You might also like
- Joe Iwanaga, R. Shane Tubbs - Atlas of Oral and Maxillofacial Anatomy-Springer (2021)Document170 pagesJoe Iwanaga, R. Shane Tubbs - Atlas of Oral and Maxillofacial Anatomy-Springer (2021)duymerNo ratings yet
- Endometrial PolypsDocument14 pagesEndometrial PolypsMusaNo ratings yet
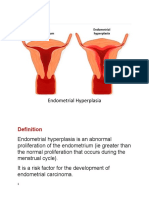
- Abnormalities of The EndometriumDocument3 pagesAbnormalities of The EndometriumDymas R SyahputraNo ratings yet
- Endometrial Polyps: DR Philip ThomasDocument4 pagesEndometrial Polyps: DR Philip Thomasapache_sp2208465No ratings yet
- Pathophysiology: Each Month, Normally Functioning Ovaries Develop SmallDocument9 pagesPathophysiology: Each Month, Normally Functioning Ovaries Develop SmallAl-nazer Azer Al100% (1)
- EndometriosisDocument46 pagesEndometriosisManoj Ranadive0% (1)
- Tinjauan PustakaDocument5 pagesTinjauan PustakaTheresa EvansNo ratings yet
- OB-GYN 101: Uterine LeiomyomaDocument3 pagesOB-GYN 101: Uterine Leiomyomamadmax500No ratings yet
- Endometrial Polyps: Irregular Menstrual BleedingDocument4 pagesEndometrial Polyps: Irregular Menstrual BleedingLuke ObusanNo ratings yet
- Myoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDocument3 pagesMyoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDiane MargretNo ratings yet
- 03 JCR 004 Rajendra EndometrialDocument4 pages03 JCR 004 Rajendra EndometrialReza HidayatNo ratings yet
- DR Sankalpa R WankhedeDocument76 pagesDR Sankalpa R Wankhedechaitanya suryawanshiNo ratings yet
- Benign Lesions of The OvariesDocument12 pagesBenign Lesions of The OvariesdocjosmaNo ratings yet
- Endometrial MalignancyDocument8 pagesEndometrial MalignancySusmita HalderNo ratings yet
- Deep Infiltrating Endometriosis: Symptoms and Diagnostic Procedures. The Symptoms As Well As Clinical FindingsDocument5 pagesDeep Infiltrating Endometriosis: Symptoms and Diagnostic Procedures. The Symptoms As Well As Clinical FindingsBunga JuwitaNo ratings yet
- Keywords: Endometrial Polyp, Endometrioma, Ovarian Cyst, Ovarian Dermoid, PelvicDocument13 pagesKeywords: Endometrial Polyp, Endometrioma, Ovarian Cyst, Ovarian Dermoid, PelvicWarrodNo ratings yet
- Breast Diseases BenignDocument34 pagesBreast Diseases BenignAhmad Uzair QureshiNo ratings yet
- Ovarian Cysts: Functional Cysts and Are Always BenignDocument9 pagesOvarian Cysts: Functional Cysts and Are Always BenignElvisNo ratings yet
- Fibroid General InfoDocument6 pagesFibroid General InfoDurosawo Adeolu TimothyNo ratings yet
- For Uterine Polyps. Racheal RaiDocument15 pagesFor Uterine Polyps. Racheal RaiChinju Jose SajithNo ratings yet
- Benign Gynecological LesionsDocument9 pagesBenign Gynecological LesionsLanceNo ratings yet
- ARC Fertility Articles: Surgical Advances in Fertility TreatmentDocument2 pagesARC Fertility Articles: Surgical Advances in Fertility TreatmentBryan MorteraNo ratings yet
- ANDI DR Louis Jordaan - 2Document9 pagesANDI DR Louis Jordaan - 2aprooolNo ratings yet
- College of Medicine: Department of General SurgeryDocument53 pagesCollege of Medicine: Department of General SurgeryAbdullah EssaNo ratings yet
- Presentation 1Document20 pagesPresentation 1Mohamad HafyfyNo ratings yet
- ADENOMYOSISDocument5 pagesADENOMYOSISdoddydrNo ratings yet
- HysterosDocument17 pagesHysterosAnto PopaNo ratings yet
