You might also like
- Head Trauma: Yoon Seung-Hwan, M.DDocument53 pagesHead Trauma: Yoon Seung-Hwan, M.DAhmed ZahranNo ratings yet
- Head InjuryDocument42 pagesHead InjuryMohammad Husni Banisalman100% (3)
- Med Surg Study GuideDocument98 pagesMed Surg Study Guideprogramgrabber100% (2)
- Flap Design For Minor Oral SurgeryDocument22 pagesFlap Design For Minor Oral SurgeryWendy Jeng88% (8)
- Acute Pain Hysterectomy MyomaDocument1 pageAcute Pain Hysterectomy Myomarozj0780% (5)
- CMS 3000 High Frequency Surgical Unit: FeatureDocument1 pageCMS 3000 High Frequency Surgical Unit: Feature-Nurman Hidayat-No ratings yet
- Management of Head InjuriesDocument90 pagesManagement of Head InjuriesrobelNo ratings yet
- Traumatic Brain InjuryDocument14 pagesTraumatic Brain InjuryBelle CaharopNo ratings yet
- Traumatic Brain Injuries: Assoc. Prof. Dr. Vicentiu M. SăceleanuDocument38 pagesTraumatic Brain Injuries: Assoc. Prof. Dr. Vicentiu M. SăceleanuAnna DianaNo ratings yet
- Head Injury Causes and TreatmentDocument47 pagesHead Injury Causes and TreatmentnikowareNo ratings yet
- Traumatic Brain InJuryDocument21 pagesTraumatic Brain InJuryShara SampangNo ratings yet
- Head Trauma: Yoon Seung-Hwan, M.DDocument53 pagesHead Trauma: Yoon Seung-Hwan, M.Dilham darnoNo ratings yet
- Head InjuryDocument6 pagesHead InjuryHurrinazilla AwaliaNo ratings yet
- Computed TomographyDocument5 pagesComputed TomographyCrisMartAgullanaNo ratings yet
- Head InjuryDocument11 pagesHead InjurypertinenteNo ratings yet
- Traumatic Brain Injury: Department of Neurosurgery, The First Affiliated Hospital of Zhengzhou University Xu BinDocument95 pagesTraumatic Brain Injury: Department of Neurosurgery, The First Affiliated Hospital of Zhengzhou University Xu Binapi-19916399No ratings yet
- D. Intralipid 20%: A. Temazepam B. Lorazepam C. NaloxoneDocument122 pagesD. Intralipid 20%: A. Temazepam B. Lorazepam C. NaloxoneOstazNo ratings yet
- All Previous Essay SurgeryDocument170 pagesAll Previous Essay Surgeryalsfyabdullah2021No ratings yet
- Acute Epidural Hemorrhage Causes and TreatmentDocument4 pagesAcute Epidural Hemorrhage Causes and TreatmentYesenia YesiNo ratings yet
- Trauma ManagementDocument39 pagesTrauma ManagementAbdesselam BerrehailNo ratings yet
- Head InjuryDocument34 pagesHead Injuryrxmskdkd33No ratings yet
- All Previous Essay Surgery 2Document162 pagesAll Previous Essay Surgery 2DR/ AL-saifiNo ratings yet
- Emd166 Slide Head InjuryDocument40 pagesEmd166 Slide Head Injuryarikashafa6No ratings yet
- Head Trauma (Head Injury) : Thitinan LimchoopornwikulDocument42 pagesHead Trauma (Head Injury) : Thitinan LimchoopornwikulPasut ChangeNo ratings yet
- Chapter 23the Multiply & Severely Injured PatientDocument19 pagesChapter 23the Multiply & Severely Injured PatientWahyuNo ratings yet
- Subdural HematomaDocument8 pagesSubdural HematomaaaronmanullangNo ratings yet
- Chronic Subdural HematomaDocument21 pagesChronic Subdural Hematomamarc_caronan100% (2)
- Med Surg Study GuideDocument98 pagesMed Surg Study Guideprogramgrabber100% (23)
- A Subdural HematomaDocument12 pagesA Subdural HematomaGina Irene IshakNo ratings yet
- AADocument4 pagesAARiski novita sari DjamalNo ratings yet
- CEDERA KEPALA ASPEK PENTING DI DIAGNOSA DAN PENANGANANDocument26 pagesCEDERA KEPALA ASPEK PENTING DI DIAGNOSA DAN PENANGANANJainir RegarNo ratings yet
- CraniectomyDocument5 pagesCraniectomytabanaoNo ratings yet
- Head and Spinal Cord Injury (Ci)Document111 pagesHead and Spinal Cord Injury (Ci)azmerawNo ratings yet
- Med SurgDocument98 pagesMed SurgKimsha Concepcion88% (8)
- SLSU College of Allied Medicine Case Study on Bilateral Subdural HematomaDocument27 pagesSLSU College of Allied Medicine Case Study on Bilateral Subdural HematomaRoeder Max Pangramuyen100% (4)
- Surgical Management of Head InjuryDocument12 pagesSurgical Management of Head InjurySumiethaa ShanmuganathanNo ratings yet
- Subdural Hematome: Oleh: Maha Satya Pembimbing: DR - Dr.Nyoman Golden, Spbs (K)Document55 pagesSubdural Hematome: Oleh: Maha Satya Pembimbing: DR - Dr.Nyoman Golden, Spbs (K)Maha Satya Dwi PalgunaNo ratings yet
