You might also like
- Amboss NotesDocument12 pagesAmboss NotesVee Mend100% (2)
- DR Nilukshi Perera Consultant HaematologistDocument68 pagesDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- UWorld Notes Step 2Document93 pagesUWorld Notes Step 2Vee Mend100% (1)
- Spleen PowerpointDocument30 pagesSpleen PowerpointZakira Alberto100% (1)
- Schwartz Chapter 33 SpleenDocument20 pagesSchwartz Chapter 33 SpleenGay Solas Epalan100% (1)
- Physiology Summary Chapter 20Document9 pagesPhysiology Summary Chapter 20gail01850% (2)
- 2023.neuroscience - Trans10.posterior Fossa Level Brainstem Cranial Nuclei and NervesDocument7 pages2023.neuroscience - Trans10.posterior Fossa Level Brainstem Cranial Nuclei and NervesstellaNo ratings yet
- Platelet BOOK PDFDocument400 pagesPlatelet BOOK PDFVikashgtm100% (1)
- Haematology: Questions&AnswersDocument87 pagesHaematology: Questions&AnswersCielNo ratings yet
- SpleenDocument42 pagesSpleenRashed LabNo ratings yet
- Spleen: - Surgical Anatomy - Functions - Causes of Spleenomegaly - Congenital Abnormalities - Rupture of SpleenDocument33 pagesSpleen: - Surgical Anatomy - Functions - Causes of Spleenomegaly - Congenital Abnormalities - Rupture of SpleenRyhan_Hussain_3590100% (1)
- General Presentations:: SplenomegalyDocument4 pagesGeneral Presentations:: SplenomegalyDaniela DiazNo ratings yet
- Spleno - DR MOKHTARDocument57 pagesSpleno - DR MOKHTARAbdelrahman MokhtarNo ratings yet
- Splenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesDocument58 pagesSplenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Spleen AnatomyDocument74 pagesSpleen AnatomysaadNo ratings yet
- Approach To Patient With Splenomegaly 2Document57 pagesApproach To Patient With Splenomegaly 2Saja SaqerNo ratings yet
- The Spleen: Schwartz's Principles of Surgery 11th EdDocument54 pagesThe Spleen: Schwartz's Principles of Surgery 11th EdaddelinsNo ratings yet
- 2007 Nov 07 CompleteDocument62 pages2007 Nov 07 CompleteKay BristolNo ratings yet
- The Spleen: by DR (MRS) BaulchDocument42 pagesThe Spleen: by DR (MRS) BaulchPrincewill SeiyefaNo ratings yet
- Systemic Sclerosis (Scleroderma)Document3 pagesSystemic Sclerosis (Scleroderma)AtiqahNo ratings yet
- Annalyn S. Da-Anoy, M.D., R.M.T.Document88 pagesAnnalyn S. Da-Anoy, M.D., R.M.T.api-25914483No ratings yet
- Systemic Lupus Erythematosus SLE: DefinitionDocument19 pagesSystemic Lupus Erythematosus SLE: DefinitionShimmering MoonNo ratings yet
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDocument5 pagesTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752No ratings yet
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocument53 pagesSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadNo ratings yet
- The Spleen: Schwartz's Principles of Surgery 11th EdDocument54 pagesThe Spleen: Schwartz's Principles of Surgery 11th EdMuhammad Fhandeka IsrarNo ratings yet
- Surgical Diseases of The SpleenDocument28 pagesSurgical Diseases of The SpleenRassoul Abu-NuwarNo ratings yet
- Thyroid & Parathyroid Glands: Hurthle CellsDocument25 pagesThyroid & Parathyroid Glands: Hurthle CellschristianNo ratings yet
