You might also like
- Clinical & Counseling AssessmentDocument52 pagesClinical & Counseling AssessmentMaica GuceNo ratings yet
- 1619921936223forensic Science UNIT - I PDFDocument86 pages1619921936223forensic Science UNIT - I PDFVyshnav RNo ratings yet
- Global Marketing-Case Analysis (Starbucks in Austraila)Document9 pagesGlobal Marketing-Case Analysis (Starbucks in Austraila)Reginald Yesuthasan100% (1)
- Low Hanging SystemDocument69 pagesLow Hanging SystemVina100% (1)
- Organizational Behaviour - Lecture NotesDocument143 pagesOrganizational Behaviour - Lecture NotesRachel Ruban80% (20)
- Classification of Behaviour and Experience in Relation To Functional Psychiatric Diagnoses-Time For A Paradigm ShiftDocument12 pagesClassification of Behaviour and Experience in Relation To Functional Psychiatric Diagnoses-Time For A Paradigm ShiftJaime Iván Hernández España100% (2)
- Pokerole Core Rulebook 2.0Document489 pagesPokerole Core Rulebook 2.0Trey Bachtiger100% (2)
- Saturn's Pending Karmas Karma Sunil JohnDocument15 pagesSaturn's Pending Karmas Karma Sunil JohnSmith Farat100% (6)
- Stigma and Outcome of Treatment Among Patients With Psychological Disorders and Their AttendersDocument5 pagesStigma and Outcome of Treatment Among Patients With Psychological Disorders and Their AttendersFathima ZoharaNo ratings yet
- Chapter 5Document42 pagesChapter 5peachypeachyNo ratings yet
- AssignmentDocument19 pagesAssignmentYashika Jain -63No ratings yet
- Measurement Scavenger HuntDocument6 pagesMeasurement Scavenger HuntDakota HoneycuttNo ratings yet
- Qualification ExaminationDocument4 pagesQualification ExaminationpsychologistkomalNo ratings yet
- Ser 9 3 240Document8 pagesSer 9 3 240Catarina C.No ratings yet
- FINAL-DEFENSE-by Jerome, Vimal, Gopi, MawteiDocument21 pagesFINAL-DEFENSE-by Jerome, Vimal, Gopi, MawteiVineeNo ratings yet
- Control Perception FinalDocument7 pagesControl Perception FinalAdina BusteaNo ratings yet
- A Systematic Review and Psychometric Evaluation of Self-Report HoardingDocument45 pagesA Systematic Review and Psychometric Evaluation of Self-Report HoardingAmita GoyalNo ratings yet
- A Meta Analysis of Self Determination Theory Informed Intervention Studies in The Health Domain Effects On Motivation Health Behavior Physical andDocument32 pagesA Meta Analysis of Self Determination Theory Informed Intervention Studies in The Health Domain Effects On Motivation Health Behavior Physical andDwi Yanti AyuNo ratings yet
- Measuring Psychological Distress 5Document32 pagesMeasuring Psychological Distress 5api-548101002No ratings yet
- Running Head: Effectiveness of Dementia Inteventions 1Document12 pagesRunning Head: Effectiveness of Dementia Inteventions 1John Mureithi NjugunaNo ratings yet
- Week 6 Psych 655Document5 pagesWeek 6 Psych 655KimMorganNo ratings yet
- Materi Kuliah ToksikologiDocument8 pagesMateri Kuliah Toksikologiradiaputri25No ratings yet
- Concept Paper - GADDocument6 pagesConcept Paper - GADDeniseNo ratings yet
- 2011 Detection of Depression and Anxiety Disorders in Primary Care Friendly)Document9 pages2011 Detection of Depression and Anxiety Disorders in Primary Care Friendly)rocksurNo ratings yet
- Running Head: Effectiveness of Dementia Inteventions 1Document17 pagesRunning Head: Effectiveness of Dementia Inteventions 1John Mureithi NjugunaNo ratings yet
- What Is The Impact of Mental Health-Related Stigma On Help-Seeking? A Systematic Review of Quantitative and Qualitative StudiesDocument49 pagesWhat Is The Impact of Mental Health-Related Stigma On Help-Seeking? A Systematic Review of Quantitative and Qualitative Studiesjulia torNo ratings yet
- Principles of GeriatricsDocument12 pagesPrinciples of GeriatricsEveryday LearnerNo ratings yet
- Case Presentation StyleDocument7 pagesCase Presentation StyleNiteshSinghNo ratings yet
- Psychiatric Nursing Notes: History, AsylumsDocument62 pagesPsychiatric Nursing Notes: History, Asylumssurviving nursing school100% (1)
- Predictors of Quality of Life Among Chinese People With SchizophreniaDocument7 pagesPredictors of Quality of Life Among Chinese People With SchizophreniawindaRQ96No ratings yet
- Original Article: ISSN: 0976 3325Document4 pagesOriginal Article: ISSN: 0976 3325Adina OlteanuNo ratings yet
- Vacarolis Chapter OutlinesDocument181 pagesVacarolis Chapter Outlinesamashriqi100% (1)
