You might also like
- Redlands' 2015 California Public Records RequestsDocument26 pagesRedlands' 2015 California Public Records RequestsBeau Yarbrough100% (1)
- LP Africa (11th Edition)Document406 pagesLP Africa (11th Edition)TucaVieiraNo ratings yet
- OB/Gyn Clinical PearlsDocument4 pagesOB/Gyn Clinical PearlsD50% (4)
- InfertilityDocument55 pagesInfertilityFedlu SirajNo ratings yet
- Permaculture - Plants Suitable For Ground Cover (P) - Plants For A FutureDocument2 pagesPermaculture - Plants Suitable For Ground Cover (P) - Plants For A Futurecontadino_impazzitoNo ratings yet
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- InfertilityDocument101 pagesInfertilityjojolilimomo100% (1)
- Toxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa ADocument42 pagesToxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa AAlyssa ManaloNo ratings yet
- Bench WorkDocument103 pagesBench Workgetu abrahaNo ratings yet
- Benha University Hospital Delta (Mansura) & Benha Fertility CentersDocument42 pagesBenha University Hospital Delta (Mansura) & Benha Fertility Centersmadmax500No ratings yet
- Training Sinal PDFDocument15 pagesTraining Sinal PDFlobitoferoz81No ratings yet
- Livro Vertex MACIOCIADocument62 pagesLivro Vertex MACIOCIAxandinhag100% (5)
- AUB StartedDocument13 pagesAUB StartedIbrahim AbdullahNo ratings yet
- Polcystic Ovarian SyndromeDocument9 pagesPolcystic Ovarian SyndromeMelissa BrodoNo ratings yet
- 1926 PapionianDocument108 pages1926 PapionianPLCS_FoundationNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- Newton Papers Letter Nat Phil Cohen EdDocument512 pagesNewton Papers Letter Nat Phil Cohen EdFernando ProtoNo ratings yet
- 80010825Document2 pages80010825rukismen100% (2)
- Din332 PDFDocument4 pagesDin332 PDFmateo100% (2)
- Hyperemesis Gravidarum: By: Solomon Berhe OBGYN ResidentDocument73 pagesHyperemesis Gravidarum: By: Solomon Berhe OBGYN Residentmuleget haileNo ratings yet
- Items of Work For RoadsDocument6 pagesItems of Work For Roadsjhc1123No ratings yet
- Gynecological NursingDocument329 pagesGynecological Nursingsharon ocharaNo ratings yet
- Basic Labour Rate ListDocument6 pagesBasic Labour Rate ListmaheshNo ratings yet
- Evaluation and Management of Primary Amenorrhea - UpToDateDocument14 pagesEvaluation and Management of Primary Amenorrhea - UpToDateCristinaCaprosNo ratings yet
- AmenorrheaDocument11 pagesAmenorrheaDr.med SurduckiNo ratings yet
- Evaluation and Management of Primary Amenorrhea - UpToDateDocument11 pagesEvaluation and Management of Primary Amenorrhea - UpToDateNatasya SugiantoNo ratings yet
- Evaluation and Management of Primary AmenorrheaDocument11 pagesEvaluation and Management of Primary AmenorrheaLisa LestariNo ratings yet
- Absent or Irregular PeriodsDocument6 pagesAbsent or Irregular PeriodsEcbNo ratings yet
- No. 34. Management of Infertility Caused by Ovulatory DysfunctionDocument19 pagesNo. 34. Management of Infertility Caused by Ovulatory DysfunctionAnnisa JuwitaNo ratings yet
- 3current Evaluation of Amenorrhea - A Committee OpinionDocument9 pages3current Evaluation of Amenorrhea - A Committee Opinionjorge nnNo ratings yet
- Laboratory Evaluation of InfertilityDocument8 pagesLaboratory Evaluation of InfertilityOndape ValeryNo ratings yet
- AmenorrheaDocument40 pagesAmenorrheaMeraol HusseinNo ratings yet
- Amenorrhea WorkupDocument10 pagesAmenorrhea WorkupHaoKeat HoeNo ratings yet