- Charts For Kidney and Lower Urinary Tract Pathology. NephrologyDocument34 pagesCharts For Kidney and Lower Urinary Tract Pathology. NephrologyM PatelNo ratings yet
- SplenomegalyDocument4 pagesSplenomegalydoctorimrankabirNo ratings yet
- Station 5 Cases 4Document73 pagesStation 5 Cases 4Sagit Nauman81100% (1)
- Rare DiseasesDocument15 pagesRare DiseasesTaimur Khalil100% (1)
- Plabable 2020 Hematology MfaDocument87 pagesPlabable 2020 Hematology MfaDr. Saqib RazaNo ratings yet
- K-5 Pathophysiology of Cyanotic Congenital Heart DefectsDocument15 pagesK-5 Pathophysiology of Cyanotic Congenital Heart DefectsJessica GintingNo ratings yet
- Clinical Features Investigations: Aplastic Anaemia Primary Idiopathic Acquiredaplastic AnaemiaDocument5 pagesClinical Features Investigations: Aplastic Anaemia Primary Idiopathic Acquiredaplastic AnaemiaananNo ratings yet
- Acute Myeloid LekumiaDocument34 pagesAcute Myeloid LekumiaBhuwan ThapaNo ratings yet
- SplenectomyDocument17 pagesSplenectomyDONALD UNASHENo ratings yet
- Aplastic Anemia Lecture 1aDocument39 pagesAplastic Anemia Lecture 1aniaaseta100% (2)
- Hema Part 3 Final PDFDocument188 pagesHema Part 3 Final PDFH.B.ANo ratings yet
- Aplastic AnemiaDocument16 pagesAplastic Anemiahazelposis100% (1)
- Diseases of Urinary SystemDocument29 pagesDiseases of Urinary SystemHassan.shehri100% (9)
- Acute GlomerulonephritisDocument32 pagesAcute Glomerulonephritismelese woldehawariatNo ratings yet
- Hematologicalemergencies 2 190101164652Document42 pagesHematologicalemergencies 2 190101164652dita evitaNo ratings yet
- (Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Document15 pages(Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Aria Jean MostajoNo ratings yet
- What Are The Criteria of Differentiation Between A Mass of Splenic Origin and Another of Renal Origin On Physical Examination?Document4 pagesWhat Are The Criteria of Differentiation Between A Mass of Splenic Origin and Another of Renal Origin On Physical Examination?AYAAAAAAAAAA222No ratings yet
- Approach To A Child With Pallor and Hepatosplenomegaly: Anirban Das, MD, DMDocument7 pagesApproach To A Child With Pallor and Hepatosplenomegaly: Anirban Das, MD, DMMarc Lyndon CafinoNo ratings yet
- Pediatric Systemic Lupus Erythematosus: Pediatric Rheumatology Red Team Resident Teaching SeriesDocument52 pagesPediatric Systemic Lupus Erythematosus: Pediatric Rheumatology Red Team Resident Teaching SeriesLili ManaoNo ratings yet
- SpherocytosisDocument4 pagesSpherocytosisMohammed IbrahimNo ratings yet
- TJH 20 3 163 165Document3 pagesTJH 20 3 163 165ece142No ratings yet
- Vascular Tumors: Pgi Pauline BaluisDocument114 pagesVascular Tumors: Pgi Pauline BaluisPahw BaluisNo ratings yet
- Hematology Topics 16-20Document20 pagesHematology Topics 16-20Angelo Jude CobachaNo ratings yet
- Acute Myeloblastic Leukemia AML: Dr. Amged H.AbdelrhmanDocument23 pagesAcute Myeloblastic Leukemia AML: Dr. Amged H.Abdelrhmanد. أمجد حسين عبد الرحمنNo ratings yet
- Aplastic AnemiaDocument23 pagesAplastic Anemiasamar yousif mohamedNo ratings yet
- Sisay Berane 083 PancytopeniaDocument23 pagesSisay Berane 083 PancytopeniaRas Siko SafoNo ratings yet
