Volume 9, Issue 4, April – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24APR2251
Implications of Adnexal Invasions in
Primary Extramammary Paget’s
Disease: A Systematic Review
Dr. Sabita Aryal 1; Dr. Liu Ye Qiang2,*
Shanghai Skin Disease Hospital, School of Medicine, Tongji University, No. 1278 Baode Road,
Shanghai, 200443, China
Corresponding Author:- Dr. Liu Ye Qiang2,*
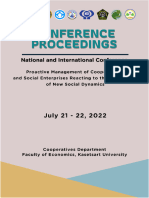
Abstract:- Extramammary Paget’s disease (EMPD) is an of EMPD manifestations: primary and secondary. Secondary
erratic malignant skin disorder primarily affecting skin EMPD involves the direct extension of an underlying
areas abundant with skin appendages like hair follicles. internal neoplasm or the epidermotropic spread of malignant
The vulva is most involved site, followed by genital areas, cells, whereas primary EMPD originates as an intraepithelial
penoscrotal regions and axillary skin. EMPD presents as neoplasm of the epidermis [4], while some theory
erythematous skin lesions resembling eczema, typically suggesting infiltration via adnexal structures (Figure 1).
progressing slowly, either primary or secondary Predominant cases of EMPD are identified as carcinoma In
manifestations. Primary EMPD originates as an Situ, which typically progresses slowly. However, local
intraepithelial neoplasm of the epidermis, often leading lymph node (LN) metastases and non-local metastases often
to local lymph node metastases and distant metastases. A occur once Paget cells penetrate deeply into the dermis [5].
systematic literature search using targeted keywords Due to the limited effectiveness of conventional
across multiple databases was conducted. Studies chemotherapies, which are typically used to treat EMPD,
focusing on EMPD, adnexal involvement, depth, cases with distant metastases with multiple lesions have a
recurrence, and prognosis were included by keeping in poor prognosis. Here, we review EMPD, covering its
view the objective which is to determine the significance diagnosis, pathogenesis, and treatment, with an emphasis on
of adnexal involvement and depth concerning recurrence recent developments.
and prognosis in the primary EMPD. Adnexal
involvement, especially in hair follicles and eccrine ducts,
is prevalent in primary EMPD. However, its correlation
with tumor progression or recurrence rates remains
inconclusive. Surgical excision, including Mohs
micrographic surgery, is the primary therapeutic
approach, with topical agents and systemic treatments
used in advanced cases. Future studies regarding
understanding adnexal involvement's depth and
significance are essential in designing effective targeted
therapeutic approaches in EMPD.
Keywords:- Disease of the Cutaneous Annexes, Primary
EMPD, Extramammary Paget’s Disease, Skin Neoplasm,
Prognosis, Skin Adnexa, Adnexal Involvement.
I. INTRODUCTION
First reported by Crocker in 1889, EMPD is a rare
malignant skin disorder that affects apocrine rich skin sites
with an abundance of hair follicles. [1, 2] The vulva is the
most often occurring site; perineal, perianal, scrotal, and
penile skin are next in frequency. The axilla, buttocks,
thighs, eyelids, and external auditory canal are additional,
less common locations. Typically, erythematous or persistent Fig 1 Adnexal Proliferation in Primary EMPD Showing
skin lesions resembling eczema are the first sign of EMPD. Pagetoid Cells Infiltrating the Dermal Layer via
[3] Another name for EMPD is skin in situ adenocarcinoma. Adnexal Structures
The tumor is limited to the epidermis, grows slowly, and
rarely spreads to other areas of the body. There are two types
IJISRT24APR2251 www.ijisrt.com 1179
Volume 9, Issue 4, April – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24APR2251
II. MATERIALS AND METHODOLOGY Exclusion Criteria
A. Study Design Studies published in languages other than English were
excluded due to potential limitations in comprehension
Research Question: and analysis.
The primary research question driving this systematic Literature lacking empirical evidence, including
review is: "What is the significance of adnexal involvement conceptual papers, reviews lacking original research,
and depth concerning recurrence and prognosis in primary case reports, case series, conference abstracts, or
extramammary Paget's disease (EMPD)?" theoretical discussions without practical implications,
were excluded.
Statement of Aims: Studies not specifically detailing adnexal involvement
This systematic review aims to comprehensively and depth in primary EMPD or not directly related to the
evaluate the significance of adnexal involvement and depth research questions were excluded.
in primary extramammary Paget's disease (EMPD)
concerning recurrence and prognosis. The review aims to
consolidate existing research to investigate the role and
depth of adnexal structures in primary EMPD, and how they
correlate with tumor progression, recurrence rates, survival
rates, and overall patient prognosis.
Search Strategy:
The literature search methodology involved systematic
techniques utilizing targeted keywords across several
databases, including PubMed, Google Scholar, ProQuest,
ScienceDirect, and the university's linked library databases
such as ISI Web of Science. The search strategy
incorporated a blend of MeSH terms and keywords focusing
on extramammary Paget disease, Paget, adnexal
involvement, depth, recurrence, and prognosis by keeping in
view the study's objective.
Moreover, a manual search is performed for relevant
articles in the journal's bibliography list and included
studies. Unpublished studies/gray literature are manually
searched in Google Scholar and gray literature databases
using study keywords. This review follows PRISMA
(Preferred Reporting Items for Systematic Reviews and
Meta-analyses) guidelines.
B. Study Selection Process
The first step was identifying and retrieving articles
based on inclusion and exclusion criteria (shown in Figure
2).