- Uterine FibroidDocument46 pagesUterine FibroidAfiqi FikriNo ratings yet
- Cervical PolypsDocument16 pagesCervical Polypstitusrop10No ratings yet
- EndometriosisDocument4 pagesEndometriosisAno DzamelashviliNo ratings yet
- Endometriosis O&g PresentationDocument31 pagesEndometriosis O&g PresentationChauthiran Agamudaiyar100% (1)
- Cervical Polyps - Causes - Symptoms - Management - TeachMeObGynDocument2 pagesCervical Polyps - Causes - Symptoms - Management - TeachMeObGynmohanNo ratings yet
- Management of Benign Breast Conditions: Part 2 - Breast Lumps and LesionsDocument3 pagesManagement of Benign Breast Conditions: Part 2 - Breast Lumps and Lesionspeter_mrNo ratings yet
- Uterus: Case Scenario 1 1. Physiology of Irregular Menses?Document3 pagesUterus: Case Scenario 1 1. Physiology of Irregular Menses?Artika MalaNo ratings yet
- UMS Short and Long CaseDocument116 pagesUMS Short and Long CaseRosniza RosliNo ratings yet
- Histeroscopy 8Document16 pagesHisteroscopy 8Silvia IzvoranuNo ratings yet
- Uterine Fibroids PDFDocument3 pagesUterine Fibroids PDFmervat_aastNo ratings yet
- Cervical Polyp 12345Document13 pagesCervical Polyp 12345Osama Edris Hama SamanNo ratings yet
- Benign Ovarian TumoursDocument82 pagesBenign Ovarian TumoursHeena ChawlaNo ratings yet
- EndometrisisDocument10 pagesEndometrisisAmmarNo ratings yet
- Case Study-Endometrial PyometraDocument7 pagesCase Study-Endometrial Pyometrasimbarashe tangwadzanaNo ratings yet
- Dapus 4Document4 pagesDapus 4Ressy IrmaNo ratings yet
- Cervicalpolyp 12345Document14 pagesCervicalpolyp 12345faikaoesmaniaNo ratings yet
- Adnexal Masses in PregnancyDocument49 pagesAdnexal Masses in Pregnancysudheshna gattemNo ratings yet
- Benign Ovarian Tumors-1Document45 pagesBenign Ovarian Tumors-1abdulghani100% (1)
- Endoscopy in Infertility Work Up at Genesis Fertility Center, KalyanDocument3 pagesEndoscopy in Infertility Work Up at Genesis Fertility Center, KalyanMayuri SwamiNo ratings yet
- Benign Tumours of The Ovary-Dr. RabiuDocument34 pagesBenign Tumours of The Ovary-Dr. Rabiuijojo elizabeth100% (1)
- Case Conference NICHOLASDocument9 pagesCase Conference NICHOLASagathapradanaNo ratings yet
- JR - Cervical PolypDocument5 pagesJR - Cervical PolypHafidz Aryan AbdillahNo ratings yet
- Adeno Related LitDocument2 pagesAdeno Related Litflorence zemogNo ratings yet
- Endoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and ComplicationsDocument16 pagesEndoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and Complicationsselatur100% (1)
- Uterine Leiomyoma and Benign Ovarian Tumors 24.8.2022 PDFDocument48 pagesUterine Leiomyoma and Benign Ovarian Tumors 24.8.2022 PDFZayNo ratings yet
- Ndometriosis: A Guide For PatientsDocument16 pagesNdometriosis: A Guide For PatientsYusran AchmadNo ratings yet
- Benign Gyne LesionsDocument133 pagesBenign Gyne LesionsJulie Ann ValenciaNo ratings yet
- EndometriosisDocument5 pagesEndometriosisLok100% (2)
- Dilatation and Curettage: James S. Krieger, M.D. Department of GynecologyDocument4 pagesDilatation and Curettage: James S. Krieger, M.D. Department of GynecologyCzarina Mae Quinones TadeoNo ratings yet
- Abnormal Uterine BleedingDocument39 pagesAbnormal Uterine BleedingVincentiusNo ratings yet
