You might also like
- 吸烟的风险Document9 pages吸烟的风险xiaoxin zhangNo ratings yet
- Cigarro-Cx 3er MolarDocument5 pagesCigarro-Cx 3er MolardralexguerraNo ratings yet
- Studies of Kidney Cancer and PCBsDocument19 pagesStudies of Kidney Cancer and PCBsl-cristinaNo ratings yet
- Articol Paro 1Document7 pagesArticol Paro 1Raluca ElenaNo ratings yet
- JurnalDocument6 pagesJurnalSiska SulistiyowatiNo ratings yet
- Immune Function in Cigarette Smokers Who Quit Smoking For 31 DaysDocument10 pagesImmune Function in Cigarette Smokers Who Quit Smoking For 31 DaysVu Anh KienNo ratings yet
- Azitromicyn COPDDocument10 pagesAzitromicyn COPDLucrécia BórgiaNo ratings yet
- Informacion Periodontitis y FumarDocument3 pagesInformacion Periodontitis y FumarFelipe MartinezNo ratings yet
- Adj 12747Document7 pagesAdj 12747Irfan HussainNo ratings yet
- Factors Affecting Dropout in The Smoking Cessation Outpatient ClinicDocument7 pagesFactors Affecting Dropout in The Smoking Cessation Outpatient ClinicAmbarsari HamidahNo ratings yet
- Health Consequences of Sustained Smoking Cessation FinalDocument5 pagesHealth Consequences of Sustained Smoking Cessation FinalAmin Mohamed Amin DemerdashNo ratings yet
- Chapter 3Document3 pagesChapter 3Cayanong Joel Jr I.No ratings yet
- Azithromycin For Prevention of Exacerbations of COPDDocument10 pagesAzithromycin For Prevention of Exacerbations of COPDAJNo ratings yet
- Plasma MalonDocument4 pagesPlasma MalonAdria Putra FarhandikaNo ratings yet
- Clinical Trial On The Effects of Oral Magnesium SuDocument9 pagesClinical Trial On The Effects of Oral Magnesium SuJose Alexander Ramirez GarciaNo ratings yet
- Direct Hemoperfusion Using A Polymyxin B-Immobilized Polystyrene Column For COVID-19Document9 pagesDirect Hemoperfusion Using A Polymyxin B-Immobilized Polystyrene Column For COVID-19TisaNo ratings yet
- Non Farmako Mulhall ReviewDocument19 pagesNon Farmako Mulhall Reviewgita cahayaNo ratings yet
- Chest: Systemic Effects of SmokingDocument10 pagesChest: Systemic Effects of SmokingArlen ResnawaldiNo ratings yet
- Antitumor Effects of Octreotide LAR, A Somatostatin AnalogDocument2 pagesAntitumor Effects of Octreotide LAR, A Somatostatin AnalogVmiguel LcastilloNo ratings yet
- Lit 6 Smoking CessationDocument6 pagesLit 6 Smoking CessationAnonymous 8rsxG4No ratings yet
- Effect of Initial Periodontal Therapy On The Oxidative Stress Markers in Gingival Crevicular Fluid, Saliva and Serum in Smokers and Non-Smokers With Chronic PeriodontitisDocument13 pagesEffect of Initial Periodontal Therapy On The Oxidative Stress Markers in Gingival Crevicular Fluid, Saliva and Serum in Smokers and Non-Smokers With Chronic Periodontitisanzila widyaNo ratings yet
- Cigarette Smoking and Asthma: Clinical Management ReviewDocument15 pagesCigarette Smoking and Asthma: Clinical Management ReviewMuhammad FikriNo ratings yet
- Systematic ReviewDocument19 pagesSystematic ReviewGery RifanoNo ratings yet
- Chapter 5 Tobacco Harm ReductionDocument4 pagesChapter 5 Tobacco Harm ReductionFoamm KitNo ratings yet
- Smoking and Periodontal DiseasesDocument9 pagesSmoking and Periodontal DiseasesSnowNo ratings yet
- Evaluation of The Impact of Cigarette Smoking OnDocument6 pagesEvaluation of The Impact of Cigarette Smoking OnBerenice SánchezNo ratings yet
- Ijii 1 101 PDFDocument3 pagesIjii 1 101 PDFLarry MicksNo ratings yet
- Treatment of Chronic Rhinosinusitis and Its Effects On AsthmaDocument7 pagesTreatment of Chronic Rhinosinusitis and Its Effects On AsthmaHalilGutajNo ratings yet
- Passive SmokingDocument6 pagesPassive SmokingHanifahNo ratings yet
- Alifiani-Jurding SNNTDocument9 pagesAlifiani-Jurding SNNTYAHYA Al-HILALNo ratings yet
- Infrared Imaging To Measure Cigarette Smoking Induced Vasoconstriction EffectsDocument15 pagesInfrared Imaging To Measure Cigarette Smoking Induced Vasoconstriction Effectsshanelynn3No ratings yet