Inclusion Criteria
Fig 2 PRISMA Flow Chart Showing the Selection of
Studies focused on primary extramammary Paget's Included Studies
disease (EMPD), including its diagnosis, pathogenesis,
treatment, and outcomes related to adnexal involvement III. RESULTS
and depth.
English-language publications were included to ensure The initial search identified a total of 289 citations, 94
comprehensive understanding and analysis. of which were duplicated. Total articles retrieved after
Studies reporting outcomes related to adnexal removing duplication is 195. The next step of the process
involvement and depth concerning recurrence rates, involved reading the abstracts in more detail and narrowing
prognosis, therapeutic approaches, and advancements in down the larger set of articles to those that specifically
EMPD management. addressed adnexal involvement in extramammary Paget
disease. Title and abstract screening of the remaining 195
citations resulted in the inclusion of 67 citations for further
review. After examination of full-text articles, 9 articles
were identified as being eligible.
IJISRT24APR2251 www.ijisrt.com 1180
Volume 9, Issue 4, April – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24APR2251
IV. DISCUSSION are distinguished by the expression of CK15 and CK19.
Both CK15 and CK19 are thought to be indicators of
Intraepidermal adenocarcinomas are the term used to derivation from follicular stem cells of the upper hair follicle
describe both extramammary and mammary Paget disease. and are expressed in trichogenic tumors. [17] A follicular
EMPD is more frequently a primary intraepidermal lesion origin of Paget cells is further supported by CK20 positivity
than mammary Paget's disease; only 20% of cases show in EPD without associated rectal carcinoma, as the hair
evidence of a dermal invasive component. [6] A disease is follicle stem cell niche is co-occupied by CK20+ Merkel
deemed minimally invasive if the invasive component is less cells and pluripotent neuroendocrine stem cells. [18]
than 1.0 mm in depth, and full excision is typically curative. Furthermore, Tanaka et al. found that HER2 overexpression
[7] An underlying cutaneous adnexal carcinoma, typically an and ERBB2 gene amplification did not differ between
apocrine adenocarcinoma, may also be linked to EMPD. Up primary lesions and lymph node (LN) metastasis in about
to 30% of cases indicate the spread of metastatic cancer 90% of EMPD patients, suggesting that HER2 targeting
from a regional visceral malignancy, such as rectal, cervical, therapies could be useful for treating both primary and
prostate, or transitional cell carcinoma. In these cases, the metastatic lesions. [19]
tumor cells show positive profiles for CK 7 and potentially
GCDFP-15, but they also exhibit immunohistochemical The relationship between adnexal involvement and
profiles that are similar to the original carcinoma, such as tumor progression has not been thoroughly studied, even
positive for prostate-specific antigen in prostate cancer or though it was a common finding in the Shaco-Levy et al.
CK 20 or CA19.9 in genitourinary or gastrointestinal report and did not impact the recurrence rate. In a study,
carcinomas. [8] Crude prevalence of EMPD in mainland comedone necrosis was found in 6 cases (11.3%) and
China was estimated to be 0.4 per 100,000 people in a recent adnexal involvement in 46 cases (86.7%). There was no
study by Yin et al. With the peak incidence at 66 years statistically significant difference in the percentage of cases
during first diagnosis, the majority of people are between 50 with adnexal involvement displaying a score of 2 between
and 80 years old. [9] invasive EMPD (77.8%) and in situ EMPD (57.7%). These
findings imply that comedon necrosis and the extent of
Ghazawi et al. report that the vulva in females and the adnexal involvement are not linked to the progression of
scrotum and penis in males are the primary sites of EMPD EMPD. [20] Preti et al. examined 122 patients with vulvar
development, though perianal, axillar, or umbilicus regions primary EMPD and found that, for intraepithelial and
may also occasionally be affected [10]. Multifocal EPMD is microinvasive (≤ 1 mm) vulvar primary EMPD, the cancer-
possible, and instances of double, triple, or synchronous specific survival at 120 months was 100%, while for
EMPD—EMPD that developed in more than two apocrine invasive (>1 mm) vulvar primary EMPD, it was 31%. [21]
gland-bearing areas—have also been documented. [11] Similar to this, van der Linden et al. examined 113 patients
There have also been cases reported where with vulvar primary EMPD and found that while the 5-year
hypopigmentation was the primary clinical presentation; disease-specific survival rate was only 50% and
these cases are challenging to diagnose as EMPD. [12] significantly worse in invasive primary EMPD, it was more
There may also be crust, scale, or erosion on the than 98% in noninvasive and micro-invasive EMPD. Thus,
erythematous lesions. These lesions can resemble several microinvasion might not have a major impact on EMPD
different skin conditions, including psoriasis, eczema, and patients' prognosis. [22]
fungal infections. Deep ulcers or nodules may appear in the
later stages. 10% of patients with EMPD are asymptomatic, In 1993, the Japanese Skin Cancer Society proposed a
despite the possibility of developing related symptoms like TNM staging system preliminary for primary EMPD. This
pruritus and tenderness. [13] The dermoscopic system classified the primary tumor category based on
characteristics of EMPD lesions have also been studied lymphovascular invasion depth, the lymph node category
recently. [14] Mun et al. compared the dermoscopic based on metastasis site (unilateral or bilateral inguinal
characteristics of EMPD lesions with those of other skin nodes), and the term "distant metastasis" was defined as
lesions, such as eczema, fungal infection, and Bowen metastasis in a lymph node that was outside of the regional
disease, the gross findings such as milky-red areas, dotted lymphatic basin or in a distant organ. This staging system
vessels, glomerular vessels, polymorphous vessels, surface was used in a cohort study by Hatta et al., who demonstrated
scales, and linear irregular vessels may be comparable to its usefulness with 76 patients. [23] Regarding the
EMPD. [15] prognostic factors associated with primary EMPD, Ito et al.
