You might also like
- EndometriosisDocument46 pagesEndometriosisManoj Ranadive0% (1)
- EndometriosisDocument5 pagesEndometriosisLok100% (2)
- Treating EndometriosisDocument67 pagesTreating EndometriosisAbegail IbañezNo ratings yet
- Endometri Osis: Par Khmermedical StudyDocument18 pagesEndometri Osis: Par Khmermedical StudyLeang KarichakNo ratings yet
- Impey Obs and Gynae Revision Notes PDFDocument9 pagesImpey Obs and Gynae Revision Notes PDFRoiseNo ratings yet
- Adenomyosis Student PresentationDocument19 pagesAdenomyosis Student PresentationRae RayNo ratings yet
- Role of Laparoscopic Surgery in Endometriosis Associated Infertility - Literature ReviewDocument7 pagesRole of Laparoscopic Surgery in Endometriosis Associated Infertility - Literature ReviewFaza KahfiNo ratings yet
- Department of Prasuti Tantra and Striroga Dayanand Ayurvedic College, Jalandhar SESSION 2016-17Document40 pagesDepartment of Prasuti Tantra and Striroga Dayanand Ayurvedic College, Jalandhar SESSION 2016-17jyothiNo ratings yet
- Endometriosis: OccurrenceDocument6 pagesEndometriosis: Occurrencewea xczNo ratings yet
- OBGYN Revision NotesDocument9 pagesOBGYN Revision NotesJoanne Bowers100% (3)
- The Association Between Endometriomas and Ovarian Cancer: Preventive Effect of Inhibiting Ovulation and Menstruation During Reproductive LifeDocument10 pagesThe Association Between Endometriomas and Ovarian Cancer: Preventive Effect of Inhibiting Ovulation and Menstruation During Reproductive LifeMohamad Syaikhul IslamNo ratings yet
- Understanding AdenomyosisDocument6 pagesUnderstanding AdenomyosisAhmed AliNo ratings yet
- Endometrio I and Fertilit: ! C - F - E1!/ Y:R - !H Gajç '!Document2 pagesEndometrio I and Fertilit: ! C - F - E1!/ Y:R - !H Gajç '!Erik MirandaNo ratings yet
- ENDOMETRIOSISsDocument27 pagesENDOMETRIOSISsNouman HameedNo ratings yet
- Deep Infiltrating Endometriosis: Symptoms and Diagnostic Procedures. The Symptoms As Well As Clinical FindingsDocument5 pagesDeep Infiltrating Endometriosis: Symptoms and Diagnostic Procedures. The Symptoms As Well As Clinical FindingsBunga JuwitaNo ratings yet
- ENDOMETRIOSISDocument17 pagesENDOMETRIOSISPeterson Wachira HscNo ratings yet
- Treating Endometriosis with Chinese MedicineDocument8 pagesTreating Endometriosis with Chinese Medicineitsik12886No ratings yet
- EndometriomaDocument7 pagesEndometriomaErick Rafael AncaNo ratings yet
- EndometriosisDocument17 pagesEndometriosisIngrid HerreraNo ratings yet
- 1 GYNE 7 - EndometriosisDocument6 pages1 GYNE 7 - EndometriosisIrene FranzNo ratings yet
- Endometriosis PresentationDocument58 pagesEndometriosis PresentationBRI KUNo ratings yet
- Endometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument39 pagesEndometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDatefujimeisterNo ratings yet
- Endometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument42 pagesEndometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDateOrlando GuerraNo ratings yet
- Ndometriosis: A Guide For PatientsDocument16 pagesNdometriosis: A Guide For PatientsYusran AchmadNo ratings yet
- American FamilyDocument8 pagesAmerican FamilyrizkiaautikasariNo ratings yet
- BCC 2008Document5 pagesBCC 2008mesNo ratings yet
- Endometriosis & Adenomyosis: Understanding Causes, Symptoms and Treatment OptionsDocument25 pagesEndometriosis & Adenomyosis: Understanding Causes, Symptoms and Treatment Optionszaid alislamNo ratings yet