- Cytomorphometric Analysis of Exfoliated Buccal Mucosal Cells in Smokers and Patients With Hypertension: A Quantitative AnalysisDocument7 pagesCytomorphometric Analysis of Exfoliated Buccal Mucosal Cells in Smokers and Patients With Hypertension: A Quantitative AnalysisKarina KabanNo ratings yet
- Body Image and Acute Burn Injuries A Literature ReviewDocument8 pagesBody Image and Acute Burn Injuries A Literature ReviewbeemwvrfgNo ratings yet
- ARDS Meduri JAMA 1998Document8 pagesARDS Meduri JAMA 1998Rivaneide AmorimNo ratings yet
- Smoking Literature ReviewDocument8 pagesSmoking Literature Reviewea6qsxqd100% (1)
- Smoking and Periodontal Disease: A Review: January 2007Document8 pagesSmoking and Periodontal Disease: A Review: January 2007Ralph TampubolonNo ratings yet
- Ebm NSCLCDocument8 pagesEbm NSCLCNaja HasnandaNo ratings yet
- S1359634912X00028 S1359634912700253 MainDocument7 pagesS1359634912X00028 S1359634912700253 MainindracuangNo ratings yet
- Jop 2010 100195Document8 pagesJop 2010 100195Dull DeviceNo ratings yet
- Smoking and Periodontal Disease - Francisco Rivera HidalgoDocument9 pagesSmoking and Periodontal Disease - Francisco Rivera HidalgoSebastián TissoneNo ratings yet
- Art:10.1186/s13063 016 1456 4Document10 pagesArt:10.1186/s13063 016 1456 4dani yan sNo ratings yet
- 1 s2.0 S1936523312800428 MainDocument9 pages1 s2.0 S1936523312800428 MainJessica GintingNo ratings yet
- Jouko - Tuomisto@ktl - Fi Other Sections Materials and Methods Results Discussion ReferencesDocument19 pagesJouko - Tuomisto@ktl - Fi Other Sections Materials and Methods Results Discussion ReferencesBab33No ratings yet
- Black2010 PDFDocument9 pagesBlack2010 PDFAntung AlangdeoNo ratings yet
- Steroids and Antiobiotics in TonsillectomyDocument9 pagesSteroids and Antiobiotics in TonsillectomyjulianasanjayaNo ratings yet
- 2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRDocument2 pages2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRPoljarLijanNo ratings yet
- June 1, 2010: 2360 CirculationDocument5 pagesJune 1, 2010: 2360 CirculationJulie KleinNo ratings yet
- Lycopene and Myocardial Infarction Risk in The EURAMIC StudyDocument9 pagesLycopene and Myocardial Infarction Risk in The EURAMIC StudySUBHADIP MANIKNo ratings yet
- Because ARDS Is Initiated by Excessive Inflammation, Corticosteroids Were TheDocument4 pagesBecause ARDS Is Initiated by Excessive Inflammation, Corticosteroids Were TheOtrebron BatisanNo ratings yet
- Jurnal Microsatelie 2Document7 pagesJurnal Microsatelie 2Ieien MuthmainnahNo ratings yet
- Simvastatin For The Prevention of Exacerbations in Moderate-to-Severe COPDDocument10 pagesSimvastatin For The Prevention of Exacerbations in Moderate-to-Severe COPDdhamaraNo ratings yet
- What's New in Respiratory DisordersDocument4 pagesWhat's New in Respiratory DisorderssobanNo ratings yet
- Gfac 227Document8 pagesGfac 227Cristina Adriana PopaNo ratings yet
- Treatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinDocument5 pagesTreatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinUbaidillah HafidzNo ratings yet
- Artigo Introdução 06Document32 pagesArtigo Introdução 06ANA CAROLINE ANDRADE DE MELONo ratings yet
- Bisa 1Document8 pagesBisa 1justforuroNo ratings yet
- 1302 FullDocument9 pages1302 FullSupicha VichaiditNo ratings yet
- 18th European Burns Association Congress: Jyrki VuolaDocument188 pages18th European Burns Association Congress: Jyrki Vuolaagatha cindyNo ratings yet
- Smoking & Periodontal DiseaseDocument20 pagesSmoking & Periodontal DiseasePrathik RaiNo ratings yet
- Calculation of Wind Loads On Monopitch Canopies - Eurocode 1Document7 pagesCalculation of Wind Loads On Monopitch Canopies - Eurocode 1MPBGDNo ratings yet
- Victorias Climate Science Report 2019Document48 pagesVictorias Climate Science Report 2019Alexander DarlingNo ratings yet
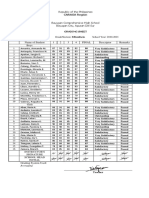
- Ma Angela Kristine Valencia - B. Grading Sheet Fili - 8Document1 pageMa Angela Kristine Valencia - B. Grading Sheet Fili - 8Ma. Angela Kristine ValenciaNo ratings yet