- Epidural Hematoma: Continuing Education ActivityDocument16 pagesEpidural Hematoma: Continuing Education ActivityIka AriandanaNo ratings yet
- NeuroimagingDocument79 pagesNeuroimagingIdris LubisNo ratings yet
- Traumatic Brain Injury: 2. Prophylactic HypothermiaDocument77 pagesTraumatic Brain Injury: 2. Prophylactic HypothermiaNinaNo ratings yet
- SurgeryDocument65 pagesSurgerysamreenNo ratings yet
- Classifying Head InjuriesDocument6 pagesClassifying Head InjuriesMohamed Al-zichrawyNo ratings yet
- Neurosurgery: Subarachnoid HemorrhageDocument5 pagesNeurosurgery: Subarachnoid HemorrhagepvsvrNo ratings yet
- Epidural Hematoma: EpidemiologyDocument5 pagesEpidural Hematoma: EpidemiologySafrilia GandhiNo ratings yet
- Head Injury - the silent epidemicDocument52 pagesHead Injury - the silent epidemickarahmanNo ratings yet
- Dr. Ali Adnan Discusses Types of Intracranial HemorrhageDocument6 pagesDr. Ali Adnan Discusses Types of Intracranial HemorrhageMohammed SattarNo ratings yet
- Head InjuryDocument50 pagesHead InjuryThiagarajah RaviNo ratings yet
- Head Injury Outline of Management CDocument89 pagesHead Injury Outline of Management CPanna SahaNo ratings yet
- CraniotomyDocument9 pagesCraniotomyandrea_zolayvarNo ratings yet
- Head CTDocument84 pagesHead CTAnirbanMallikNo ratings yet
- Management of Head Injuries (Open and ClosedDocument48 pagesManagement of Head Injuries (Open and ClosedAsmahan AliNo ratings yet
- EDH - Epidural HematomaDocument5 pagesEDH - Epidural HematomaJulintari BidramnantaNo ratings yet
- 2 5291964174748882717Document11 pages2 5291964174748882717نشط عقلكNo ratings yet
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- 5.nervous System PDFDocument88 pages5.nervous System PDFMelancholy MedicineNo ratings yet
- Head InjuryDocument30 pagesHead InjuryAngel MakinNo ratings yet
- Epidural Hematom: Dewi Sartika NIM 22041919310002Document32 pagesEpidural Hematom: Dewi Sartika NIM 22041919310002Dewi Sartika100% (1)
- Description: Increased Intracranial Pressure, P. 346Document5 pagesDescription: Increased Intracranial Pressure, P. 346bittttttttttNo ratings yet
- Kjellberg 1971Document6 pagesKjellberg 1971Samantha AdrianneNo ratings yet
- Traumatic Brain Injury (TBI)Document48 pagesTraumatic Brain Injury (TBI)Alaa OmarNo ratings yet
- Subdural Hematoma Case PresentationDocument20 pagesSubdural Hematoma Case PresentationDarwin Arockia RajNo ratings yet
- Subdural HematomaDocument7 pagesSubdural Hematomamiss RN50% (2)
- 22 - Postoperative Complications and Managament IIDocument39 pages22 - Postoperative Complications and Managament IIAmmarNo ratings yet
- Spleen Lec.2Document17 pagesSpleen Lec.2AmmarNo ratings yet
- Second Trimester MiscarriageDocument5 pagesSecond Trimester MiscarriageAmmarNo ratings yet
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
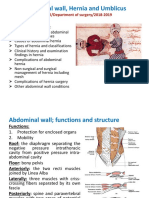
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Document46 pagesAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarNo ratings yet
- Spleen Lec.1Document30 pagesSpleen Lec.1AmmarNo ratings yet
- Bariatric and Metabolic SurgeryDocument32 pagesBariatric and Metabolic SurgeryAmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Induced Abortion: Dr. Ali Murad Dr. Wassan NoriDocument12 pagesInduced Abortion: Dr. Ali Murad Dr. Wassan NoriAmmarNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- Polycystic Ovary Syndrome: Learning ObjectivesDocument8 pagesPolycystic Ovary Syndrome: Learning ObjectivesAmmarNo ratings yet
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarNo ratings yet
- Menstrual cycle clinical considerationsDocument23 pagesMenstrual cycle clinical considerationsAmmarNo ratings yet
- Recurrent MiscarriageDocument9 pagesRecurrent MiscarriageAmmarNo ratings yet
- INVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTDocument5 pagesINVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTAmmarNo ratings yet
- INVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTDocument5 pagesINVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTAmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- IntersexDocument10 pagesIntersexAmmarNo ratings yet