- Endometriosis Is A Common Disease in Women of Reproductive Age and IsDocument45 pagesEndometriosis Is A Common Disease in Women of Reproductive Age and IsSreekanth reddyNo ratings yet
- Womb Gynecological Endometrial Cells Uterine Cavity: Endometriosis (From Endo, "Inside", and Metra, "Document3 pagesWomb Gynecological Endometrial Cells Uterine Cavity: Endometriosis (From Endo, "Inside", and Metra, "remyavarghese25No ratings yet
- 14 Vol. 11 Issue 11 Nov 2020 IJPSR RE 3646Document7 pages14 Vol. 11 Issue 11 Nov 2020 IJPSR RE 3646Ehwanul HandikaNo ratings yet
- International Journal of Pharmaceutical Science Invention (IJPSI)Document3 pagesInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsNo ratings yet
- Laparoscopic Diagnosis of Endometriosis-Clinical Study: Henri Lahdemaki, Markku Santala, Markku RyynanenDocument5 pagesLaparoscopic Diagnosis of Endometriosis-Clinical Study: Henri Lahdemaki, Markku Santala, Markku Ryynanenfalon papalangiNo ratings yet
- Cervical PolypsDocument16 pagesCervical Polypstitusrop10No ratings yet
- Diagnosing and Treating Ovarian TorsionDocument8 pagesDiagnosing and Treating Ovarian TorsionSebastian GandyNo ratings yet
- From The Archives of The AFIP: Endometriosis: Radiologic-Pathologic CorrelationDocument24 pagesFrom The Archives of The AFIP: Endometriosis: Radiologic-Pathologic Correlation104022432 104a-No ratings yet
- Endometriosis and infertility: a literature reviewDocument17 pagesEndometriosis and infertility: a literature reviewiduy cantikNo ratings yet
- EndometriosisDocument4 pagesEndometriosisAno DzamelashviliNo ratings yet
- Endometriosis: Li Qi LingDocument67 pagesEndometriosis: Li Qi LingwaheedaNo ratings yet
- Differential Diagnosis of Common Gynecological Complaints - Sundhed - DKDocument7 pagesDifferential Diagnosis of Common Gynecological Complaints - Sundhed - DKPavel BerlinschiNo ratings yet
- Benign Lesions of The OvariesDocument12 pagesBenign Lesions of The OvariesdocjosmaNo ratings yet
- Makalah Rule of Ultrasound in Management of Uterine LeiomyomaDocument23 pagesMakalah Rule of Ultrasound in Management of Uterine LeiomyomaKristabella GianinaNo ratings yet
- Breast CancerDocument3 pagesBreast CancerPauline Salgado100% (1)
- Müllerian Agenesis Diagnosis and TreatmentDocument2 pagesMüllerian Agenesis Diagnosis and TreatmentMaulana DimasNo ratings yet
- 14 Abortion Noted PDFDocument37 pages14 Abortion Noted PDFmohammed farajiNo ratings yet
- EndometriosisDocument6 pagesEndometriosissalamredNo ratings yet
- Uterine Fibroids PDFDocument3 pagesUterine Fibroids PDFmervat_aastNo ratings yet
- Infert F - Endometriosis PDFDocument10 pagesInfert F - Endometriosis PDFJuan Sebastián ElcanoNo ratings yet
- Endometriosis Diagnosis, Symptoms, Stages and TreatmentDocument2 pagesEndometriosis Diagnosis, Symptoms, Stages and TreatmentApril Kirstin ChuaNo ratings yet
- Endometriosis and Adenomyosis: Bahaa MaliDocument40 pagesEndometriosis and Adenomyosis: Bahaa Mali'محمد علي' محمد لافيNo ratings yet
- Endometriosis: Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument41 pagesEndometriosis: Pathogenesis, Clinical Features, and Diagnosis - UpToDateRafael Vilano AvelarNo ratings yet
- Swatilekha Das (RN, MSN)Document20 pagesSwatilekha Das (RN, MSN)sandeepv08No ratings yet
- Primary Umbilical Endometriosis. Case Report and Discussion On Management OptionsDocument7 pagesPrimary Umbilical Endometriosis. Case Report and Discussion On Management Optionsari naNo ratings yet