retrospectively analyzed 35 patients and found that the
Although the histogenesis of EPD is still unknown, degree of tumor invasion, lymph node metastases, clinically
several theories point to pluripotent epidermal stem cells, palpable lymph nodes, and the presence of a nodule on the
intraepidermal "Toker cells," apocrine glands, or both as primary lesion were significant prognostic factors. [24-26] A
possible sources. Mucin core proteins, androgen receptors, recent study found that while invasion level and perianal
Her-2 neu, gross cystic disease fluid protein-15, and location were not significantly associated with a worse
intermediate filaments of the cytokeratin (CK) type15— prognosis, tumor thickness, and lymphovascular invasion
specifically, CK7 and CK20—are all expressed by Paget were. In terms of node status, it was discovered that patients
cells. [16] Progeny from follicular stem cells can who had two or more node metastases fared worse in terms
differentiate into sebocytes, sweat glands, epidermis, and of survival than those who only had one. Metastatic lymph
hair follicle lineages. The bulge region's follicular stem cells
IJISRT24APR2251 www.ijisrt.com 1181
Volume 9, Issue 4, April – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24APR2251
node distribution on both sides did not significantly affect The 5-year overall survival rate for metastatic disease
prognosis. [5] is less than 10%. For these patients, there isn't yet a standard
systemic treatment plan. [37, 38] 5-FU and cisplatin (FP
According to conventional wisdom, Paget's disease is a therapy), 5-FU, epirubicin, carboplatin, vincristine, and
form of skin in-situ adenocarcinoma. Because EMPD mitomycin C (FECOM therapy), cisplatin, epirubicin, and
progresses slowly and typically affects only the epidermis paclitaxel (PET therapy), or combination S-1 (tegafur, 5-FU,
and cutaneous adnexal structures, most patients have a good and 5-chloro-2-4-dihydroxypyridine) and docetaxel, S-1
prognosis. [27] The adnexa may act as a conduit for monotherapy, or docetaxel monotherapy are among the
carcinoma to spread to deeper tissues where local available combination therapies. [39] Patients on FP and
therapeutic agents are less likely to be effective, as FECOM regimens have shown a median progression-free
evidenced by earlier case reports and case series. [28-30] survival of 5.2 months and 6.5 months, respectively, even
According to a study, adnexal involvement is a highly though the overall median survival is less than a year. [40]
prevalent feature in over 90% of cases of primary EMPD.
The most often affected anatomical structures by Paget cells Future directions in the field of primary EMPD with
are hair follicles and eccrine ducts. The most profound adnexal involvement hold immense promise for advancing
involvement in this investigation was 3.6 mm, and the diagnosis, treatment, and patient outcomes. One critical area
median for each adnexal structure was between 0.93 mm of focus is the development of targeted therapies that
(eccrine ducts) and 2.55 mm (eccrine secretory coils). [31] specifically address the mechanisms underlying adnexal
infiltration and disease progression. This includes
Future development of new local treatment modalities investigating molecular markers associated with adnexal
or planning of topical nonsurgical treatment should consider involvement, such as cell adhesion molecules, growth
this information. Imiquimod, 5-fluorouracil, and retinoic factors, and signaling pathways implicated in tumor cell
acid are currently used to treat primary EMPD to replace survival and proliferation within adnexal structures. By
more invasive, frequently disfiguring surgical methods. elucidating these molecular mechanisms, researchers can
Additional cutting-edge therapies under investigation identify potential therapeutic targets for novel drug
include photodynamic therapy, trastuzumab, either alone or development. In addition to molecular and
in conjunction with chemotherapy, and CO2 laser. [32, 33] microenvironmental studies, future diagnostic modalities
Although the aforementioned treatment modalities have should aim for greater precision in detecting adnexal
different mechanisms of action, understanding the depths of involvement in primary EMPD. Advanced imaging
tumor deposits and the depth of skin penetration are techniques, such as high-resolution MRI and molecular
undoubtedly crucial for designing an effective treatment imaging approaches, could enhance our ability to visualize
plan. While 5-fluorouracil is said to penetrate the skin to a tumor extent and accurately assess adnexal infiltration.
depth of 1-2 mm, we were unable to ascertain the potential Integration of imaging data with histopathological findings
depth of imiquimod's skin penetration based on our review and biomarker analysis may enable more personalized
of the literature. [34] treatment strategies tailored to individual patients based on
the degree of adnexal involvement and disease
The principal therapeutic approach entails a broad local aggressiveness.
surgical excision of the affected area. In comparison to the
standard treatment (wide local excision), Mohs V. CONCLUSION
micrographic surgery resulted in an over 10-fold reduction
in the risk of positive margins. [35] A study by Long et al. The prognosis and recurrence of primary EMPD are
with 154 cases of EMPD found that females were more closely linked with the extent of adnexal involvement. Over
likely than males to have a positive margin. They also 90% of primary EMPD cases exhibit adnexal involvement,
concluded that patients with positive pathologic margins had predominantly in hair follicles and eccrine ducts. Although
a 3.5-fold higher chance of recurrence than patients with this involvement has not been definitively linked to tumor
negative margins. [36] A study conducted between 1998 and progression or higher recurrence rates, it plays a crucial role
2012 by Fujisawa et al. with 151 patients examined the by potentially facilitating deeper tissue infiltration, thus
function of sentinel lymph node biopsy in EMPD. 107 highlighting its clinical importance.