- Acute LeukemiaDocument25 pagesAcute LeukemiaТаня МарченкоNo ratings yet
- PANCYTOPENIADocument51 pagesPANCYTOPENIAResmyNo ratings yet
- View A Negative Experience in Your Life Like You'd Look at A Photo Negative. A Single Negative Can Create An Unlimited Number of Positive Prints.Document90 pagesView A Negative Experience in Your Life Like You'd Look at A Photo Negative. A Single Negative Can Create An Unlimited Number of Positive Prints.madhuNo ratings yet
- All About Pleural EffusionDocument6 pagesAll About Pleural EffusionTantin KristantoNo ratings yet
- eMRCS Pathology 326 MCQsDocument101 pageseMRCS Pathology 326 MCQsSaad KhanNo ratings yet
- Splenomegaly and HypersplenismDocument59 pagesSplenomegaly and Hypersplenismanas hindawi100% (3)
- Chronic Myeloproliferative DisorderDocument25 pagesChronic Myeloproliferative DisorderJilycamae COSMODNo ratings yet
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
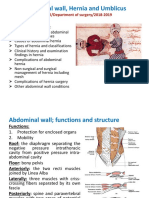
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Document46 pagesAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarNo ratings yet
- Second Trimester MiscarriageDocument5 pagesSecond Trimester MiscarriageAmmarNo ratings yet
- Menstrual Cycle: - Assistance Professor Dr. Wissam Akram - Fifth Year Lecture - 2020-2021Document23 pagesMenstrual Cycle: - Assistance Professor Dr. Wissam Akram - Fifth Year Lecture - 2020-2021AmmarNo ratings yet
- Invasive Disease of VulvaDocument5 pagesInvasive Disease of VulvaAmmarNo ratings yet
- Induced Abortion: Dr. Ali Murad Dr. Wassan NoriDocument12 pagesInduced Abortion: Dr. Ali Murad Dr. Wassan NoriAmmarNo ratings yet
- EndometrisisDocument10 pagesEndometrisisAmmarNo ratings yet
- 7 - HydrocephalusDocument4 pages7 - HydrocephalusAmmarNo ratings yet
- 5 - Space Occupying LesionsDocument39 pages5 - Space Occupying LesionsAmmarNo ratings yet
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- 4 - Raised ICPDocument6 pages4 - Raised ICPAmmarNo ratings yet
- 6 - Intracranial MassDocument5 pages6 - Intracranial MassAmmarNo ratings yet
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- DR Mohamed Al Tamiami:5 Class Lecture 1 OnDocument6 pagesDR Mohamed Al Tamiami:5 Class Lecture 1 OnAmmarNo ratings yet
- Peripheral NeuropathyDocument7 pagesPeripheral NeuropathyAmmarNo ratings yet
- Head Injury 2: (DR Mohamed A. J. Al Tamimi)Document10 pagesHead Injury 2: (DR Mohamed A. J. Al Tamimi)AmmarNo ratings yet
- Juvenile Idiopathic ArthritisDocument4 pagesJuvenile Idiopathic ArthritisAmmarNo ratings yet
- "Neonatal Infections" Lecture 1: Pediatrics Dr. Sawsan AliDocument5 pages"Neonatal Infections" Lecture 1: Pediatrics Dr. Sawsan AliAmmarNo ratings yet
- The Challenge of Kidney Damage During Interventional Cardiology ProceduresDocument6 pagesThe Challenge of Kidney Damage During Interventional Cardiology ProceduresIJAR JOURNALNo ratings yet
- LTE TG Module 1 Respiratory PDFDocument26 pagesLTE TG Module 1 Respiratory PDFAnnEviteNo ratings yet
- Abnormal Uterine BleedingDocument5 pagesAbnormal Uterine Bleedingmendato marcabanNo ratings yet
- CKD PDFDocument26 pagesCKD PDFNogra CarlNo ratings yet