- EndometriosisDocument50 pagesEndometriosisHannah Eloise MagsinoNo ratings yet
- Postmenopausal Bleeding - StatPearls - NCBI BooksDocument11 pagesPostmenopausal Bleeding - StatPearls - NCBI BooksKalaivathanan VathananNo ratings yet
- Swatilekha Das (RN, MSN)Document20 pagesSwatilekha Das (RN, MSN)sandeepv08No ratings yet
- 16.uterine Disorders (B.m.a)Document35 pages16.uterine Disorders (B.m.a)Jimmy MainaNo ratings yet
- Extra Pelvic Endometriosis: Double Ileal and Ileo-Caecal Localization Revealed by Acute Small Bowel Obstruction, A Clinical CaseDocument9 pagesExtra Pelvic Endometriosis: Double Ileal and Ileo-Caecal Localization Revealed by Acute Small Bowel Obstruction, A Clinical CaseIJAR JOURNALNo ratings yet
- ANDI Classification System Explains Benign Breast DisordersDocument9 pagesANDI Classification System Explains Benign Breast DisordersaprooolNo ratings yet
- ADENOMYOSISDocument5 pagesADENOMYOSISdoddydrNo ratings yet
- Endometriosis, A Simple Guide to The Condition, Treatment And Related DisordersFrom EverandEndometriosis, A Simple Guide to The Condition, Treatment And Related DisordersNo ratings yet
- Second Trimester MiscarriageDocument5 pagesSecond Trimester MiscarriageAmmarNo ratings yet
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
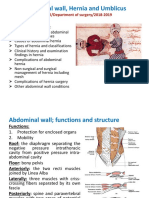
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Document46 pagesAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarNo ratings yet
- 22 - Postoperative Complications and Managament IIDocument39 pages22 - Postoperative Complications and Managament IIAmmarNo ratings yet
- Spleen Lec.2Document17 pagesSpleen Lec.2AmmarNo ratings yet
- Recurrent MiscarriageDocument9 pagesRecurrent MiscarriageAmmarNo ratings yet
- Bariatric and Metabolic SurgeryDocument32 pagesBariatric and Metabolic SurgeryAmmarNo ratings yet
- Spleen Lec.1Document30 pagesSpleen Lec.1AmmarNo ratings yet
- Menstrual cycle clinical considerationsDocument23 pagesMenstrual cycle clinical considerationsAmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- INVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTDocument5 pagesINVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTAmmarNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarNo ratings yet
- Polycystic Ovary Syndrome: Learning ObjectivesDocument8 pagesPolycystic Ovary Syndrome: Learning ObjectivesAmmarNo ratings yet
- Induced Abortion: Dr. Ali Murad Dr. Wassan NoriDocument12 pagesInduced Abortion: Dr. Ali Murad Dr. Wassan NoriAmmarNo ratings yet
- IntersexDocument10 pagesIntersexAmmarNo ratings yet
- Intracranial Mass DiagnosisDocument5 pagesIntracranial Mass DiagnosisAmmarNo ratings yet
- INVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTDocument5 pagesINVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTAmmarNo ratings yet
- 11 - Spinal Cord Injuries Lec.2Document4 pages11 - Spinal Cord Injuries Lec.2AmmarNo ratings yet
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- 7 - HydrocephalusDocument4 pages7 - HydrocephalusAmmarNo ratings yet
- 10 - Spinal Cord Injuries Lec.1Document7 pages10 - Spinal Cord Injuries Lec.1AmmarNo ratings yet
- 5 - Space Occupying LesionsDocument39 pages5 - Space Occupying LesionsAmmarNo ratings yet
- 9 - Spinal Cord InjuriesDocument61 pages9 - Spinal Cord InjuriesAmmarNo ratings yet
- 4 - Raised ICPDocument6 pages4 - Raised ICPAmmarNo ratings yet
