziSeptianNo ratings yet
- Trisomy 18: Prenatal Diagnosis and Outcome in A Tertiary Care Fetal Medicine Center in South IndiaDocument13 pagesTrisomy 18: Prenatal Diagnosis and Outcome in A Tertiary Care Fetal Medicine Center in South IndiaElna EstherNo ratings yet
- Jurnal KustaDocument14 pagesJurnal KustaRobertus ElvantoraNo ratings yet
- Radiological Findings of Pulmonary Tuberculosis in Infants and Young ChildrenDocument5 pagesRadiological Findings of Pulmonary Tuberculosis in Infants and Young ChildrendtmNo ratings yet
- Journal NeuroDocument5 pagesJournal NeuroStevany LiangNo ratings yet
- J of Obstet and Gynaecol - 2020 - Samura - Update On Noninvasive Prenatal Testing A Review Based On Current WorldwideDocument9 pagesJ of Obstet and Gynaecol - 2020 - Samura - Update On Noninvasive Prenatal Testing A Review Based On Current Worldwidejazz castañedaNo ratings yet
- Trisomy 21 ThesisDocument7 pagesTrisomy 21 Thesiswah0tahid0j3100% (2)
- Journal Homepage: - : Manuscript HistoryDocument11 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Spectrum of Symptoms in Women Diagnosed With Endometriosis During Adolescence Vs AdulthoodDocument11 pagesSpectrum of Symptoms in Women Diagnosed With Endometriosis During Adolescence Vs AdulthoodnicloverNo ratings yet
- Treatment For Benign Thyroid Nodules With A CombinDocument7 pagesTreatment For Benign Thyroid Nodules With A CombindarthjesussithNo ratings yet
- Ni Hms 911584Document24 pagesNi Hms 911584kiranaNo ratings yet
- 05 N026 31333Document13 pages05 N026 31333Ankur AggarwalNo ratings yet
- Evolution in Screening For Down Syndrome: ReviewsDocument7 pagesEvolution in Screening For Down Syndrome: ReviewsMayada Osman100% (1)
- Mosaic Trisomy 16Document13 pagesMosaic Trisomy 16apventure trip plannerNo ratings yet
- Brain Tumors in ChildrenFrom EverandBrain Tumors in ChildrenAmar GajjarNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth Through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth Through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web To Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web To Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System For Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System For Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation For Translating Global Languages Into Indian LanuagesDocument7 pagesHarnessing Open Innovation For Translating Global Languages Into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction Using Bi-LSTMDocument8 pagesAir Quality Index Prediction Using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict The Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict The Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Keywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalDocument7 pagesKeywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis On Mental Health Issues Among IndividualsDocument6 pagesAn Analysis On Mental Health Issues Among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson's Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolDocument31 pagesThe Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonDocument14 pagesTerracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions On Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions On Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- One H5N1 Paper Finally Goes To Press Second Greenlighted: InfluenzaDocument2 pagesOne H5N1 Paper Finally Goes To Press Second Greenlighted: InfluenzaVera MillerNo ratings yet
- Phenotypic Characterization of Class II MalocclusionDocument88 pagesPhenotypic Characterization of Class II MalocclusionPoonam K JayaprakashNo ratings yet
- Questions & Solutions of Aipmt-2010 (Mains) Test Paper: Important InstructionsDocument32 pagesQuestions & Solutions of Aipmt-2010 (Mains) Test Paper: Important InstructionsSankar Kumarasamy0% (1)
- Hericium Erinaceus - ReviewDocument24 pagesHericium Erinaceus - ReviewMV Analia CochettiNo ratings yet
- Application of The Bethesda Classification For Thyroid FNABDocument12 pagesApplication of The Bethesda Classification For Thyroid FNABJudrelle Krizia MarianoNo ratings yet
- Introduction To Biotechnology 3Rd Edition Thieman Test Bank Full Chapter PDFDocument12 pagesIntroduction To Biotechnology 3Rd Edition Thieman Test Bank Full Chapter PDFchastescurf7btc100% (8)
- A Descriptive Study of Diet in Family of Patients With Diabetes Mellitus Type 2Document9 pagesA Descriptive Study of Diet in Family of Patients With Diabetes Mellitus Type 2Ilham djafarNo ratings yet
- Anti Microbial DrugsDocument18 pagesAnti Microbial Drugseyadballas35No ratings yet
- Rage Against The Machine: Advancing The Study of Aggression Ethology Via Machine LearningDocument20 pagesRage Against The Machine: Advancing The Study of Aggression Ethology Via Machine LearningCony GSNo ratings yet
- Pathology MBBS MCQsDocument7 pagesPathology MBBS MCQsShahzad Asghar Arain100% (3)
- Revolutions in Biomedicine Summer School Brochure 2018Document14 pagesRevolutions in Biomedicine Summer School Brochure 2018Nicolas Fernando Schiappacasse VegaNo ratings yet
- Griffiths - Are Non Speech Oro-Motor Exercises More EffectiveDocument1 pageGriffiths - Are Non Speech Oro-Motor Exercises More EffectiveMira AlaaNo ratings yet
- Animalhealth Flyer Vetmax Aiv CO125306Document2 pagesAnimalhealth Flyer Vetmax Aiv CO125306Yoana GulenovaNo ratings yet
- Histochemistry Print PDFDocument4 pagesHistochemistry Print PDFEka Putra PratamaNo ratings yet
- Precios BiosystemsDocument8 pagesPrecios Biosystemsjoaquin140292No ratings yet
- Revtox 29 1 2012Document80 pagesRevtox 29 1 2012Oscar Eduardo SilvaNo ratings yet
- Evidence-Based Medicine: Lucman, Hakeymah Lunag, Tara Jane Magaoay, CheyserineDocument71 pagesEvidence-Based Medicine: Lucman, Hakeymah Lunag, Tara Jane Magaoay, CheyserinereadmeamllionNo ratings yet
- Cytoplasmic Particle by Nabablit NotesDocument3 pagesCytoplasmic Particle by Nabablit NotesJoshua NabablitNo ratings yet
- Kidney and Liver FunctionDocument6 pagesKidney and Liver FunctionAhmad Ripani Musyaffa AhdanLabNo ratings yet