- Psychosocial NursingDocument21 pagesPsychosocial NursingAngeline Angeles100% (1)
- C9a1 PDFDocument12 pagesC9a1 PDFfujfrNo ratings yet
- Lecture 2 Health Beliefs by WindaDocument20 pagesLecture 2 Health Beliefs by Windawinda lestariNo ratings yet
- Quality of Life in Caregivers of Patients With Schizophrenia A Literature ReviewDocument6 pagesQuality of Life in Caregivers of Patients With Schizophrenia A Literature Reviewgw0q12dxNo ratings yet
- GHQ Intro and BCDocument4 pagesGHQ Intro and BCIndrashis MandalNo ratings yet
- University of Health and Allied Sciences School of Public HealthDocument12 pagesUniversity of Health and Allied Sciences School of Public HealthWillis ITNo ratings yet
- Crisis Counselling - Caring People With Mental DistubancesDocument6 pagesCrisis Counselling - Caring People With Mental DistubancesVictor JamesNo ratings yet
- UiTM STA555 Project Report SampleDocument39 pagesUiTM STA555 Project Report SampleEmma100% (7)
- W A Psychopathology and Mental HealthDocument6 pagesW A Psychopathology and Mental HealthBen ObiNo ratings yet
- 01 Taylor-Rodgers Evaluation of An Online 2014Document7 pages01 Taylor-Rodgers Evaluation of An Online 2014sushmita bhartiaNo ratings yet
- Impact of Stigma On The Clients' Participation in Mental Health ServicesDocument19 pagesImpact of Stigma On The Clients' Participation in Mental Health ServicesJoshua C. Gandi100% (1)
- The Future of Psychology Compassion-Focused Outcomes & Using Technology To Increase Compassion Worldwide - Yotam HeinebergDocument28 pagesThe Future of Psychology Compassion-Focused Outcomes & Using Technology To Increase Compassion Worldwide - Yotam HeinebergccareemailNo ratings yet
- Insight and Symptom Severity in An Inpatient Psychiatric SampleDocument12 pagesInsight and Symptom Severity in An Inpatient Psychiatric SamplealejandraNo ratings yet
- Dissertation Mental Health StigmaDocument8 pagesDissertation Mental Health StigmaNeedSomeoneWriteMyPaperIndianapolis100% (1)
- Rou Saud 2007Document11 pagesRou Saud 2007healliz36912No ratings yet
- Mental Health Nursing Module 1 - Introduction Student 2023Document44 pagesMental Health Nursing Module 1 - Introduction Student 2023Biology TutorNo ratings yet
- ShowPDF PaperDocument9 pagesShowPDF Paperdipak suresh sawarkarNo ratings yet
- Perception About General Awarness of Mental Illness: Group A2Document23 pagesPerception About General Awarness of Mental Illness: Group A2Dilawar JanNo ratings yet
- Psychosocial Interventions CompleteDocument14 pagesPsychosocial Interventions CompleteDwane PaulsonNo ratings yet
- 8.5 Health PromotionDocument30 pages8.5 Health PromotionEstela Such GilNo ratings yet
- Social Work Mental Health Dissertation IdeasDocument6 pagesSocial Work Mental Health Dissertation IdeasCollegePapersWritingServiceCanada100% (1)
- Differential Mental Health Assessment in Older Adults Lecture NotesDocument34 pagesDifferential Mental Health Assessment in Older Adults Lecture NotesMagishaa ThiyagarajahNo ratings yet
- Lesson 4 - Mental Health Across The Lifespan: Disaster and Mental Health/ Compiled By: Minera Laiza C. AcostaDocument5 pagesLesson 4 - Mental Health Across The Lifespan: Disaster and Mental Health/ Compiled By: Minera Laiza C. AcostaCala WritesNo ratings yet
- Lay Beliefs About Treatments For People With Mental Illness and Their Implications For Antistigma StrategiesDocument8 pagesLay Beliefs About Treatments For People With Mental Illness and Their Implications For Antistigma Strategiesshah khalidNo ratings yet
- Factor Influncing Depression Among AdolescentsDocument5 pagesFactor Influncing Depression Among AdolescentsIJSTENo ratings yet
- Challenge Facing People Living With Hiv and Aids in GithuraiDocument5 pagesChallenge Facing People Living With Hiv and Aids in GithuraiorigafelixNo ratings yet
- Herman 2011Document8 pagesHerman 2011weni astutiNo ratings yet
- Research Paper On Mental IllnessDocument9 pagesResearch Paper On Mental Illnessiangetplg100% (1)
- Mental Health FacilitiesDocument11 pagesMental Health FacilitiesMiKayla PenningsNo ratings yet
- Online Teaching SO 100 5.0 Health Seeking Behaviour, Access, and Utilization of Health Services (For 16. 06. 2020) - Latest VersionDocument28 pagesOnline Teaching SO 100 5.0 Health Seeking Behaviour, Access, and Utilization of Health Services (For 16. 06. 2020) - Latest VersionBenjamin DanielNo ratings yet
- Thesis RevisionDocument3 pagesThesis RevisionJoshuaNo ratings yet