patients in this cohort did not exhibit any clinically
noticeable lymphadenopathy, and all of them had sentinel Therapeutic options for primary EMPD range from
biopsies performed. Finally, it was discovered that 15% of topical treatments like imiquimod and 5-fluorouracil to
these clinically negative patients had lymph node surgical excision. Among surgical methods, Mohs
metastases. This was linked to the primary specimen's micrographic surgery is preferred for its enhanced margin
lymphovascular and deeper levels of invasion. This indicates control. The efficacy of topical agents depends significantly
that, in the absence of clinically noticeable on the depth of Paget cell invasion within these adnexal
lymphadenopathy, patients with invasive disease should structures, illustrating the need to thoroughly understand the
seek sentinel lymph node biopsy. Hence, patients with early- pattern and extent of this invasion to optimize patient
stage lymph node metastases may have a better prognosis if management strategies.
they receive early detection and lymph node dissection. [5]
IJISRT24APR2251 www.ijisrt.com 1182
Volume 9, Issue 4, April – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24APR2251
Given these insights, it is essential to refine current [11]. Zhang, Z., et al., Cutaneous metastases from triple
diagnostic and treatment protocols to better address the primary extramammary Paget's disease. Journal der
intricacies of adnexal proliferation in primary EMPD. Deutschen Dermatologischen Gesellschaft= Journal
of the German Society of Dermatology: JDDG, 2020.
Conflict of Interest Statement 18(10): p. 1169-1172.
The authors have no conflicts of interest to declare. [12]. Iwamoto, K., et al., Depigmented extramammary
Paget's disease without histological dermal invasion
Funding Sources identified by multiple inguinal and pelvic lymph
This study was not supported by any sponsor or funder. node metastases. European Journal of Dermatology,
2018. 28(3): p. 387-388.
Author Contributions [13]. St Claire, K., et al., Extramammary paget disease.
All authors have participated sufficiently in the Dermatology online journal, 2019. 25(4).
intellectual content, conception, and design of this study. All [14]. Payapvipapong, K., A. Nakakes, and M. Tanaka,
authors agree to be accountable for all aspects of the Lava lake structure and cloud-like structureless area:
manuscript. new clues for diagnosing extramammary Paget
REFERENCES disease. Journal of the European Academy of
Dermatology and Venereology, 2017. 31(10): p.
[1]. Shaco-Levy, R., et al., Paget disease of the vulva: a e459-e461.
study of 56 cases. Eur J Obstet Gynecol Reprod Biol, [15]. Mun, J.H., et al., Clinical and dermoscopic
2010. 149(1): p. 86-91. characteristics of extramammary Paget disease: a
[2]. Crocker, H.R., Paget's disease affecting the scrotum study of 35 cases. British Journal of Dermatology,
and penis. Trans Pathol Soc Lond, 1889. 40: p. 187- 2016. 174(5): p. 1104-1107.
191. [16]. Regauer, S., Extramammary Paget's disease—a
[3]. Moretto, P., et al., Management of Penoscrotal proliferation of adnexal origin? Histopathology,
Extramammary Paget Disease: Case Series and 2006. 48(6): p. 723-729.
Review of the Literature. Current Oncology, 2013. [17]. Blanpain, C., et al., Self-renewal, multipotency, and
20(4): p. 311-320. the existence of two cell populations within an
[4]. Scarbrough, C.A., A. Vrable, and D.R. Carr, epithelial stem cell niche. Cell, 2004. 118(5): p. 635-
Definition, association with malignancy, biologic 648.
behavior, and treatment of ectopic extramammary [18]. Sieber‐Blum, M. and M. Grim, The adult hair
Paget’s disease: A review of the literature. The follicle: cradle for pluripotent neural crest stem cells.
Journal of clinical and aesthetic dermatology, 2019. Birth Defects Research Part C: Embryo Today:
12(8): p. 40. Reviews, 2004. 72(2): p. 162-172.
[5]. Ohara, K., et al., A proposal for a TNM staging [19]. Tanaka, R., et al., Concordance of the HER2 protein
system for extramammary Paget disease: and gene status between primary and corresponding
retrospective analysis of 301 patients with invasive lymph node metastatic sites of extramammary Paget
primary tumors. Journal of dermatological science, disease. Clinical & experimental metastasis, 2016.
2016. 83(3): p. 234-239. 33: p. 687-697.
[6]. Abbott, J.J. and I. Ahmed, Adenocarcinoma of [20]. Shiomi, T., et al., Extramammary Paget’s disease:
mammary-like glands of the vulva: report of a case evaluation of the adnexal status of 53 cases. Polish
and review of the literature. The American journal of Journal of Pathology, 2015. 66(2): p. 121-126.
dermatopathology, 2006. 28(2): p. 127-133. [21]. Preti, M., et al., Vulvar Paget's disease and stromal
[7]. Liegl, B., L.-C. Horn, and F. Moinfar, Androgen invasion: clinico-pathological features and survival
receptors are frequently expressed in mammary and outcomes. Surgical Oncology, 2021. 38: p. 101581.
extramammary Paget's disease. Modern pathology, [22]. van der Linden, M., et al., Vulvar Paget disease: a
2005. 18(10): p. 1283-1288. national retrospective cohort study. Journal of the
[8]. Obaidat, N.A., K.O. Alsaad, and D. Ghazarian, Skin American Academy of Dermatology, 2019. 81(4): p.
