You might also like
- Solution Manual For Digital Control System Analysis and Design 4th Edition by Phillips ISBN 0132938316 9780132938310Document36 pagesSolution Manual For Digital Control System Analysis and Design 4th Edition by Phillips ISBN 0132938316 9780132938310jenniferwatersgbrcixdmzt96% (24)
- ECG-EKG Presentation - Gunda GDocument21 pagesECG-EKG Presentation - Gunda GGadzikaNo ratings yet
- Management of Patients With Dysrhythmias and Conduction Problems Dr. SydioncoDocument15 pagesManagement of Patients With Dysrhythmias and Conduction Problems Dr. SydioncoRoyce Vincent Tizon100% (1)
- PacemakerDocument63 pagesPacemakerMonish RautNo ratings yet
- EKG Study GuideDocument45 pagesEKG Study GuideBrawner100% (6)
- Project Report On BananaDocument64 pagesProject Report On Bananaapi-2695636194% (18)
- L3.2 - IM - Correlated Lecture Dr. BJC (Sept0922)Document6 pagesL3.2 - IM - Correlated Lecture Dr. BJC (Sept0922)Maria Carmela CastilloNo ratings yet
- Basic EKG InterpretationDocument48 pagesBasic EKG InterpretationAimee Ann Pauco MacaraegNo ratings yet
- ECGs The Basics (Part 1) LectureDocument32 pagesECGs The Basics (Part 1) Lectureliudmyla zakordonetsNo ratings yet
- ECGs The Basics (Part 1) LectureDocument33 pagesECGs The Basics (Part 1) Lectureliudmyla zakordonetsNo ratings yet
- Unit 8 PresentationDocument34 pagesUnit 8 Presentation03152788No ratings yet
- Ekg PsikDocument69 pagesEkg PsikZEISVA APRILIANINGRUMNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- Electrocardiogram: By: Keverne Jhay P. Colas, RN, MANDocument72 pagesElectrocardiogram: By: Keverne Jhay P. Colas, RN, MANGaras AnnaBerniceNo ratings yet
- Special Conductive System of Heart: By: Azher SyedDocument14 pagesSpecial Conductive System of Heart: By: Azher SyedAzhersyedNo ratings yet
- Group 4 - Baseline Heart Rate & EcgDocument38 pagesGroup 4 - Baseline Heart Rate & EcgTimothy John Bautista100% (2)
- ECG ECG Basics Presentation 201309101527422446 PDFDocument45 pagesECG ECG Basics Presentation 201309101527422446 PDFRamesh RajNo ratings yet
- Basic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNDocument34 pagesBasic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNMavic Martinez BuntalesNo ratings yet
- Electrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosisDocument38 pagesElectrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosislorhenzsoNo ratings yet
- Trinity CVS Lecture 1-ECG 12.13.Ppt (Read-Only)Document24 pagesTrinity CVS Lecture 1-ECG 12.13.Ppt (Read-Only)cystanarisaNo ratings yet
- Ecg Treadmill and Holter TestDocument77 pagesEcg Treadmill and Holter TestRiteka Singh100% (1)
- MUCLecture 2021 1292271Document34 pagesMUCLecture 2021 1292271Kouka MahfoudiNo ratings yet
- Ecg in ExDocument70 pagesEcg in ExLakshmi PrasannaNo ratings yet
- Disrythmia Recognition ACLS ASHIDocument127 pagesDisrythmia Recognition ACLS ASHIJulisa FernandezNo ratings yet
- Chapter 23 Management of Patients With Dysrhythmias and Conduction ProblemsDocument64 pagesChapter 23 Management of Patients With Dysrhythmias and Conduction Problemsسلطان محمد فوزي سلمانNo ratings yet
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- ECG Placement Final DLSL - DDocument44 pagesECG Placement Final DLSL - DAlma Janella TOSINONo ratings yet
