You might also like
- EndometriosisDocument46 pagesEndometriosisManoj Ranadive0% (1)
- Ectopic PregnancyDocument17 pagesEctopic Pregnancyapi-3700579No ratings yet
- EndometriosisDocument17 pagesEndometriosisapi-383379774No ratings yet
- Fibroid in Pregnancy: Characteristics, Complications, and ManagementDocument11 pagesFibroid in Pregnancy: Characteristics, Complications, and ManagementAnonymous UHnQSkxLBDNo ratings yet
- Endometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument39 pagesEndometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDatefujimeisterNo ratings yet
- Gynae and Obstetrics Nursing: 2 Year Post RN B.SC.N Mrs. Adeline Younas Topic: DysmenorrheaDocument17 pagesGynae and Obstetrics Nursing: 2 Year Post RN B.SC.N Mrs. Adeline Younas Topic: Dysmenorrheasajida adelineNo ratings yet
- Uterine Prolapse: Causes, Symptoms and TreatmentDocument39 pagesUterine Prolapse: Causes, Symptoms and Treatmentannu panchalNo ratings yet
- Menstrual DisorderDocument17 pagesMenstrual Disorderalisaa100% (1)
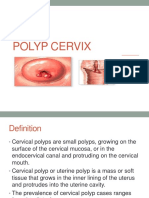
- Polyp CervixDocument14 pagesPolyp CervixT Horan100% (1)
- EndometriosisDocument29 pagesEndometriosisJohnnyDeepNo ratings yet
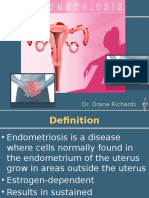
- Endometriosis Defined and Treatment OptionsDocument39 pagesEndometriosis Defined and Treatment OptionsOrane Richards100% (1)
- Dilation and curettage procedure overviewDocument15 pagesDilation and curettage procedure overviewnautilus81No ratings yet
- I. Dystocia: A. CausesDocument9 pagesI. Dystocia: A. CausesDianne GalangNo ratings yet
- Endometriosis: OccurrenceDocument6 pagesEndometriosis: Occurrencewea xczNo ratings yet
- Endometriosis PresentationDocument58 pagesEndometriosis PresentationBRI KUNo ratings yet
- Gyne History Taking PDFDocument6 pagesGyne History Taking PDFGokul AdarshNo ratings yet
- ADENOMYOSISDocument5 pagesADENOMYOSISdoddydrNo ratings yet
- 5 - Abortion or MiscarriageDocument43 pages5 - Abortion or Miscarriageasifdawar2011No ratings yet
- Obgyn HISTORY TAKING & EXAMINATIONDocument94 pagesObgyn HISTORY TAKING & EXAMINATIONvalentinemusa218100% (1)
- MenopauseDocument14 pagesMenopauseMizna SabillaNo ratings yet
- Indirect Inguinal Hernia FINALDocument6 pagesIndirect Inguinal Hernia FINALJonalyn TumanguilNo ratings yet
- Uterine Myoma CPDocument44 pagesUterine Myoma CPCristina L. JaysonNo ratings yet
- ENDOMETRITISDocument6 pagesENDOMETRITISKhrisna ParamaarthaNo ratings yet
- AbortionDocument121 pagesAbortionSindhu JojoNo ratings yet
- Fournier Gangrene Causes and AnatomyDocument16 pagesFournier Gangrene Causes and AnatomyAmirah Dahalan100% (1)
- Endometriosis (Complete)Document71 pagesEndometriosis (Complete)Justin Ng SincoNo ratings yet
- Ectopic PregnancyDocument46 pagesEctopic PregnancyNoegi AkasNo ratings yet
- Endometrial HyperplasiaDocument9 pagesEndometrial HyperplasiaMelissa Aina Mohd YusofNo ratings yet
- History Taking ObstetricDocument13 pagesHistory Taking ObstetricAnironOrion100% (7)
- Gynecology Course Overview for Nursing StudentsDocument104 pagesGynecology Course Overview for Nursing StudentsJean Pierre Hitimana100% (1)
- Ectopic PregnancyDocument3 pagesEctopic PregnancyMary Anne Yap100% (1)