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- Head Injury 2: (DR Mohamed A. J. Al Tamimi)Document10 pagesHead Injury 2: (DR Mohamed A. J. Al Tamimi)AmmarNo ratings yet
- Topic 9 ObsDocument7 pagesTopic 9 ObsHannan SyedNo ratings yet
- Classification of female genital anomaliesDocument1 pageClassification of female genital anomaliesDomnita UrsuNo ratings yet
- Multifetal GestationDocument22 pagesMultifetal GestationPaolo QuezonNo ratings yet
- The Gynaecological ExaminationDocument3 pagesThe Gynaecological ExaminationpogimudaNo ratings yet
- Perdarahan Uterus AbnormalDocument37 pagesPerdarahan Uterus AbnormalElno Tatipikalawan100% (1)
- Aub Updated-1 PDFDocument87 pagesAub Updated-1 PDFEvelyn Pamela Espinoza Morales100% (2)
- SNJune2009 SfinalDocument109 pagesSNJune2009 SfinalrickkolluriNo ratings yet
- Fetal Heart Monitoring AWHONN 15Document4 pagesFetal Heart Monitoring AWHONN 15Álvaro M. Luna CisnerosNo ratings yet
- Pengaruh Edukasi Online Berbasis Family Centered Dalam Pemberian Asi EksklusifDocument9 pagesPengaruh Edukasi Online Berbasis Family Centered Dalam Pemberian Asi EksklusifrisdawatiNo ratings yet
- Prof J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabweDocument17 pagesProf J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabwedanielNo ratings yet
- Adventures in Tandem NursingDocument3 pagesAdventures in Tandem NursingPesawaran VacationNo ratings yet
- METRORAGIADocument6 pagesMETRORAGIAMagda MagNo ratings yet
- Prenatal Care and Childbirth EducationDocument41 pagesPrenatal Care and Childbirth EducationEvan ChrissantaNo ratings yet
- Armando Menstrual CycleDocument2 pagesArmando Menstrual CycleMatthew PinedaNo ratings yet
- Ovulation and FertilizationDocument2 pagesOvulation and FertilizationEarl CopeNo ratings yet
- Bra Size Conversion ChartDocument3 pagesBra Size Conversion ChartTop Drawer Lingerie100% (1)
- Maternal and Child Health NursingDocument25 pagesMaternal and Child Health Nursingmarie100% (46)
- Science 10 - Activity 2 - 3rd Quarter - MontereyDocument2 pagesScience 10 - Activity 2 - 3rd Quarter - MontereyKiel Angelo MontereyNo ratings yet
- Maternity Record Keeping 4.0Document24 pagesMaternity Record Keeping 4.0ItaNo ratings yet
- Female Reproductive Anatomy GuideDocument33 pagesFemale Reproductive Anatomy GuideERIC ASAMAMLEH KLEMEHNo ratings yet
- Terminology in Clinical SettingDocument13 pagesTerminology in Clinical SettingCiuss ThamrinNo ratings yet
- Benign Lesions of The Ovary NotesDocument5 pagesBenign Lesions of The Ovary Notesmkct111No ratings yet
- 2019 Midwife CVDocument2 pages2019 Midwife CVapi-455508133No ratings yet
- Everything You Need to Know About Prenatal CareDocument5 pagesEverything You Need to Know About Prenatal Carelaura fernandiaNo ratings yet
- MessageDocument5 pagesMessageNikolae MarschallNo ratings yet
- FP TCLDocument2 pagesFP TCLlaliejhessNo ratings yet
- Comparative Study of Micronised Progesterone Versus ISOXSUPRINE IN THE PREVENTION OF PRETERM LABOURDocument7 pagesComparative Study of Micronised Progesterone Versus ISOXSUPRINE IN THE PREVENTION OF PRETERM LABOURshivareddychNo ratings yet
- Placenta PreviaDocument4 pagesPlacenta PreviaJeizel IgnacioNo ratings yet
- Quiz 9 Human Reproduction Pregnancy Menstruation GraphsDocument4 pagesQuiz 9 Human Reproduction Pregnancy Menstruation GraphsCamille FrancoNo ratings yet
- FHSIS report for Sampaloc BrgyDocument3 pagesFHSIS report for Sampaloc BrgyBe NjNo ratings yet