- Xviii The Roots of CalculusDocument3 pagesXviii The Roots of CalculusDaniel VargasNo ratings yet
- Incident Record Form ASSIGNMENTDocument3 pagesIncident Record Form ASSIGNMENTJustin Raymundo CuyanNo ratings yet
- Do-It-Yourself Chain Link Fence and Gate Installation InstructionsDocument11 pagesDo-It-Yourself Chain Link Fence and Gate Installation InstructionsvjNo ratings yet
- 2nd Quarter Exam Empowerment - TechnologiesDocument3 pages2nd Quarter Exam Empowerment - Technologieskathryn soriano100% (11)
- ResumeDocument4 pagesResumeapi-233282347No ratings yet
- The Basics of Capital BudgetingDocument35 pagesThe Basics of Capital BudgetingFebriannNo ratings yet
- Pr1 CP Mathandscigr11Document65 pagesPr1 CP Mathandscigr11AllyNo ratings yet
- Weibull DistributionDocument5 pagesWeibull Distributionknight1410No ratings yet
- Invoice 1 - GecolDocument1 pageInvoice 1 - Gecolq8rjsqvssyNo ratings yet
- Ee3101 Lab Report ExpDocument16 pagesEe3101 Lab Report ExpyucesNo ratings yet
- 01-02 VXLAN Deployment ModesDocument4 pages01-02 VXLAN Deployment ModesAbdelhaiNo ratings yet
- B9 Main Ideas ML-1Document3 pagesB9 Main Ideas ML-1rd4tp5k25gNo ratings yet
- Material Safety Data Sheet: L IdentificationDocument4 pagesMaterial Safety Data Sheet: L Identificationkesling rsiNo ratings yet
- UNIT-5 FullDocument99 pagesUNIT-5 Fullsyedali24779No ratings yet
- Common Book ProjectDocument16 pagesCommon Book Projectgamergod6978No ratings yet
- Anh 6 Kim Hien Key Kì 2Document18 pagesAnh 6 Kim Hien Key Kì 2Diệu NguyễnNo ratings yet
- AMLTM.00.092-00-Iss1 Tape Adhesion Test For Paints and CoatingsDocument6 pagesAMLTM.00.092-00-Iss1 Tape Adhesion Test For Paints and CoatingsalbertoNo ratings yet
- Installation & Maintenance Instructions: Description / IdentificationDocument6 pagesInstallation & Maintenance Instructions: Description / IdentificationPrimadani KurniawanNo ratings yet
- Episode 68 Transcript - Listening TimeDocument5 pagesEpisode 68 Transcript - Listening TimeSDMK Dinkes DKINo ratings yet
- Module 6Document4 pagesModule 6api-701165246No ratings yet
- Nao Presentation - Robotics Lab, KCTDocument16 pagesNao Presentation - Robotics Lab, KCTRamkumar ANo ratings yet
- Instructions: Mixer ManualDocument46 pagesInstructions: Mixer ManualJose VidalNo ratings yet
- Lesson Plan On Body Parts For EslDocument2 pagesLesson Plan On Body Parts For Eslapi-265046009No ratings yet
- Desert Sun Arts & Entertainment Oct. 27, Nov. 3 2019Document22 pagesDesert Sun Arts & Entertainment Oct. 27, Nov. 3 2019julie makinenNo ratings yet
- WOCN OCA Learning OutcomesDocument3 pagesWOCN OCA Learning OutcomesNieva Portia Bunagan-DuriaNo ratings yet
- Python Lab Manual - III BCA (1 To 10)Document23 pagesPython Lab Manual - III BCA (1 To 10)sp2392546No ratings yet
- Assignment 1 302 Fall 2009. CorrectDocument2 pagesAssignment 1 302 Fall 2009. CorrectJohn HopkinsNo ratings yet
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (2)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (6)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Ultrametabolism: The Simple Plan for Automatic Weight LossFrom EverandUltrametabolism: The Simple Plan for Automatic Weight LossRating: 4.5 out of 5 stars4.5/5 (28)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- The Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayFrom EverandThe Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayNo ratings yet
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaFrom EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaNo ratings yet
- Dr. Nowzaradan's Diet Plan: The Scales Don't Lie, People Do! The Only 1200 kcal Diet from Dr. NOW to Lose Weight Fast. 30-Day Diet PlanFrom EverandDr. Nowzaradan's Diet Plan: The Scales Don't Lie, People Do! The Only 1200 kcal Diet from Dr. NOW to Lose Weight Fast. 30-Day Diet PlanNo ratings yet
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (353)