You might also like
- Systems Hydraulics - Massey FergussonDocument15 pagesSystems Hydraulics - Massey FergussonJPJFNo ratings yet
- Abnormal Heart Sounds: First Heart Sound (S)Document4 pagesAbnormal Heart Sounds: First Heart Sound (S)Faris Mufid MadyaputraNo ratings yet
- Sistema Lubricacion Cummins Diesel C8.3Document6 pagesSistema Lubricacion Cummins Diesel C8.3Pitricio Campos Del Río100% (2)
- Bombay High AccidentDocument7 pagesBombay High AccidentsapphirerkNo ratings yet
- Stroke - Physiotherapy Treatment Approaches - Physiopedia PDFDocument25 pagesStroke - Physiotherapy Treatment Approaches - Physiopedia PDFBeta100% (2)
- AuscultationDocument41 pagesAuscultationAnonymous ZUaUz1wwNo ratings yet
- 09 - Mastering First Heart SoundDocument10 pages09 - Mastering First Heart SoundSharan MurugaboopathyNo ratings yet
- Oleh: Dina E. Agapa Atmaja Sirupang Enggelin Stevykurnia Arungpadang Chris A.M. Kmur Mirna F. Tandi'RapakDocument38 pagesOleh: Dina E. Agapa Atmaja Sirupang Enggelin Stevykurnia Arungpadang Chris A.M. Kmur Mirna F. Tandi'RapakMeiriyani LembangNo ratings yet
- MURMURDocument21 pagesMURMURtoyyibNo ratings yet
- Extra Systolic Heart SoundDocument23 pagesExtra Systolic Heart SoundAtmaja R. SirupangNo ratings yet
- Principles Auscultatory Areas: ND NDDocument5 pagesPrinciples Auscultatory Areas: ND NDPinay YaunNo ratings yet
- IVMS Heart and Lung Auscultation Sounds NotesDocument7 pagesIVMS Heart and Lung Auscultation Sounds NotesMarc Imhotep Cray, M.D.No ratings yet
- Physiology, Heart Sounds Authors AffiliationsDocument6 pagesPhysiology, Heart Sounds Authors AffiliationsBrandtherootNo ratings yet
- 1 Mitral Stenosis: InstructionDocument8 pages1 Mitral Stenosis: Instructionrashid.scribdNo ratings yet
- Heart SoundsDocument3 pagesHeart Soundsمحمد نعيمNo ratings yet
- Approach To Cardiac MurmursDocument11 pagesApproach To Cardiac Murmurstouthang0074085No ratings yet
- Cardio 2Document2 pagesCardio 2Erika De JesusNo ratings yet
- Heart SoundsDocument17 pagesHeart SoundsAlfrin Antony100% (3)
- Approach To The Patient With A Heart Murmur - Thoracic KeyDocument14 pagesApproach To The Patient With A Heart Murmur - Thoracic KeyFitri NurullahNo ratings yet
- Atrial, Jugular Pressures and Heart SoundDocument11 pagesAtrial, Jugular Pressures and Heart Soundtehillahkabwe100No ratings yet
- Heart SoundsDocument56 pagesHeart SoundsBetsy Babilonia100% (1)
- 7th Heart Sounds and MurmursDocument6 pages7th Heart Sounds and MurmursbabibubeboNo ratings yet
- S and S: Presenter: Guidance and ModerationDocument60 pagesS and S: Presenter: Guidance and ModerationCatherine PaulNo ratings yet
- Heart Murmurs Topic Review - From Description To AuscultationDocument15 pagesHeart Murmurs Topic Review - From Description To AuscultationRapmle PrasadNo ratings yet
- Heart SoundsDocument4 pagesHeart SoundsEros ThanatosNo ratings yet
- Heart SoundDocument2 pagesHeart SounddamarisapNo ratings yet
- Endocardium. The Subendocardial TissueDocument8 pagesEndocardium. The Subendocardial TissuedeanNo ratings yet
- 2017 Labkomp - Auskultation-Bloodpressure - Niklas IvarssonDocument19 pages2017 Labkomp - Auskultation-Bloodpressure - Niklas IvarssonJohn Paolo JosonNo ratings yet
- Mitral StenosisDocument2 pagesMitral StenosisKing Bal94No ratings yet
- The Myth of The HabandurasoDocument15 pagesThe Myth of The HabandurasoAlrick GonzalezNo ratings yet
- HEART AND LUNG SOUNDS: Reading For IVMS Heart and Lung Auscultation PageDocument87 pagesHEART AND LUNG SOUNDS: Reading For IVMS Heart and Lung Auscultation PageMarc Imhotep Cray, M.D.100% (4)