- The Management of Uterine Leiomyomas: DR .Ashraf FoudaDocument158 pagesThe Management of Uterine Leiomyomas: DR .Ashraf Foudakhadzx100% (2)
- ENDOMETRIOSISDocument17 pagesENDOMETRIOSISPeterson Wachira HscNo ratings yet
- Arellano University: Jose Abad Santos CampusDocument7 pagesArellano University: Jose Abad Santos CampusLloyd VargasNo ratings yet
- Information From The British Association of Urological Surgeons (BAUS) About Bladder CathetersDocument6 pagesInformation From The British Association of Urological Surgeons (BAUS) About Bladder CathetersralphholingsheadNo ratings yet
- FadenDocument5 pagesFadenbonny_07_fk_unsri9248No ratings yet
- Case Study HydrocephalusDocument19 pagesCase Study HydrocephalusJane Mae JesoroNo ratings yet
- Thoracic Surgery ManualDocument63 pagesThoracic Surgery ManualAhmed Abd El HamedNo ratings yet
- Day Care SummaryDocument4 pagesDay Care SummaryVijay SharmaNo ratings yet
- Nasopalatine Nerve BlockDocument29 pagesNasopalatine Nerve Blockoutright RohitNo ratings yet
- Koropenko Etd MiniposterDocument1 pageKoropenko Etd Miniposterapi-246574942No ratings yet
- HESI Exam PracticeDocument33 pagesHESI Exam PracticeJean AustenNo ratings yet
- 12 Lead Ecg PlacementsDocument2 pages12 Lead Ecg PlacementsShaina FukamiNo ratings yet
- Chest Trauma 2017 PDFDocument96 pagesChest Trauma 2017 PDFDeomicah SolanoNo ratings yet
- اسئله جراحه مدققه تDocument3 pagesاسئله جراحه مدققه تEba'a GamilNo ratings yet
- Branchial Cleft CystDocument6 pagesBranchial Cleft CystIvana SupitNo ratings yet
- Artikel Nama Medis DhionDocument2 pagesArtikel Nama Medis DhionDhion HernandoNo ratings yet
- Enema: Prepared By: Lourdes C. Lumba-Bacuyag RN, MANDocument27 pagesEnema: Prepared By: Lourdes C. Lumba-Bacuyag RN, MANkallin_10No ratings yet
- Extubation CriteriaDocument17 pagesExtubation CriteriaOliver TabagNo ratings yet
- Essay 3 Draft 2Document4 pagesEssay 3 Draft 2api-643529353No ratings yet
- Case Report Surgical Management of Lumbal Compression FractureDocument8 pagesCase Report Surgical Management of Lumbal Compression FractureYustinusrobbyNo ratings yet
- Anesthesia For Orthopedic SurgeryDocument27 pagesAnesthesia For Orthopedic Surgeryjeremy_raineyNo ratings yet
- Combine Bladder Irrigation Post Mortem Special MouthDocument88 pagesCombine Bladder Irrigation Post Mortem Special MouthJannen CasasNo ratings yet
- Postpartum Hemorrhage HandoutDocument3 pagesPostpartum Hemorrhage HandoutHarvey T. Dato-onNo ratings yet
- Resume Mina GhazaviDocument2 pagesResume Mina Ghazavimohammadrezahajian12191No ratings yet
- Epidural AnesthesiaDocument5 pagesEpidural AnesthesiaImran MukhlessNo ratings yet
- Perineum RepairDocument5 pagesPerineum RepairYwagar Ywagar100% (1)
- Administration of An Enema: Prepared By: Salwa MaghrabiDocument16 pagesAdministration of An Enema: Prepared By: Salwa MaghrabiAnonymous 1EoKWlNo ratings yet
- BT 2023153Document2 pagesBT 2023153Indiana Family to FamilyNo ratings yet
- Rec To Vaginal Fistula RepairDocument7 pagesRec To Vaginal Fistula Repairnaftalina7No ratings yet
- Wound Drain FinalDocument16 pagesWound Drain Finaljosephnoon1100% (1)
- Upper Airway Hypoglossal Nerve Stimulation - 2019 - Atlas of The Oral and MaxiDocument6 pagesUpper Airway Hypoglossal Nerve Stimulation - 2019 - Atlas of The Oral and Maxilaljadeff12No ratings yet