- Electro Cardiograph yDocument94 pagesElectro Cardiograph ykajonasfoodproductsNo ratings yet
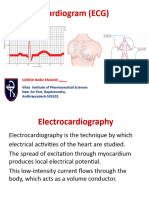
- Electrocardiogram (ECG)Document53 pagesElectrocardiogram (ECG)eric100% (1)
- Basic Ecg Interpretation & Procedure: BY: Ahmad Hafiz Bin Alias Universuty Lecturer UniszaDocument26 pagesBasic Ecg Interpretation & Procedure: BY: Ahmad Hafiz Bin Alias Universuty Lecturer UniszaLogadarshini VeerasamyNo ratings yet
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDocument102 pagesElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNo ratings yet
- Electro PhysiologyDocument108 pagesElectro PhysiologyGUTIERREZ, CRISHA ANDREA M.No ratings yet
- Ecg or Electro Cardiogram and ElectrocardiographDocument20 pagesEcg or Electro Cardiogram and ElectrocardiographsureshNo ratings yet
- UntitledDocument4 pagesUntitledmostafa5050No ratings yet
- DrAbnet ECG - BasicsDocument99 pagesDrAbnet ECG - BasicsAbnet WondimuNo ratings yet
- Tomasz WikarekDocument95 pagesTomasz Wikareknamar13766No ratings yet
- 321 Lecture ECGDocument38 pages321 Lecture ECGCea Mikee Mitch BartolomeNo ratings yet
- Electrocardiogram (Ecg/Ekg) : Presented By: Elgeene E. DizonDocument41 pagesElectrocardiogram (Ecg/Ekg) : Presented By: Elgeene E. DizonElgeene DizonNo ratings yet
- ECG 22septDocument53 pagesECG 22septA ScribbbNo ratings yet
- Topic:: Performing and Interpreting Electrocardiogram (ECG)Document137 pagesTopic:: Performing and Interpreting Electrocardiogram (ECG)Tiffany AdriasNo ratings yet
- Conducting System of The HeartDocument27 pagesConducting System of The HeartMuhammadNo ratings yet
- Santosh DevDocument45 pagesSantosh Devdevdsantosh100% (1)
- Electrical Activity of The HeartDocument156 pagesElectrical Activity of The HeartNIRANJANA SHALININo ratings yet
- ECG Complete LectureDocument33 pagesECG Complete LectureDr. SUVA NATHNo ratings yet
- Basic ElectrophysiologyDocument46 pagesBasic Electrophysiologyiin setiyanaNo ratings yet
- ElectrocardiographyDocument4 pagesElectrocardiographyJho BuanNo ratings yet
- ElectrocardiogramSignalAnalysis-An OverviewDocument5 pagesElectrocardiogramSignalAnalysis-An OverviewLejla AkšamovićNo ratings yet
- Electrophysiologyofheart PDFDocument99 pagesElectrophysiologyofheart PDFsahar awaisNo ratings yet
- Week02 Measurement ToolsDocument57 pagesWeek02 Measurement ToolsKhalil AbuhantashNo ratings yet
- Mechanical and Electrical Events of The Cardiac CycleDocument39 pagesMechanical and Electrical Events of The Cardiac CyclebhatsindhoorNo ratings yet
- Unit 1Document29 pagesUnit 1SasikumarNo ratings yet
- Dysrythmia Review For Pre TestDocument29 pagesDysrythmia Review For Pre TestGeena sekhonNo ratings yet
- Electrocardioghraphy ECG/ (EKG) : ZTG PHR 327 Fall 2019Document17 pagesElectrocardioghraphy ECG/ (EKG) : ZTG PHR 327 Fall 2019mujNo ratings yet
- Permanent Pacemaker: Supervisor: DR Pipin Ardhianto SPJP (K), FihaDocument67 pagesPermanent Pacemaker: Supervisor: DR Pipin Ardhianto SPJP (K), Fihapelantikan ppnirsdkNo ratings yet
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- Electrocardiogram: Clinical Skills III NYIT Physician Assistant StudiesDocument36 pagesElectrocardiogram: Clinical Skills III NYIT Physician Assistant StudiesasdfgrtttNo ratings yet
