You might also like
- Cancer ImmunologyDocument37 pagesCancer ImmunologyBeenish SarfrazNo ratings yet
- 9.lecturer 18 Biochemistry Effect On Tumor and Tumor MarkersDocument19 pages9.lecturer 18 Biochemistry Effect On Tumor and Tumor MarkersAbdulRahman MuthannaNo ratings yet
- Biology Investigatory Project: Study On CancerDocument24 pagesBiology Investigatory Project: Study On CancerAthiya Zainab100% (1)
- Blood Vessels Vasculogenesis Endothelial Mesoderm Embryo: Angiogenesis Is The Physiological Process Through Which NewDocument23 pagesBlood Vessels Vasculogenesis Endothelial Mesoderm Embryo: Angiogenesis Is The Physiological Process Through Which NewDaniel SutantoNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument8 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Neoplasia S. M Jawwad AliDocument25 pagesNeoplasia S. M Jawwad AliAnt EverafterNo ratings yet
- An Introduction To Cancer Biology: When Good Cells Go BadDocument68 pagesAn Introduction To Cancer Biology: When Good Cells Go BadSavitaNo ratings yet
- Introduction To OncologyDocument58 pagesIntroduction To OncologyserviceNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument8 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Conchem q4 Module 3 Week 5-6Document8 pagesConchem q4 Module 3 Week 5-6Tiffany Moore100% (2)
- Cancer and Malignant GrowthDocument3 pagesCancer and Malignant GrowthTapan Kumar PalNo ratings yet
- Cancer (Medical Term:Malignant NeoplasmDocument7 pagesCancer (Medical Term:Malignant NeoplasmolussojiNo ratings yet
- Cancer CareDocument84 pagesCancer Careakoeljames8543No ratings yet
- Chapter 16-JnuCancer - 複本Document42 pagesChapter 16-JnuCancer - 複本Wai Kwong ChiuNo ratings yet
- Investigatory Project On CANCERDocument15 pagesInvestigatory Project On CANCERSreeja SwainNo ratings yet
- Prepared By: Anna Marie M. Montalban, RN, Us-RnDocument71 pagesPrepared By: Anna Marie M. Montalban, RN, Us-RnPrecai Permangil100% (2)
- Cellular AberrationDocument71 pagesCellular AberrationKris TejereroNo ratings yet
- 13 ChemoDocument40 pages13 ChemoSweet SunNo ratings yet
- Jurnal NeoplasmaDocument10 pagesJurnal NeoplasmaFadhilah Asyifa DewantiNo ratings yet
- Neoplastic DisordersDocument36 pagesNeoplastic DisordersJSeasharkNo ratings yet
- L11, Pathophysiology ManualDocument11 pagesL11, Pathophysiology Manualph.mt.pharmaNo ratings yet
- 3 CancerDocument47 pages3 Cancerkirubel getyeNo ratings yet
- Cc2 - MidtermDocument3 pagesCc2 - MidtermMika SusadaNo ratings yet
- Cancer DevelopmentDocument4 pagesCancer DevelopmenterinNo ratings yet
- Cellular AberrationDocument58 pagesCellular AberrationTauqeer AhmedNo ratings yet
- Unco Ntrolled Proliferation: Distinguishing Property of Malignant Cells. Without Intervention, Cancerous Tissues Grow inDocument7 pagesUnco Ntrolled Proliferation: Distinguishing Property of Malignant Cells. Without Intervention, Cancerous Tissues Grow inYukiNo ratings yet
- G Path-NeoplasiaDocument60 pagesG Path-Neoplasiachouchou124No ratings yet
- Oncology NursingDocument7 pagesOncology NursingDiana Laura Lei100% (1)
- CancerDocument19 pagesCancerparabharshita2709No ratings yet
- Cancer: Large Group of DiseasesDocument141 pagesCancer: Large Group of Diseasesmynoidanh19No ratings yet
- Anti Neoplastic AgentsDocument116 pagesAnti Neoplastic AgentsAbii KetiNo ratings yet