- Pcos - Clinical Case DiscussionDocument4 pagesPcos - Clinical Case Discussionreham macadatoNo ratings yet
- Notes Infertility Delayed PubertyDocument9 pagesNotes Infertility Delayed PubertyTONY GO AWAYNo ratings yet
- Amenorrhea & Heavy Menstrual BleedingDocument22 pagesAmenorrhea & Heavy Menstrual BleedingJanesel Plariza PanerioNo ratings yet
- Raspa Infertility Final (Optimized)Document49 pagesRaspa Infertility Final (Optimized)Saya MenangNo ratings yet
- Amenorrhea - An Approach To Diagnosis and Management AFP 2013 PDFDocument8 pagesAmenorrhea - An Approach To Diagnosis and Management AFP 2013 PDFBabila CarvalhoNo ratings yet
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- AmenorrheaDocument13 pagesAmenorrheaJanesel Plariza PanerioNo ratings yet
- Athanasia Piouka, 1 Dimitrios Farmakiotis, 1 Ilias Katsikis, 1 Djuro Macut, 2 Spiros Gerou, 3 and Dimitrios Panidis1Document8 pagesAthanasia Piouka, 1 Dimitrios Farmakiotis, 1 Ilias Katsikis, 1 Djuro Macut, 2 Spiros Gerou, 3 and Dimitrios Panidis1Yosefin EkaNo ratings yet
- Polycystic Ovary Syndrome: A Review (Ricardo Azizz)Document3 pagesPolycystic Ovary Syndrome: A Review (Ricardo Azizz)Jeremy LickteigNo ratings yet
- Polycystic Ovarian SyndromeDocument19 pagesPolycystic Ovarian SyndromeAndreeaBiancaPuiuNo ratings yet
- 無月經症 Amenorrhea: Reporter: FM R1 余明謙 Supervisor: VS 張德宇Document38 pages無月經症 Amenorrhea: Reporter: FM R1 余明謙 Supervisor: VS 張德宇余明謙No ratings yet
- Pcos StudiesDocument34 pagesPcos StudiesDoctora SantanaNo ratings yet
- Diagnostic Evaluation of Polycystic Ovary Syndrome in Adolescents - UpToDateDocument31 pagesDiagnostic Evaluation of Polycystic Ovary Syndrome in Adolescents - UpToDateRICO NOVYANTONo ratings yet
- Polycystic Ovary Syndrome: Dr. Rizwana ShaheenDocument34 pagesPolycystic Ovary Syndrome: Dr. Rizwana ShaheenAmaan Hakim100% (1)
- Secamenhyper 120208102817 Phpapp02Document31 pagesSecamenhyper 120208102817 Phpapp02Mohan DassNo ratings yet
- AmennorheaDocument14 pagesAmennorheakutra3000No ratings yet
- Polycystic Ovarian SyndromeDocument32 pagesPolycystic Ovarian SyndromeRaras MayangNo ratings yet
- PcosDocument9 pagesPcosMonomay HalderNo ratings yet
- Emedicine Hypersemesis GravidarumDocument26 pagesEmedicine Hypersemesis GravidarumAnonymous 3OoumAUytNo ratings yet
- Polycystic Ovary Syndrome: Adam BalenDocument14 pagesPolycystic Ovary Syndrome: Adam BalenRufino Guarniz CapristanNo ratings yet
- What Is AmenorrheaDocument5 pagesWhat Is AmenorrheaYhoyho Akhilun Dewa MimpiNo ratings yet
- Hyperandrogenism: Arrest Occurs When The Granulosa Cells of The Ovaries Normally Begin To ProduceDocument7 pagesHyperandrogenism: Arrest Occurs When The Granulosa Cells of The Ovaries Normally Begin To ProduceNathan JeffreyNo ratings yet
- GROUP 3 LC AminoreDocument11 pagesGROUP 3 LC AminoreAAANo ratings yet
- Amenorrhea: Darren Farley, M.D. Department of Obstetrics and Gynecology UKSM-WichitaDocument13 pagesAmenorrhea: Darren Farley, M.D. Department of Obstetrics and Gynecology UKSM-WichitaFandy SetiawanNo ratings yet
- Study PCOS XDocument8 pagesStudy PCOS XdfdfffffNo ratings yet
- Pathogenesis of PcosDocument14 pagesPathogenesis of PcosMitali Narurkar100% (1)
- SDII 42 Phy Polycystic Ovary SyndromeDocument48 pagesSDII 42 Phy Polycystic Ovary SyndromeRodrick StoneNo ratings yet
- Basic Infertility EvaluationDocument13 pagesBasic Infertility EvaluationRosu GeorgeNo ratings yet