- Uterine MyomaDocument15 pagesUterine Myomaanon_302623176100% (1)
- Obstetric History Taking - OSCE GuideDocument18 pagesObstetric History Taking - OSCE Guideabdalbaset100% (1)
- Obstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityDocument5 pagesObstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityBill HarmanNo ratings yet
- Management of Septic Abortion and ComplicationsDocument19 pagesManagement of Septic Abortion and Complicationsapi-370504683% (6)
- Pelvic InfectionsDocument56 pagesPelvic Infectionsvein94No ratings yet
- Ectopic PregnancyDocument5 pagesEctopic PregnancyFaith FuentevillaNo ratings yet
- EndometriosisDocument1 pageEndometriosisZiyad100% (1)
- Nodular Goiter Concept MapDocument5 pagesNodular Goiter Concept MapAllene PaderangaNo ratings yet
- Physical Assessment of The GentialiaDocument48 pagesPhysical Assessment of The GentialiaWilliam Lim100% (2)
- Physiological Changes of PregnancyDocument40 pagesPhysiological Changes of PregnancyAita AladianseNo ratings yet
- Malposition - Breech PresentationDocument133 pagesMalposition - Breech PresentationRadhakrishnan GovindanNo ratings yet
- Ectopic PregnancyDocument78 pagesEctopic PregnancyCarie Manarondong80% (5)
- Case Study-Ectopic PNDocument55 pagesCase Study-Ectopic PNArbie Jacinto100% (2)
- Obstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONDocument59 pagesObstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONmaezu100% (2)
- Uterine Fibroid - Viva VoceDocument77 pagesUterine Fibroid - Viva VoceK Haynes Raja100% (1)
- Hypertensive Disorders in Pregnancy (Williams 22 Edition)Document88 pagesHypertensive Disorders in Pregnancy (Williams 22 Edition)bagir_dm1067% (3)
- Ectopic Pregnancy Study GuideDocument5 pagesEctopic Pregnancy Study GuideCarl Elexer Cuyugan Ano100% (1)
- Abnormal Uterine BleedingDocument23 pagesAbnormal Uterine BleedingTakeru Ferry100% (1)
- Abnormal Uterine BleedingDocument4 pagesAbnormal Uterine BleedingAmellyn Reyes0% (1)
- HysterectomyDocument10 pagesHysterectomyjhodaneNo ratings yet
- EndometriosisDocument11 pagesEndometriosisKevin de SilvaNo ratings yet
- NSVDDocument32 pagesNSVDChris Oliver Kevin Ledesma100% (3)
- Benign and Malignant Ovarian Tumors (Gynaecology)Document70 pagesBenign and Malignant Ovarian Tumors (Gynaecology)Dr Ali MehdiNo ratings yet
- Swatilekha Das (RN, MSN)Document20 pagesSwatilekha Das (RN, MSN)sandeepv08No ratings yet
- LECTURE_EIGHT_CARE_ OF_WOMEN_WITH_ENDOMETRIOSISDocument22 pagesLECTURE_EIGHT_CARE_ OF_WOMEN_WITH_ENDOMETRIOSISOmar SanyangNo ratings yet
- Maternal Quiz 1Document59 pagesMaternal Quiz 1Teresa DumalagNo ratings yet
- EndometriosisDocument4 pagesEndometriosisAno DzamelashviliNo ratings yet
- Treating Endometriosis With The Integration of Traditional Chinese Medicine and Western MedicineDocument6 pagesTreating Endometriosis With The Integration of Traditional Chinese Medicine and Western MedicinedoeaNo ratings yet
- Endometriosis Diagnosis, Symptoms, Stages and TreatmentDocument2 pagesEndometriosis Diagnosis, Symptoms, Stages and TreatmentApril Kirstin ChuaNo ratings yet
- SUBMITTED BY Nahima Anhum SUBMITTED TO DR - Maimoona MSC - Microbiology 2 Semester University of HaripurDocument17 pagesSUBMITTED BY Nahima Anhum SUBMITTED TO DR - Maimoona MSC - Microbiology 2 Semester University of Haripursandeepv08No ratings yet