- Approach To The Adult With Pancytopenia - UpToDateDocument32 pagesApproach To The Adult With Pancytopenia - UpToDatePatricio RamirezNo ratings yet
- All Lecture Notes EuropeanDocument906 pagesAll Lecture Notes Europeanabdul100% (1)
- 2018 Book PrimaryAngioplastyDocument339 pages2018 Book PrimaryAngioplastyRami El-Mokdad100% (2)
- NCM 118 - Trans 1Document4 pagesNCM 118 - Trans 1NAYLA MAUBANNo ratings yet
- Final Assignment of ShockDocument21 pagesFinal Assignment of Shocknyandap tanyuNo ratings yet
- Maui's Tips For Natural Remedies V2.3Document57 pagesMaui's Tips For Natural Remedies V2.3DennisNo ratings yet
- Greys-Anatomy-Student (1) - CompressedDocument2 pagesGreys-Anatomy-Student (1) - CompressedKaranNo ratings yet
- JurnalDocument12 pagesJurnalFKWNo ratings yet
- Amniotic Fluid Embolism: About A CaseDocument4 pagesAmniotic Fluid Embolism: About A CaseIJAR JOURNALNo ratings yet
- Vishram Singh - Selective Anatomy - Prep Manual For Undergraduates (Vol - 2) - 2E. 2-Elsevier (INR) (2020)Document468 pagesVishram Singh - Selective Anatomy - Prep Manual For Undergraduates (Vol - 2) - 2E. 2-Elsevier (INR) (2020)Pappu KumarNo ratings yet
- Null 1Document8 pagesNull 1arpit kaushikNo ratings yet
- Evidence-Based Review and Consensus Statement On Monitoring of Hemodynamics and Oxygen Transport BalanceDocument61 pagesEvidence-Based Review and Consensus Statement On Monitoring of Hemodynamics and Oxygen Transport Balancesusanita1974No ratings yet
- Mobilizing Pre-Heart-Transplant Patients With A Percutaneously Placed Axillary-Subclavian Intraaortic Balloon Pump: A Retrospective StudyDocument6 pagesMobilizing Pre-Heart-Transplant Patients With A Percutaneously Placed Axillary-Subclavian Intraaortic Balloon Pump: A Retrospective StudyDheaDesniaNo ratings yet
- Anaphylactic Shock FINAL PATHODocument3 pagesAnaphylactic Shock FINAL PATHOCG Patron BamboNo ratings yet
- The Circulatory System ReviewerDocument4 pagesThe Circulatory System ReviewerKaten KyoukotsuNo ratings yet
- Cushing SyndromeDocument10 pagesCushing SyndromeAkim DanielNo ratings yet
- NCM101J - Nursing Health Assessment - Week 3Document31 pagesNCM101J - Nursing Health Assessment - Week 3Jenny Ruth TubanNo ratings yet
- Thromboangiitis Obliterans (Buerger Disease)Document12 pagesThromboangiitis Obliterans (Buerger Disease)Sheila AzelyaNo ratings yet
- Case 5 - (Salimbagat) Diagnostic and Laboratory ProceduresDocument12 pagesCase 5 - (Salimbagat) Diagnostic and Laboratory ProceduresChristine Pialan SalimbagatNo ratings yet
- Shock: Classification, Pathophysiology, and Approach To ManagementDocument45 pagesShock: Classification, Pathophysiology, and Approach To ManagementClaudia IsabelNo ratings yet
- Amniodarone (Norvasc) Drug SummDocument1 pageAmniodarone (Norvasc) Drug SummWarrenNo ratings yet
- Arrhythmia Essentials 2Nd Edition Edition Brian Olshansky Full ChapterDocument51 pagesArrhythmia Essentials 2Nd Edition Edition Brian Olshansky Full Chapterallan.morgan579100% (6)
- How I Personalize Fluid Therapy in Septic Shock?: Review Open AccessDocument11 pagesHow I Personalize Fluid Therapy in Septic Shock?: Review Open AccessGian CarloNo ratings yet