adnexal neoplasms—part 2: an approach to tumours 956-962.
of cutaneous sweat glands. Journal of Clinical [23]. Hatta, N., et al., Extramammary Paget’s disease:
Pathology, 2007. 60(2): p. 145-159. treatment, prognostic factors and outcome in 76
[9]. Yin, S., et al., Prevalence of extramammary Paget's patients. Br J Dermatol, 2008. 158(2): p. 313-318.
disease in urban China: a population-based study. [24]. Dai, B., et al., Primary invasive carcinoma associated
Orphanet J Rare Dis, 2021. 16(1): p. 1-7. with penoscrotal extramammary P aget's disease: a
[10]. Ghazawi, F.M., et al., Demographic and clinical clinicopathological analysis of 56 cases. BJU
characteristics of extramammary Paget's disease international, 2015. 115(1): p. 153-160.
patients in Japan from 2000 to 2019. Journal of the [25]. Ito, T., et al., Tumor thickness as a prognostic factor
European Academy of Dermatology and in extramammary Paget's disease. The Journal of
Venereology, 2021. 35(2): p. e133-e135. Dermatology, 2015. 42(3): p. 269-275.
[26]. Ito, T., Y. Kaku-Ito, and M. Furue, The diagnosis and
management of extramammary Paget’s disease.
Expert Rev Anticancer Ther, 2018. 18(6): p. 543-553.
IJISRT24APR2251 www.ijisrt.com 1183
Volume 9, Issue 4, April – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24APR2251
[27]. Zhao, Y., et al., Primary extramammary Paget’s
disease: a clinicopathological study of 28 cases. Int J
Clin Exp Pathol, 2019. 12(9): p. 3426.
[28]. Belousova, I.E., et al., Vulvar toker cells: the long-
awaited missing link: a proposal for an origin-based
histogenetic classification of extramammary paget
disease. The American journal of dermatopathology,
2006. 28(1): p. 84-86.
[29]. Goldblum, J.R. and W.R. Hart, Vulvar Paget's
disease: a clinicopathologic and
immunohistochemical study of 19 cases. The
American journal of surgical pathology, 1997.
21(10): p. 1178-1187.
[30]. Hart, W.R. and J.B. Millman, Progression of
intraepithelial Paget's disease of the vulva to invasive
carcinoma. Cancer, 1977. 40(5): p. 2333-2337.
[31]. Konstantinova, A.M., et al., Depth and patterns of
adnexal involvement in primary extramammary
(anogenital) Paget disease: a study of 178 lesions
from 146 patients. Am J Dermatopathol, 2016.
38(11): p. 802-808.
[32]. Karam, A., et al., HER-2/neu targeting for recurrent
vulvar Paget's disease: a case report and literature
review. Gynecologic oncology, 2008. 111(3): p. 568-
571.
[33]. Takahagi, S., et al., Metastatic extramammary
Paget’s disease treated with paclitaxel and
trastuzumab combination chemotherapy. The Journal
of dermatology, 2009. 36(8): p. 457-461.
[34]. Delport, E.S., Extramammary Paget's disease of the
vulva: an annotated review of the current literature.
Australasian Journal of Dermatology, 2013. 54(1): p.
9-21.
[35]. Wollina, U., et al., Surgical treatment for
extramammary Paget’s disease. Current treatment
options in oncology, 2018. 19: p. 1-12.
[36]. Long, B., et al., A matter of margins: Surgical and
pathologic risk factors for recurrence in
extramammary Paget's disease. Gynecologic
oncology, 2017. 147(2): p. 358-363.
[37]. Nabavizadeh, R., et al., Extramammary Paget's
disease: Updates in the workup and management.
Asian Journal of Urology, 2022. 9(4): p. 451-459.
[38]. Oashi, K., et al., Combination chemotherapy for
metastatic extramammary Paget disease. British
Journal of Dermatology, 2014. 170(6): p. 1354-1357.
[39]. Tanese, K., et al., Updates on the systemic treatment
of advanced non-melanoma skin cancer. Frontiers in
medicine, 2019. 6: p. 160.
[40]. Tokuda, Y., F. Arakura, and H. Uhara, Combination
chemotherapy of low-dose 5-fluorouracil and
cisplatin for advanced extramammary Paget’s
disease. International journal of clinical oncology,
2015. 20: p. 194-197.