- Drugs Acting On G I System: Mr. Dipti SorteDocument65 pagesDrugs Acting On G I System: Mr. Dipti Sortesandeepv08No ratings yet
- Pharma Unit 3Document77 pagesPharma Unit 3sandeepv08No ratings yet
- CHW ManualDocument151 pagesCHW Manualsandeepv08No ratings yet
- Antiseptics & DisinfectantsDocument12 pagesAntiseptics & DisinfectantsMiguel MansillaNo ratings yet
- KMCT College of NursingDocument2 pagesKMCT College of Nursingsandeepv08No ratings yet
- Pharmacology: For Health Science StudentsDocument211 pagesPharmacology: For Health Science StudentssafibayNo ratings yet
- Antitubercular Drug: Dr. Deepak K GuptaDocument46 pagesAntitubercular Drug: Dr. Deepak K Guptasandeepv08No ratings yet
- GYNDocument3 pagesGYNsandeepv08No ratings yet
- Introduction To PharmacologyDocument45 pagesIntroduction To Pharmacologysandeepv08No ratings yet
- Benin LesionDocument14 pagesBenin Lesionsandeepv08No ratings yet
- Luther Gulick:: ControllingDocument52 pagesLuther Gulick:: Controllingsandeepv08No ratings yet
- Fourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric NursingDocument35 pagesFourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric Nursingsandeepv080% (1)
- New Text DocumentDocument1 pageNew Text Documentsandeepv08No ratings yet
- Q.P. CODE: 402010 Reg. No: ... Final Year B.SC Nursing Degree Examinations, September 2014 Management of Nursing Service and EducationDocument1 pageQ.P. CODE: 402010 Reg. No: ... Final Year B.SC Nursing Degree Examinations, September 2014 Management of Nursing Service and Educationsandeepv08No ratings yet
- Family Planning 2020 Commitment: Govt. of IndiaDocument3 pagesFamily Planning 2020 Commitment: Govt. of Indiasandeepv08No ratings yet
- Family Planning 2020 Commitment: Govt. of IndiaDocument3 pagesFamily Planning 2020 Commitment: Govt. of Indiasandeepv08No ratings yet
- CystoceleDocument4 pagesCystocelesandeepv08No ratings yet
- Fistula in Female Genital Tract .Document39 pagesFistula in Female Genital Tract .sandeepv08No ratings yet
- Fistula in Female Genital TractDocument40 pagesFistula in Female Genital Tractsandeepv08No ratings yet
- EndometriosisDocument6 pagesEndometriosissalamredNo ratings yet
- Nursing Management of Neonatal InfectionDocument19 pagesNursing Management of Neonatal Infectionsandeepv08No ratings yet
- Treat Cystocele with Surgery, Pessary or KegelsDocument7 pagesTreat Cystocele with Surgery, Pessary or Kegelssandeepv08No ratings yet
- Presented By-Mr. Yogesh A. DengaleDocument33 pagesPresented By-Mr. Yogesh A. Dengalesandeepv08No ratings yet
- Publc ReltnDocument15 pagesPublc Reltnsandeepv08No ratings yet
- Swatilekha Das (RN, MSN)Document20 pagesSwatilekha Das (RN, MSN)sandeepv08No ratings yet
- Information For You: Pelvic Organ ProlapseDocument8 pagesInformation For You: Pelvic Organ Prolapsesandeepv08No ratings yet
- Benin Lesion PDFDocument14 pagesBenin Lesion PDFsandeepv08No ratings yet
- Pre ND Post MGMNTDocument36 pagesPre ND Post MGMNTsandeepv08No ratings yet
- Congntl Anmls FRTDocument29 pagesCongntl Anmls FRTsandeepv08No ratings yet
- C612Document5 pagesC612dinhtung2210100% (1)
- English Sds Turalik 52Document13 pagesEnglish Sds Turalik 52Muhammad ArifudinNo ratings yet