- 4th Lecture (NCM106 CA I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDocument14 pages4th Lecture (NCM106 CA I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (3)
- Mohammad Altamimi, MD, PHD Jordan UniversityDocument16 pagesMohammad Altamimi, MD, PHD Jordan UniversityDaniel AtiehNo ratings yet
- Mohammad Altamimi, MD, PHD Jordan UniversityDocument16 pagesMohammad Altamimi, MD, PHD Jordan UniversityDaniel AtiehNo ratings yet
- CANCERDocument84 pagesCANCERhydrocodoonieNo ratings yet
- Nursing Care of The Client With CancerDocument15 pagesNursing Care of The Client With CancerAlvin M Alcayno0% (1)
- Topics: Nasopharyngeal CarcinomaDocument21 pagesTopics: Nasopharyngeal CarcinomaShruthi Y nursingNo ratings yet
- Lewis: Medical-Surgical Nursing, 9 Edition: CancerDocument8 pagesLewis: Medical-Surgical Nursing, 9 Edition: CancerPrincess AgarwalNo ratings yet
- Thursday, 3 November 2022 10:14 PMDocument5 pagesThursday, 3 November 2022 10:14 PMAdiel CalsaNo ratings yet
- Cancer" Is The Latin Word For Crab.: Normal Mechanism of Body GrowthDocument9 pagesCancer" Is The Latin Word For Crab.: Normal Mechanism of Body Growthanupriya mittalhy6No ratings yet
- Immuno TherapyDocument20 pagesImmuno TherapyAttis PhrygiaNo ratings yet
- Tumour Immunology: Von Ryan F. Lingcallo, RMTDocument20 pagesTumour Immunology: Von Ryan F. Lingcallo, RMTJuan SalenNo ratings yet
- Neoplasia Summer 2020Document38 pagesNeoplasia Summer 2020Sharif HossainNo ratings yet
- Neoplasia Stom Eng 2011Document58 pagesNeoplasia Stom Eng 2011Artem GrigoryanNo ratings yet
- Oncologic Nursing: Oncology: OverviewDocument156 pagesOncologic Nursing: Oncology: OverviewNathalie KerrNo ratings yet
- MR 28 Agustus-1Document7 pagesMR 28 Agustus-1BramaNo ratings yet
- Invasion of ECM Degradation of ECMDocument8 pagesInvasion of ECM Degradation of ECMJezreel NicolasNo ratings yet
- Ursing Care of Client With CancerDocument51 pagesUrsing Care of Client With CancerJimmelyn PalosNo ratings yet
- Oncology: Ivano-Frankivsk National Medical University Department of OncologyDocument41 pagesOncology: Ivano-Frankivsk National Medical University Department of OncologyAli Baker AlgelaneNo ratings yet
- Module 3.1. Intro To Cellular Aberration and PathophysiologyDocument15 pagesModule 3.1. Intro To Cellular Aberration and PathophysiologyShiena Mae PelagioNo ratings yet
- FranciscoDocument4 pagesFranciscoFrances FranciscoNo ratings yet
- Management of Patient With CancerDocument47 pagesManagement of Patient With Canceruuuhbnb lplhghNo ratings yet
- Cancer OverviewDocument13 pagesCancer OverviewDevansh MoyalNo ratings yet
- JSCR 18 013Document7 pagesJSCR 18 013Mary ChikamaraNo ratings yet
- Tumor Immunology: ObjectivesDocument20 pagesTumor Immunology: ObjectivesMarl EstradaNo ratings yet
- CancerBooklest FinalDocument15 pagesCancerBooklest Finalrafael alvarizNo ratings yet
- NE0PLASIADocument28 pagesNE0PLASIADaniel SutantoNo ratings yet
- Cancer ResearchDocument5 pagesCancer ResearchmelanieNo ratings yet
- Tumor Immunology: M. Nagarkatti Teaching ObjectivesDocument4 pagesTumor Immunology: M. Nagarkatti Teaching Objectives99manu99No ratings yet
- Forefoot Myopericytoma: A Case Reportand Review of The LiteratureDocument4 pagesForefoot Myopericytoma: A Case Reportand Review of The LiteratureIJAR JOURNALNo ratings yet