IJISRT24APR2251 www.ijisrt.com 1184
You might also like
- Cutaneous Candidiasis - An Evidence-Based Review of Topical and Systemic Treatments To Inform Clinical PracticeDocument11 pagesCutaneous Candidiasis - An Evidence-Based Review of Topical and Systemic Treatments To Inform Clinical PracticeRose ParkNo ratings yet
- Research Microneedling in DermatologyDocument10 pagesResearch Microneedling in DermatologyErik BrooksNo ratings yet
- Maldonado 20 Et 20 AlDocument6 pagesMaldonado 20 Et 20 AlAzuhra AnnisaNo ratings yet
- Patofisiologia de Sinutis OdontogenicaDocument7 pagesPatofisiologia de Sinutis OdontogenicaDaniel Alejandro Flores Gutierrez.No ratings yet
- Keratitis Por Adenovirus 2018Document8 pagesKeratitis Por Adenovirus 2018pachisfmbNo ratings yet
- JIAMSE 19-2s LIMSCDocument167 pagesJIAMSE 19-2s LIMSCHafriliantika RamadhaniNo ratings yet
- Skin Disease Classification Using Hybrid ApproachDocument4 pagesSkin Disease Classification Using Hybrid ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Simple Approach To Histological Diagnosis of Common Skin Adnexal TumorsDocument11 pagesSimple Approach To Histological Diagnosis of Common Skin Adnexal TumorsThiều Mạnh CườngNo ratings yet
- A Diagnostic Software Tool For Skin Diseases With Basic and Weighted K-NNDocument4 pagesA Diagnostic Software Tool For Skin Diseases With Basic and Weighted K-NNkrlitoxNo ratings yet
- Cancers 14 00476Document25 pagesCancers 14 00476Christine OlivarNo ratings yet
- Inglés 2018Document7 pagesInglés 2018Luis GuzmánNo ratings yet
- Effectiveness of Oral Albendazole As A Treatment For Pediculosis CapitisDocument8 pagesEffectiveness of Oral Albendazole As A Treatment For Pediculosis CapitisFlorensia WodaNo ratings yet
- Intervention Development in Occupational ResearchDocument7 pagesIntervention Development in Occupational ResearchAllisa DzakwanNo ratings yet
- Foresta 2014Document14 pagesForesta 2014stoia_sebiNo ratings yet
- Erythema Dyschromicum Perstans A Case Report 2376 0427 1000266Document3 pagesErythema Dyschromicum Perstans A Case Report 2376 0427 1000266Batra MourinhoNo ratings yet
- The Management of Sinonasal Inverted Papilloma: Our ExperienceDocument7 pagesThe Management of Sinonasal Inverted Papilloma: Our Experiencesri ayu lestari wulandariNo ratings yet
- Fmed 09 835843Document20 pagesFmed 09 835843juan uribeNo ratings yet
- Simple Approach To Histological Diagnosis of Skin Adnexal Tumors PDFDocument11 pagesSimple Approach To Histological Diagnosis of Skin Adnexal Tumors PDFElmer MoralesNo ratings yet
- Diagnostic Procedures in OphthalmologyDocument21 pagesDiagnostic Procedures in OphthalmologyRajit Singh PalNo ratings yet
- Antrocoanal THTDocument6 pagesAntrocoanal THTNIGHTCORE NATIONNo ratings yet
- Normal Variants in Patients Consulted in The Dermatology Clinic For Lesions of The Male External GenitaliaDocument5 pagesNormal Variants in Patients Consulted in The Dermatology Clinic For Lesions of The Male External GenitaliaId BaNo ratings yet
- Jurnal RooDocument8 pagesJurnal RooPradistya Syifa YudiasariNo ratings yet
- Complications and Management After A Nonsurgical Rhinoplasty - A Literature ReviewDocument8 pagesComplications and Management After A Nonsurgical Rhinoplasty - A Literature ReviewKerlida SantosNo ratings yet
- Examining A Case: Carbamazepine-Triggered Drug Reaction With Eosinophilia and Systemic SymptomsDocument2 pagesExamining A Case: Carbamazepine-Triggered Drug Reaction With Eosinophilia and Systemic SymptomsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- S Under The MicroscopeDocument41 pagesS Under The MicroscopeBruno SarmentoNo ratings yet
- Chiniforush2016 PDT PDFDocument10 pagesChiniforush2016 PDT PDFShriya ShahuNo ratings yet
- EuropeanpaperDocument11 pagesEuropeanpaperMostafa EidNo ratings yet
- Application For Iec NriasDocument15 pagesApplication For Iec NriasPavan Kumar TripuraneniNo ratings yet
- CystDocument1 pageCystAhmadBuldaniNo ratings yet
- Review: Tinea Corporis: An Updated ReviewDocument22 pagesReview: Tinea Corporis: An Updated ReviewMade SetiadjiNo ratings yet
- Targeted Drug Delivery DissertationDocument4 pagesTargeted Drug Delivery DissertationPaperWriterOnlineUK100% (1)
- ECD Vs Sup Parotidectomy ArticleDocument8 pagesECD Vs Sup Parotidectomy ArticleAmeena AzeemiNo ratings yet
- Topic Treatment Acne Scars1Document3 pagesTopic Treatment Acne Scars1Stanca NicolaeNo ratings yet
- Dermal Fillers For Tear Trough Rejuvenation: A Systematic ReviewDocument12 pagesDermal Fillers For Tear Trough Rejuvenation: A Systematic ReviewPoramate PITAK-ARNNOPNo ratings yet
- Diagnostic Use of Facial Image Analysis Software in Endocrine and Genetic Disorders: Review, Current Results and Future PerspectivesDocument6 pagesDiagnostic Use of Facial Image Analysis Software in Endocrine and Genetic Disorders: Review, Current Results and Future PerspectivesRavi KiranNo ratings yet
- Ijerph 19 00801Document9 pagesIjerph 19 00801satriaNo ratings yet
- Decrease in Visual Acuity As The Ini.3tial Clinical Presentation of Lung Adenocarcinoma A Case ReportDocument6 pagesDecrease in Visual Acuity As The Ini.3tial Clinical Presentation of Lung Adenocarcinoma A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Augustin 2011Document9 pagesAugustin 2011Trustia RizqandaruNo ratings yet
- Sclerotherapy For Lymphatic Malformations in Children: A Scoping ReviewDocument11 pagesSclerotherapy For Lymphatic Malformations in Children: A Scoping ReviewHung Thuyen PhamNo ratings yet