- SimmonsDocument12 pagesSimmonsGürelBaltalıNo ratings yet
- Acp 22 9349 2022Document20 pagesAcp 22 9349 2022merlinakisNo ratings yet
- Ic M423GDocument2 pagesIc M423GSerikhi AliNo ratings yet
- PMBOK - Chapter 9: Project Human Resource ManagementDocument16 pagesPMBOK - Chapter 9: Project Human Resource Management7565006No ratings yet
- Preparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionDocument12 pagesPreparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionPaula NancyNo ratings yet
- World Bank ReportDocument14 pagesWorld Bank Reportaditya_erankiNo ratings yet
- Intro To GymnasticsDocument69 pagesIntro To GymnasticsMichaela Celerio50% (2)
- Filipino Nurses United OrientationDocument30 pagesFilipino Nurses United OrientationErlinda PosadasNo ratings yet
- Better - Call - Saul - 4x10 WINNERDocument70 pagesBetter - Call - Saul - 4x10 WINNERMarcos Valdés GarridoNo ratings yet
- Conveying Water Distribution SEODocument90 pagesConveying Water Distribution SEOmichelghanemNo ratings yet
- UNSG Report On Safety Security Humanitarian PersonnelDocument25 pagesUNSG Report On Safety Security Humanitarian PersonnelInterAction100% (1)
- Pensions Reforms at NSSFDocument4 pagesPensions Reforms at NSSFcliffmogere2348No ratings yet
- Pengaruh Ukuran Potongan Kopra Dalam Proses Pengeringan: Effect of The Copra Cut Size in The Drying ProcessDocument5 pagesPengaruh Ukuran Potongan Kopra Dalam Proses Pengeringan: Effect of The Copra Cut Size in The Drying ProcessAlexia Desi Ratnasari Loi 1841100210No ratings yet
- Testing Automotive/Industrial Composite Materials: Standard Guide ForDocument7 pagesTesting Automotive/Industrial Composite Materials: Standard Guide ForJuanNo ratings yet
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- Schlumber: Kevin: 16010072 Moch Rizky Setiawan: 16010068Document12 pagesSchlumber: Kevin: 16010072 Moch Rizky Setiawan: 16010068KevinNo ratings yet
- Paper 1Document8 pagesPaper 1Santhoshi Sadhanaa SankarNo ratings yet
- Science Activity Sheet Quarter 4 - MELC 2 Week 2: Uses of WaterDocument13 pagesScience Activity Sheet Quarter 4 - MELC 2 Week 2: Uses of WaterShareinne TeamkNo ratings yet
- 2.factory Price - Alarm Accessories-Complete 20150325Document15 pages2.factory Price - Alarm Accessories-Complete 20150325FREE BUSINESS INTELLIGENCENo ratings yet
- M&SDocument39 pagesM&Sgo.pushp70910% (1)
- Inside Out or Outside In. Meeting With Couples. Hugh JenkinsDocument24 pagesInside Out or Outside In. Meeting With Couples. Hugh JenkinsRita1976No ratings yet
- Septic Abortion PDFDocument4 pagesSeptic Abortion PDFmariachrismayaniNo ratings yet
- FD2000 DatasheetDocument2 pagesFD2000 DatasheetIvan MihajlovicNo ratings yet
- Edwards Auto 306 CharacteristicsDocument4 pagesEdwards Auto 306 CharacteristicsJuan Antonio Rubio-LaraNo ratings yet
- Answers To Extra PracticeDocument5 pagesAnswers To Extra PracticesaraNo ratings yet
- Celecoxib Identification MethodsDocument5 pagesCelecoxib Identification Methodsabc1679No ratings yet
- Project 3 - Gas Turbine Tutorial - ChemCad Draft - 01 15 2020Document58 pagesProject 3 - Gas Turbine Tutorial - ChemCad Draft - 01 15 2020Daniel Andres Canro CalderónNo ratings yet