- Koagulasi Intravaskuler Diseminata Pada Kanker: January 2015Document13 pagesKoagulasi Intravaskuler Diseminata Pada Kanker: January 2015Zinnan Al-FaqihNo ratings yet
- Cancer Cell and Cell CycleDocument10 pagesCancer Cell and Cell CycleRouie AzucenaNo ratings yet
- Radiation Dose and Image Quality BT DBT and FFDMDocument6 pagesRadiation Dose and Image Quality BT DBT and FFDMRenadNo ratings yet
- 1 Introduction To Economic EvaluationDocument31 pages1 Introduction To Economic EvaluationSwayam MohapatraNo ratings yet
- Diet and CancerDocument7 pagesDiet and CanceraibutyNo ratings yet
- BreastQ-bank Full - 2Document44 pagesBreastQ-bank Full - 2Helene AlawamiNo ratings yet
- Female Genital Tract Cytopathology: PracticalDocument26 pagesFemale Genital Tract Cytopathology: PracticalNgotelo FunwiNo ratings yet
- CT Simulation MethodologyDocument41 pagesCT Simulation MethodologyRohla habibiNo ratings yet
- Bernhardt 2020Document6 pagesBernhardt 2020ghanaNo ratings yet
- Lymph Nodes Normal and MalignantDocument12 pagesLymph Nodes Normal and MalignantMagzNo ratings yet
- Face Tanner: HB179, HB175, HB172Document76 pagesFace Tanner: HB179, HB175, HB172gheorghe_georgelNo ratings yet
- Asian Hps ReportDocument145 pagesAsian Hps ReportUMRATUN HAYATINo ratings yet
- Carcinoma of Prostate: Patho Ogy - Chapter &Document29 pagesCarcinoma of Prostate: Patho Ogy - Chapter &HAMIDNo ratings yet
- Cell Line Profile MDA-MB-231 (ECACC Catalogue No.)Document3 pagesCell Line Profile MDA-MB-231 (ECACC Catalogue No.)Manikanta Sai KumarNo ratings yet
- Communique of The 5TH National Conference On Environment and HealthDocument8 pagesCommunique of The 5TH National Conference On Environment and HealthJoshuaNo ratings yet
- Summary of BASICS OF DIFFUSION MRI PDFDocument13 pagesSummary of BASICS OF DIFFUSION MRI PDFParamitha AdriyatiNo ratings yet
- DIANDRA PARIKESIT Thrombus-Like - Tumor - of - Renal - Cell - Carcinoma - MimickDocument4 pagesDIANDRA PARIKESIT Thrombus-Like - Tumor - of - Renal - Cell - Carcinoma - MimickYulia DjatiwardaniNo ratings yet
- 02 Breast PDFDocument15 pages02 Breast PDFANAS ALINo ratings yet
- Standardization of The Definition and Surgical.9Document11 pagesStandardization of The Definition and Surgical.9JobelleNo ratings yet
- Instructor's Presentation-Tumor MarkersDocument57 pagesInstructor's Presentation-Tumor MarkersMACOB, ETHELHYN JHANENo ratings yet
- Family Support and Self-Esteem of Patient With Breast CancerDocument5 pagesFamily Support and Self-Esteem of Patient With Breast CancerDean Rex Azriel TelaumbanuaNo ratings yet
- ProstateDocument204 pagesProstatevonicaNo ratings yet
- 17, Feb, FDocument13 pages17, Feb, FMohsin AliNo ratings yet
- Elsevier HPV 16-18Document8 pagesElsevier HPV 16-18Kevin SNo ratings yet
- Malignant Proliferating Trichilemmal Tumor One Case and Literature ReviewDocument4 pagesMalignant Proliferating Trichilemmal Tumor One Case and Literature ReviewIJAR JOURNALNo ratings yet
- Liposarcoma Cyto PDFDocument10 pagesLiposarcoma Cyto PDFHerdyastuti NurwestriNo ratings yet
- Comparing Breast-Conserving Surgery With Radical MastectomyDocument6 pagesComparing Breast-Conserving Surgery With Radical MastectomyRonald Cariaco FlamesNo ratings yet
- Melanoma 2016Document413 pagesMelanoma 2016Anca-Raluca Pascu100% (2)
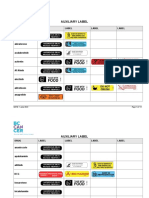
- Auxiliary Label LISTDocument14 pagesAuxiliary Label LISTAbdur RachmanNo ratings yet