- Psychosocial Interventions DraftDocument12 pagesPsychosocial Interventions DraftDwane PaulsonNo ratings yet
- Finding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareFrom EverandFinding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareNo ratings yet
- Inpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsFrom EverandInpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsHoward H. FennNo ratings yet
- The 2019 Novel Coronavirus Disease Introduction Sep 2022Document2 pagesThe 2019 Novel Coronavirus Disease Introduction Sep 2022Saadia TalibNo ratings yet
- Qualitative and Quantitative Research Methodology Mix MethodDocument1 pageQualitative and Quantitative Research Methodology Mix MethodSaadia TalibNo ratings yet
- Table of Contents OCD and Covid SurvivorsDocument1 pageTable of Contents OCD and Covid SurvivorsSaadia TalibNo ratings yet
- Managing OCD During The Coronavirus Pandemic Internet SourceDocument13 pagesManaging OCD During The Coronavirus Pandemic Internet SourceSaadia TalibNo ratings yet
- Scale Aircraft Modelling December 2017 PDFDocument96 pagesScale Aircraft Modelling December 2017 PDFAnonymous N13Jdn100% (2)
- A.M. 1693 The Reformed GentlemanDocument93 pagesA.M. 1693 The Reformed GentlemanMitchell JohnsonNo ratings yet
- Decathlon SD Report FY16 PDFDocument136 pagesDecathlon SD Report FY16 PDFHimanshu Yadav100% (1)
- Company Secretary Journal 2019 - Download ICSI E-Bulletin For Students & Members - Finance Updates 2019Document5 pagesCompany Secretary Journal 2019 - Download ICSI E-Bulletin For Students & Members - Finance Updates 2019Fin UpdatesNo ratings yet
- The Workshop of The Sculptor Thutmose inDocument14 pagesThe Workshop of The Sculptor Thutmose inYara LinariNo ratings yet
- Q4 Applied Eco Learning Material Week7Document8 pagesQ4 Applied Eco Learning Material Week7marvi salmingoNo ratings yet
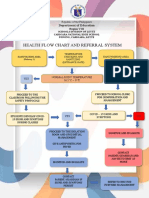
- Health Flow Chart and Referral System: Department of EducationDocument2 pagesHealth Flow Chart and Referral System: Department of EducationWendy TablaNo ratings yet
- Chart Book - Corporate Restructuring Insolvency Liquidation and Winding Up - CS Vaibhav Chitlangia - Yes Academy, PuneDocument47 pagesChart Book - Corporate Restructuring Insolvency Liquidation and Winding Up - CS Vaibhav Chitlangia - Yes Academy, PuneJohn carollNo ratings yet
- Health Benefits of Financial Inclusion A Literature ReviewDocument7 pagesHealth Benefits of Financial Inclusion A Literature Reviewl1wot1j1fon3No ratings yet
- "Kapit Sa Patalim" Proclivity and Perpetuity of "5-6" Credit Facility Among The Wet Market Micro-EntrepreneursDocument28 pages"Kapit Sa Patalim" Proclivity and Perpetuity of "5-6" Credit Facility Among The Wet Market Micro-Entrepreneurszab1226No ratings yet
- District Memo On Deped Ed Run For Students Wave 2 - EditedDocument4 pagesDistrict Memo On Deped Ed Run For Students Wave 2 - EditedNioganElemNo ratings yet
- Southwest Airlines AnalysisDocument6 pagesSouthwest Airlines Analysisdocmund100% (1)
- 10 Chavez Vs ViolaDocument5 pages10 Chavez Vs ViolaJohn JurisNo ratings yet
- 6 Principles To Design A Sales Coaching Curriculum From ScratchDocument19 pages6 Principles To Design A Sales Coaching Curriculum From ScratchRodrigo FerreiraNo ratings yet
- Chapter 3 - Islamic LawsDocument208 pagesChapter 3 - Islamic LawsNur Hidayah Muhammad FauziNo ratings yet
- Different Types of Renewable EnergiesDocument1 pageDifferent Types of Renewable EnergiesJamlick KibuchiNo ratings yet
- Saludo, Jr. vs. Philippine National Bank DigestDocument4 pagesSaludo, Jr. vs. Philippine National Bank DigestEmir Mendoza100% (2)
- 12 Top Five Regrets of The DyingDocument2 pages12 Top Five Regrets of The DyingOvini De SilvaNo ratings yet
- Gonzales V HechanovaDocument2 pagesGonzales V HechanovaMicco PesuenaNo ratings yet
- Consolidation of Financial InstitutionsDocument2 pagesConsolidation of Financial InstitutionsPatricia SorianoNo ratings yet
- Appraisal FormDocument3 pagesAppraisal FormOluwasegun OdunlamiNo ratings yet
- Family, Ancestry, Early Education and Binan StudiesDocument3 pagesFamily, Ancestry, Early Education and Binan Studies셸라No ratings yet
- Flashcards Word PictureDocument34 pagesFlashcards Word PictureNur Lisa Ahmad ZakiNo ratings yet
- David Correia OpinionDocument8 pagesDavid Correia OpinionLaw&CrimeNo ratings yet