- An Institutional Study On Covid-19 Associated Rhino-Orbital-Cerebral MucormycosisDocument8 pagesAn Institutional Study On Covid-19 Associated Rhino-Orbital-Cerebral MucormycosisIJAR JOURNALNo ratings yet
- 2023 A Practical Review of The ManagementDocument8 pages2023 A Practical Review of The ManagementHong HuynhNo ratings yet
- Microneedling Tratamiento en CicatricesDocument7 pagesMicroneedling Tratamiento en CicatricesRocio VinderolaNo ratings yet
- JCM 11 04974 v2Document20 pagesJCM 11 04974 v2Javier MartinNo ratings yet
- Overview of Ultrasound Imaging Applications in DermatologyDocument9 pagesOverview of Ultrasound Imaging Applications in DermatologyLeonardo PiberNo ratings yet
- Applsci 11 11181Document15 pagesApplsci 11 11181dNo ratings yet
- Immunopathology SepsisDocument2 pagesImmunopathology SepsisJavier LugoNo ratings yet
- Allergy - 2019 - Ivanova - What Did We Learn From Multiple Omics Studies in AsthmaDocument17 pagesAllergy - 2019 - Ivanova - What Did We Learn From Multiple Omics Studies in Asthmanhc_king_proNo ratings yet
- Klasifikasi Rhinitis KronisDocument9 pagesKlasifikasi Rhinitis Kronisfasa bihamdiNo ratings yet
- FullDocument20 pagesFulledith calderonNo ratings yet
- Ref 1Document5 pagesRef 1Nanda SapitriNo ratings yet
- Case Studies in Occupational Epidemiology 230913 012907Document219 pagesCase Studies in Occupational Epidemiology 230913 012907karlanatalbertNo ratings yet
- PanaceaJMedSci 11 2 289 296Document8 pagesPanaceaJMedSci 11 2 289 296Jenerio PanggabeanNo ratings yet
- Dermatopathology - Classification of Cutaneous Lesions (E Zappi)Document219 pagesDermatopathology - Classification of Cutaneous Lesions (E Zappi)Denisa VladulescuNo ratings yet
- Skin ManifestationsDocument7 pagesSkin ManifestationsyuliNo ratings yet
- Ccid 11 175Document11 pagesCcid 11 175Remo Alnovryanda PutraNo ratings yet
- Slide Eritroderma 2Document7 pagesSlide Eritroderma 2Anonymous QqGJk2jK5No ratings yet
- Ectopic Thyroid Carcinoma in The Nasal S 2024 International Journal of SurgeDocument4 pagesEctopic Thyroid Carcinoma in The Nasal S 2024 International Journal of SurgeRonald QuezadaNo ratings yet
- Research Paper Skin CancerDocument7 pagesResearch Paper Skin Cancersuw1vadibys2100% (1)
- Ccid 12 911Document7 pagesCcid 12 911Imanuel CristiantoNo ratings yet
- Detection of Phishing WebsitesDocument6 pagesDetection of Phishing WebsitesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vertical Farming System Based on IoTDocument6 pagesVertical Farming System Based on IoTInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Detection and Counting of Fake Currency & Genuine Currency Using Image ProcessingDocument6 pagesDetection and Counting of Fake Currency & Genuine Currency Using Image ProcessingInternational Journal of Innovative Science and Research Technology100% (9)
- Osho Dynamic Meditation; Improved Stress Reduction in Farmer Determine by using Serum Cortisol and EEG (A Qualitative Study Review)Document8 pagesOsho Dynamic Meditation; Improved Stress Reduction in Farmer Determine by using Serum Cortisol and EEG (A Qualitative Study Review)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Influence of Principals’ Promotion of Professional Development of Teachers on Learners’ Academic Performance in Kenya Certificate of Secondary Education in Kisii County, KenyaDocument13 pagesInfluence of Principals’ Promotion of Professional Development of Teachers on Learners’ Academic Performance in Kenya Certificate of Secondary Education in Kisii County, KenyaInternational Journal of Innovative Science and Research Technology100% (1)
- The Impact of Music on Orchid plants Growth in Polyhouse EnvironmentsDocument5 pagesThe Impact of Music on Orchid plants Growth in Polyhouse EnvironmentsInternational Journal of Innovative Science and Research Technology100% (1)
- Consistent Robust Analytical Approach for Outlier Detection in Multivariate Data using Isolation Forest and Local Outlier FactorDocument5 pagesConsistent Robust Analytical Approach for Outlier Detection in Multivariate Data using Isolation Forest and Local Outlier FactorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Realigning Curriculum to Simplify the Challenges of Multi-Graded Teaching in Government Schools of KarnatakaDocument5 pagesRealigning Curriculum to Simplify the Challenges of Multi-Graded Teaching in Government Schools of KarnatakaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sustainable Energy Consumption Analysis through Data Driven InsightsDocument16 pagesSustainable Energy Consumption Analysis through Data Driven InsightsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Entrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisDocument10 pagesEntrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Overview of Lung CancerDocument6 pagesAn Overview of Lung CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Digital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaDocument10 pagesDigital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaDocument6 pagesImpact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Utilization of Waste Heat Emitted by the KilnDocument2 pagesUtilization of Waste Heat Emitted by the KilnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Efficient Cloud-Powered Bidding MarketplaceDocument5 pagesAn Efficient