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDocument6 pagesHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNo ratings yet
- Mid-Systolic Ejection: Time Condition DescriptionDocument3 pagesMid-Systolic Ejection: Time Condition DescriptionZahrosofi AhmadahNo ratings yet
- Apical Pulse AssessmentDocument9 pagesApical Pulse AssessmentmscastrogelacastroNo ratings yet
- S1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesDocument10 pagesS1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesCHARIEMAE CA�AZARESNo ratings yet
- Valvular Heart Disease1Document80 pagesValvular Heart Disease1Abnet WondimuNo ratings yet
- Journal of Nursing: Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyDocument8 pagesJournal of Nursing: Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyNiala AlmarioNo ratings yet
- Auscultatia CardiacaDocument9 pagesAuscultatia CardiacaMh MhNo ratings yet
- Research Paper On Heart MurmurDocument4 pagesResearch Paper On Heart Murmurnodahydomut2100% (1)
- Cardiovascular Physical ExaminationDocument29 pagesCardiovascular Physical ExaminationannisNo ratings yet
- Cardiovascular SystemDocument74 pagesCardiovascular Systemاسامة محمد السيد رمضانNo ratings yet
- 51e - Approach To The Patient With A Heart MurmurDocument16 pages51e - Approach To The Patient With A Heart MurmurSiva RamanNo ratings yet
- Mitral StenosisDocument15 pagesMitral StenosisAshwin Aby ThomasNo ratings yet
- Aaa Ejempl TraductDocument8 pagesAaa Ejempl TraductJm GamaNo ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- Cardiac MurmursDocument53 pagesCardiac MurmursdrgashokNo ratings yet
- 7 Heart Sounds LectureDocument27 pages7 Heart Sounds LecturebvkjtzrvnyNo ratings yet
- Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyDocument7 pagesBasic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest Radiographyrowd1yNo ratings yet
- Stenoza AorticaDocument31 pagesStenoza Aorticamicaella07No ratings yet
- Cardiac Cycle - Atrial Contraction (Phase 1)Document10 pagesCardiac Cycle - Atrial Contraction (Phase 1)Fatima KhanNo ratings yet
- 2 Valvular Heart Disease1Document87 pages2 Valvular Heart Disease1Danny DesuNo ratings yet
- Differential Diagnosis of Valvular Heart DiseaseDocument10 pagesDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeeNo ratings yet
- Prof. Maharlika Levi Sumilang: Heart Assessment NCM112 MS RLE 8/7/21Document6 pagesProf. Maharlika Levi Sumilang: Heart Assessment NCM112 MS RLE 8/7/21Yman Gio BumanglagNo ratings yet
- The Cardiac CycleDocument19 pagesThe Cardiac CycleRebi NesroNo ratings yet
- Cardio AuscultationDocument19 pagesCardio AuscultationshadabNo ratings yet
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNo ratings yet
- Heart Sounds and Arteriovenous Pulses: DR Chandana HewageDocument48 pagesHeart Sounds and Arteriovenous Pulses: DR Chandana HewagePrasad HewawasamNo ratings yet
- Heart Sounds - PracticalDocument7 pagesHeart Sounds - Practicalshadapaaak100% (1)
- Valves Part 2Document2 pagesValves Part 2AIKA BAYANo ratings yet
- ABC of Clinical Electrocardiography Myocardial IschaemiaDocument6 pagesABC of Clinical Electrocardiography Myocardial IschaemiaShri Mahalaxmi HarishNo ratings yet
- Heart PathophysiologyDocument20 pagesHeart PathophysiologyDoctorDrapion100% (2)
- Week 5 1Document6 pagesWeek 5 1deanNo ratings yet
- Penyakit Katup Jantung-Kuliah DR ErlinaDocument70 pagesPenyakit Katup Jantung-Kuliah DR ErlinaAdhiatma DotNo ratings yet
- All in OneDocument99 pagesAll in OneAKANKSHA RANANo ratings yet