- Menstrual Disorders 2Document39 pagesMenstrual Disorders 2Nanang HidayatullohNo ratings yet
- Polycystic Ovarian SyndromeDocument20 pagesPolycystic Ovarian SyndromeMuhammad khairul afizal RohimNo ratings yet
- Amen or RheaDocument34 pagesAmen or RheaAsma Naseer CheemaNo ratings yet
- Ovario Poliquístico/Polycystic Ovary SyndromeDocument14 pagesOvario Poliquístico/Polycystic Ovary SyndromeJosé María Lauricella100% (1)
- Amenorrhea: Evaluation & Treatment: Jurnal Reading Mohamad Athaullah 11.2012.062Document28 pagesAmenorrhea: Evaluation & Treatment: Jurnal Reading Mohamad Athaullah 11.2012.062Athaullah IsmailNo ratings yet
- 5f33a63892ff020200812article - PDF - FileStep-up Protocol Versus Conventional Dosage of Letrozole For Ovulation Induction in Women With PCOSDocument4 pages5f33a63892ff020200812article - PDF - FileStep-up Protocol Versus Conventional Dosage of Letrozole For Ovulation Induction in Women With PCOSAhmed AnwarNo ratings yet
- Guideline On Induction of Ovulation 2011Document20 pagesGuideline On Induction of Ovulation 2011Atik ShaikhNo ratings yet
- Management Ectopic Pregnancy SLCOGDocument9 pagesManagement Ectopic Pregnancy SLCOGMelissa Aina Mohd YusofNo ratings yet
- Assesment of Amen or RheaDocument49 pagesAssesment of Amen or Rheakhadzx100% (2)
- Clinical CaseDocument10 pagesClinical CaseCristy RomeroNo ratings yet
- Recurrent Pregnancy Loss - Management - UpToDateDocument19 pagesRecurrent Pregnancy Loss - Management - UpToDateJean CarlosNo ratings yet
- Lecture 20 Hormones and Infertility LectureDocument48 pagesLecture 20 Hormones and Infertility LectureJoseph Stans KasiryeNo ratings yet
- AE240 Notes Early-Airfoil-Development-Handout-1Document5 pagesAE240 Notes Early-Airfoil-Development-Handout-1mohamedNo ratings yet
- MSC in Subsea Engineering - Flexible Pipe Analysis Lecture JP 2023Document67 pagesMSC in Subsea Engineering - Flexible Pipe Analysis Lecture JP 2023Fakey LaazNo ratings yet
- Compteur 7757 - A PDFDocument16 pagesCompteur 7757 - A PDFbromartNo ratings yet
- CekocideDocument1 pageCekocideKaren Claire HorcaNo ratings yet
- s1160 Jorvet Infusion PumpDocument4 pagess1160 Jorvet Infusion PumpGhulam HyderNo ratings yet
- January 2005 6677 Mechanics M1: Mark SchemeDocument7 pagesJanuary 2005 6677 Mechanics M1: Mark SchemeWael TareqNo ratings yet
- RymesDocument6 pagesRymesFarida YesminNo ratings yet
- MAIN Electrical Parts List: Design LOC Sec-Code DescriptionDocument12 pagesMAIN Electrical Parts List: Design LOC Sec-Code DescriptionAndroid Schematics and CircuitsNo ratings yet
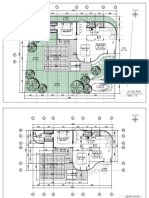
- 2023.01.25 Plan Pecatu Villa - FinishDocument3 pages2023.01.25 Plan Pecatu Villa - FinishTika AgungNo ratings yet
- Falsework For Concrete Structures - Guidelines: Indian StandardDocument24 pagesFalsework For Concrete Structures - Guidelines: Indian StandardLivinston JosephNo ratings yet
- Consola Phonic CELEUS800 en EspañolDocument32 pagesConsola Phonic CELEUS800 en EspañolRoberto BurgosNo ratings yet
- BCA 5005 Minor Project Synopsis Format & GuidelinesDocument7 pagesBCA 5005 Minor Project Synopsis Format & GuidelinesAnu VermaNo ratings yet
- Our Changing WorldDocument3 pagesOur Changing Worlddinesh869863% (8)
- Ps 0412 0612obh WDocument1 pagePs 0412 0612obh WHunterNo ratings yet
- Basic Concepts of SociologyDocument4 pagesBasic Concepts of SociologyAiman HaiqarlNo ratings yet
- Group 3 Aia ReportDocument26 pagesGroup 3 Aia ReportNAVAS E VNo ratings yet