Cloud-Powered Bidding MarketplaceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Designing Cost-Effective SMS based Irrigation System using GSM ModuleDocument8 pagesDesigning Cost-Effective SMS based Irrigation System using GSM ModuleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictDocument13 pagesEffect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predictive Analytics for Motorcycle Theft Detection and RecoveryDocument5 pagesPredictive Analytics for Motorcycle Theft Detection and RecoveryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Tix: Automated Bus Ticket SolutionDocument5 pagesAuto Tix: Automated Bus Ticket SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Examining the Benefits and Drawbacks of the Sand Dam Construction in Cadadley RiverbedDocument8 pagesExamining the Benefits and Drawbacks of the Sand Dam Construction in Cadadley RiverbedInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ambulance Booking SystemDocument7 pagesAmbulance Booking SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparative Evaluation of Action of RISA and Sodium Hypochlorite on the Surface Roughness of Heat Treated Single Files, Hyflex EDM and One Curve- An Atomic Force Microscopic StudyDocument5 pagesComparative Evaluation of Action of RISA and Sodium Hypochlorite on the Surface Roughness of Heat Treated Single Files, Hyflex EDM and One Curve- An Atomic Force Microscopic StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Computer Vision Gestures Recognition System Using Centralized Cloud ServerDocument9 pagesComputer Vision Gestures Recognition System Using Centralized Cloud ServerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Forensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsDocument12 pagesForensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Textbook of Respiratory Disease in Dogs and Cats Diaphragmatic HerniaDocument9 pagesTextbook of Respiratory Disease in Dogs and Cats Diaphragmatic HerniaDiego CushicóndorNo ratings yet
- (Loga.vn) Tiếng Anh 10 (Sách Nâng Cao) - Đề Thi Chọn HSGDocument6 pages(Loga.vn) Tiếng Anh 10 (Sách Nâng Cao) - Đề Thi Chọn HSGdonhan91No ratings yet
- Encyclopedia of Urban Cultures Cities and Cultures Around The World, Volume 2 (Melvin Ember Carol R. Ember)Document536 pagesEncyclopedia of Urban Cultures Cities and Cultures Around The World, Volume 2 (Melvin Ember Carol R. Ember)Lelissa KelbesaNo ratings yet
- TXDVXX 12Document7 pagesTXDVXX 12Pedro RochaNo ratings yet
- Camera Mouse ManualDocument23 pagesCamera Mouse ManualJoe Lassie El-KhouriNo ratings yet
- Market Analysis and Sales Development of AmulDocument19 pagesMarket Analysis and Sales Development of AmulPrabhakar ManoharanNo ratings yet
- (TP) Chapter 10 - Sound in DuctsDocument9 pages(TP) Chapter 10 - Sound in Ductsagung_123123No ratings yet
- 5990 8296enDocument4 pages5990 8296enGiriraj T KulkarniNo ratings yet
- Fundamentals of AccountingDocument2 pagesFundamentals of AccountingDiane SorianoNo ratings yet
- DPP Engine Room Log Book Page#1Document1 pageDPP Engine Room Log Book Page#1Muhammad Suleman FaizNo ratings yet
- The Role of Co-Creation Experience in Engaging Customers With Service BrandsDocument16 pagesThe Role of Co-Creation Experience in Engaging Customers With Service BrandsEdy Yulianto PutraNo ratings yet
- Industrial Boiler Project Final ReportDocument34 pagesIndustrial Boiler Project Final Reportvanshita7020No ratings yet
- Compressed Natural Gas - WikipediaDocument1 pageCompressed Natural Gas - WikipediaEkampreet KaurNo ratings yet
- Fm-npd-16 (Temp. Change Request Note)Document1 pageFm-npd-16 (Temp. Change Request Note)akash.vd.1603No ratings yet
- Electromagnetic Wave Propagation: A. Wave in Scalar FormDocument18 pagesElectromagnetic Wave Propagation: A. Wave in Scalar FormEWUNETU TEKEBANo ratings yet
- Heating Cable Selection GuideDocument4 pagesHeating Cable Selection Guidehassan3012No ratings yet
- Fib Congress Freyssinet by ShushkewichDocument28 pagesFib Congress Freyssinet by ShushkewichpablokrahlNo ratings yet
- Series QCT and QCB Cylinders With Integrated Guide: Double-Acting, Magnetic Piston, Guided Ø 20, 25, 32, 40, 50, 63 MMDocument5 pagesSeries QCT and QCB Cylinders With Integrated Guide: Double-Acting, Magnetic Piston, Guided Ø 20, 25, 32, 40, 50, 63 MMVanesaNo ratings yet
- SSTMZG528: Assignment 1Document4 pagesSSTMZG528: Assignment 1D V BHASKARNo ratings yet
- SS ZG653 (RL1.2) : Software Architecture: BITS PilaniDocument12 pagesSS ZG653 (RL1.2) : Software Architecture: BITS PilaniAditya AggarwalNo ratings yet
- ResumeatbapujiDocument2 pagesResumeatbapujiEllur AnandNo ratings yet
- Ethical Theories and Social WorkDocument12 pagesEthical Theories and Social Workbonny70% (1)
- ReadMe WinDocument4 pagesReadMe WinpundaiNo ratings yet
- Coop Conference Proceeding (21-22aug 2022)Document585 pagesCoop Conference Proceeding (21-22aug 2022)oliviahuda75No ratings yet
- Paper Wilke and ChangDocument7 pagesPaper Wilke and ChangMaría Angélica Garcia Giraldo100% (1)
- MerkabahDocument8 pagesMerkabahbrozacaNo ratings yet
- Second Law Part 2Document10 pagesSecond Law Part 2Sivan RajNo ratings yet
- Composite Member EI ValueDocument4 pagesComposite Member EI ValueArjun RajaNo ratings yet
- Xerox Wc423 SMDocument600 pagesXerox Wc423 SMkerintNo ratings yet
- Audit Programe - InventoryDocument3 pagesAudit Programe - InventoryAnnete Utomo HutabaratNo ratings yet