- Rheumato AllDocument224 pagesRheumato AllAKANKSHA RANANo ratings yet
- Psychiatry Exam 2018 BSU 1Document98 pagesPsychiatry Exam 2018 BSU 1AKANKSHA RANANo ratings yet
- Urology All in OneDocument107 pagesUrology All in OneAKANKSHA RANANo ratings yet
- Public Health Final Exam-Nizharadze-AnswersDocument39 pagesPublic Health Final Exam-Nizharadze-AnswersAKANKSHA RANANo ratings yet
- MIDTERMDocument34 pagesMIDTERMAKANKSHA RANANo ratings yet
- Shched Vii Admission 142 Spring 2021Document166 pagesShched Vii Admission 142 Spring 2021AKANKSHA RANANo ratings yet
- Islamic (Hijri) Calendar For Year 1962 CE: Based On Global Crescent Moon Sighting ProbabilityDocument8 pagesIslamic (Hijri) Calendar For Year 1962 CE: Based On Global Crescent Moon Sighting ProbabilityMohsin Hassas MohsinNo ratings yet
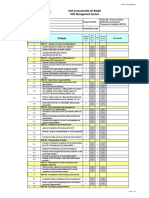
- HSE Evaluation CriteriaDocument2 pagesHSE Evaluation CriteriaChan RizkyNo ratings yet
- Lesson 5 - Single Sideband System: ECE121 - Principles of CommunicationsDocument67 pagesLesson 5 - Single Sideband System: ECE121 - Principles of CommunicationsJhezreel JohnNo ratings yet
- Drugs To Avoid in Myasthenia GravisDocument3 pagesDrugs To Avoid in Myasthenia GravispapitomalosoNo ratings yet
- JESA - Welding Grinding & Cutting WorksDocument7 pagesJESA - Welding Grinding & Cutting WorksLeo PascualNo ratings yet
- Lime and Dolomite For The Steel IndustryDocument8 pagesLime and Dolomite For The Steel IndustrychmsarfrazNo ratings yet
- Ee101 Jfet 1 PDFDocument70 pagesEe101 Jfet 1 PDFShubham Khoker100% (1)
- Potential Prospects of Petcare Sector in IndiaDocument12 pagesPotential Prospects of Petcare Sector in IndiaParas03No ratings yet
- Efficiency of Asphalt and Concrete in Road ConstructionDocument18 pagesEfficiency of Asphalt and Concrete in Road ConstructionTimothy James S ReyesNo ratings yet
- Conducting Diving Operations ACOPDocument75 pagesConducting Diving Operations ACOPkanakarao1100% (1)
- Totemtek ATxx Series Product User Manual V3.0.1Document17 pagesTotemtek ATxx Series Product User Manual V3.0.1runtimeavlNo ratings yet
- Vegetal Vs Mineral OilsDocument6 pagesVegetal Vs Mineral OilsDark CenobiteNo ratings yet
- Ayurveda Perspective of Natural Drug Interaction: A Literature ReviewDocument3 pagesAyurveda Perspective of Natural Drug Interaction: A Literature ReviewBhavana GangurdeNo ratings yet
- Ceramic Matrix CompositeDocument10 pagesCeramic Matrix CompositeMohammed KhalidNo ratings yet
- AJPTR Pharmaceutical Packaging TechnologyDocument13 pagesAJPTR Pharmaceutical Packaging TechnologyNitin KashyapNo ratings yet
- NZ 46 Flying ClubsDocument4 pagesNZ 46 Flying ClubsNZHHNo ratings yet
- Analytical Modeling of Graded Channel TFET - v1Document5 pagesAnalytical Modeling of Graded Channel TFET - v1sudipta2580No ratings yet
- Disinfectants HandoutDocument3 pagesDisinfectants HandoutNelson michaelNo ratings yet
- Unit 5 Biology NotesDocument21 pagesUnit 5 Biology Notes098789100% (1)
- Technical Leaflet Cim 776 & Cim 777Document16 pagesTechnical Leaflet Cim 776 & Cim 777blindjaxxNo ratings yet
- Quiz 1Document2 pagesQuiz 1Jun RyNo ratings yet
- ID DCU IndustrialDocument4 pagesID DCU IndustrialRoozbeh BahmanyarNo ratings yet
- Hurtado2003 PlomoDocument8 pagesHurtado2003 Plomopilar1984No ratings yet
- Dengue CRF - FillableDocument3 pagesDengue CRF - FillableRosario Dalida100% (1)
- Krishnas Final Year ProjectDocument33 pagesKrishnas Final Year ProjectVIGNESHWARAN VNo ratings yet
- 1112 - JEMDS Title PageDocument2 pages1112 - JEMDS Title PageKriti KumariNo ratings yet