- Basic of ECG: Prepared By: Zahid HussainDocument38 pagesBasic of ECG: Prepared By: Zahid HussainZahid Hussain100% (1)
- Ecg PrsentationDocument33 pagesEcg Prsentationtehillahkabwe100No ratings yet
- ECG ECG Basics PresentationDocument45 pagesECG ECG Basics PresentationLan Anh Pham100% (1)
- Aritmii EngDocument90 pagesAritmii EngAnna HaritonencoNo ratings yet
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Human Body Systems For KidsDocument12 pagesHuman Body Systems For Kidsnk20No ratings yet
- Shallow Lakes 2002Document309 pagesShallow Lakes 2002testvietnamNo ratings yet
- Environmental Science Q1 Week 2 3Document23 pagesEnvironmental Science Q1 Week 2 3Anonymous gV9BmXXHNo ratings yet
- Food Deterioration and Its ControlDocument3 pagesFood Deterioration and Its Controlansar ali100% (3)
- Ajcr0008 2436Document21 pagesAjcr0008 2436louisehip UFCNo ratings yet
- Reading ToeflDocument7 pagesReading ToeflAlessia SMNo ratings yet
- Biology Sem 1 Exam PapersqDocument13 pagesBiology Sem 1 Exam Papersqpc usageNo ratings yet
- 2012 OpenExam AnsKeyDocument11 pages2012 OpenExam AnsKeymartynapetNo ratings yet
- NCERT Class 12 BiologyDocument311 pagesNCERT Class 12 Biologynaveen reddy100% (1)
- Solving Cold Cases With DNA Boston Strangler CaseDocument3 pagesSolving Cold Cases With DNA Boston Strangler CasePranjal SinghalNo ratings yet
- Evaluation of Imbred Lines Derived FromDocument9 pagesEvaluation of Imbred Lines Derived FromManuel GuzmanNo ratings yet
- Land Resources: Use For Prosperity, Save For Posterity: Activity Guide Book For NCSC 2010 - 2011 (Draft)Document50 pagesLand Resources: Use For Prosperity, Save For Posterity: Activity Guide Book For NCSC 2010 - 2011 (Draft)Aditya NatekarNo ratings yet
- Bioceramic Sealer ReviewDocument11 pagesBioceramic Sealer ReviewArdelia RaissaNo ratings yet
- JetoptimusDocument7 pagesJetoptimusShubh YouTubeNo ratings yet
- Class 8-Question Paper 2022Document8 pagesClass 8-Question Paper 2022Vicky VermaNo ratings yet
- Lesson 1:introduction To The Ocean SciencesDocument24 pagesLesson 1:introduction To The Ocean SciencesgfhjNo ratings yet
- 1) New Standards For Neutral Thermal Environment ofDocument5 pages1) New Standards For Neutral Thermal Environment ofroselNo ratings yet
- BCH 332 Lectures 1 and 2 0Document33 pagesBCH 332 Lectures 1 and 2 0asdNo ratings yet
- 18btc101j Biochem-Unit 1Document134 pages18btc101j Biochem-Unit 1nikteshgNo ratings yet
- 2014 MBAA Chris White Yeast ManagementDocument30 pages2014 MBAA Chris White Yeast ManagementAdrián LampazziNo ratings yet
- CNS - Important QuestionsDocument2 pagesCNS - Important Questionsavantika rajeev100% (3)
- Plant and Animal Organ System and Their FunctionsDocument28 pagesPlant and Animal Organ System and Their FunctionsJohn Michael Lopez100% (1)
- Tutorial W4 SCES3373Document5 pagesTutorial W4 SCES3373PRBMSK50622 Mathilda Durie Anak RowneyNo ratings yet
- Self Reflection MammalsDocument1 pageSelf Reflection Mammalsapi-319897202No ratings yet
- Lecture10 CompetitiveLearningDocument17 pagesLecture10 CompetitiveLearningBongkyu JeonNo ratings yet
- Detoxifiere Mercur Etc-GhidDocument175 pagesDetoxifiere Mercur Etc-GhidRadulescu EugenNo ratings yet
- Biology Module 5 NotesDocument17 pagesBiology Module 5 NotesKatie BellNo ratings yet
- EngDocument14 pagesEnganjuNo ratings yet