- EndometrisisDocument10 pagesEndometrisisAmmarNo ratings yet
- 10 - Spinal Cord Injuries Lec.1Document7 pages10 - Spinal Cord Injuries Lec.1AmmarNo ratings yet
- 9 - Spinal Cord InjuriesDocument61 pages9 - Spinal Cord InjuriesAmmarNo ratings yet
- Intracranial Mass DiagnosisDocument5 pagesIntracranial Mass DiagnosisAmmarNo ratings yet
- 7 - HydrocephalusDocument4 pages7 - HydrocephalusAmmarNo ratings yet
- 5 - Space Occupying LesionsDocument39 pages5 - Space Occupying LesionsAmmarNo ratings yet
- 11 - Spinal Cord Injuries Lec.2Document4 pages11 - Spinal Cord Injuries Lec.2AmmarNo ratings yet
- 4 - Raised ICPDocument6 pages4 - Raised ICPAmmarNo ratings yet
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- FIQ - Proliferative Diabetic RetinopathyDocument35 pagesFIQ - Proliferative Diabetic RetinopathyHikban FiqhiNo ratings yet
- Paraphimosis (Ingles)Document1 pageParaphimosis (Ingles)Joaquín SosaNo ratings yet
- Dentoalveolar & ImplantsDocument10 pagesDentoalveolar & ImplantsabdullahNo ratings yet
- MetaanalysisDocument12 pagesMetaanalysisAhmed BadrNo ratings yet
- Urology in India Numbers and PracticeDocument3 pagesUrology in India Numbers and PracticebrightozhrNo ratings yet
- Pathophysiology DiagramDocument1 pagePathophysiology Diagramzebzeb STEMANo ratings yet
- Management in Radiology (Mir) CongressDocument52 pagesManagement in Radiology (Mir) CongressElvira RodNo ratings yet
- FINAL - Media Statement - MCH Update SMRMCDocument1 pageFINAL - Media Statement - MCH Update SMRMCEdlyn Jade TagulaoNo ratings yet
- Arteriovenous Access for HemodialysisDocument11 pagesArteriovenous Access for Hemodialysislakshminivas PingaliNo ratings yet
- Corpus Alienum EsophagusDocument3 pagesCorpus Alienum EsophagusTrhey Ahmilza DamaitaNo ratings yet
- Achieve Programmable Automatic Biopsy System: Spring-Loaded Action For Fast, Accurate PenetrationDocument4 pagesAchieve Programmable Automatic Biopsy System: Spring-Loaded Action For Fast, Accurate PenetrationradeonunNo ratings yet
- DEV2011 2018 Practical Week 8 DRAFT REPORT PDFDocument1 pageDEV2011 2018 Practical Week 8 DRAFT REPORT PDFAreesha FatimaNo ratings yet
- RCSED Regulations for Oral and Maxillofacial Surgery DiplomaDocument7 pagesRCSED Regulations for Oral and Maxillofacial Surgery DiplomaGaurav ChakrabartyNo ratings yet
- SH Catalogue - UrologyDocument5 pagesSH Catalogue - UrologySahil sharmaNo ratings yet
- Medind - Nic.in Iad t08 s1 Iadt08s1p688Document11 pagesMedind - Nic.in Iad t08 s1 Iadt08s1p688Anonymous S0H8cqgnfiNo ratings yet
- Contemporary Perioperative Haemodynamic MonitoringDocument12 pagesContemporary Perioperative Haemodynamic MonitoringrjerezrNo ratings yet
- Weinberg1958 Tooth Position in Relation To The Denture Base FoundationDocument8 pagesWeinberg1958 Tooth Position in Relation To The Denture Base FoundationSanasalud Pedro De ValdiviaNo ratings yet
- 1 s2.0 S002234682200834X MainDocument7 pages1 s2.0 S002234682200834X MainenimaNo ratings yet
- Group Health Insurance - Policy Overview.Document14 pagesGroup Health Insurance - Policy Overview.Sai SandeepNo ratings yet
- Breast Reconstruction Selected Readings in Plastic SurgeryDocument87 pagesBreast Reconstruction Selected Readings in Plastic SurgeryJordan LauNo ratings yet
- Trauma Penetrante y Contuso de Cuello (ORL)Document13 pagesTrauma Penetrante y Contuso de Cuello (ORL)Rodrix004No ratings yet
- Vandooren Interdisc 2 LeseprobeDocument33 pagesVandooren Interdisc 2 LeseprobeAlfred OrozcoNo ratings yet
- Jaccoa 11 00412Document5 pagesJaccoa 11 00412Sardi MonNo ratings yet
- Diastole and AnesthesiaDocument16 pagesDiastole and AnesthesiadrsubramanianNo ratings yet
- Outpatient SurgeryDocument7 pagesOutpatient SurgeryJulián David Ríos ZuluagaNo ratings yet
- Treatment of VME Using Extra Alveolar TADs Quantifica - 2018 - Seminars in OrthDocument12 pagesTreatment of VME Using Extra Alveolar TADs Quantifica - 2018 - Seminars in OrthLabassy RymeNo ratings yet
- Affections of The Salivary Ducts in Buffaloes: ISSN: 2226-4485 (Print) ISSN: 2218-6050 (Online)Document4 pagesAffections of The Salivary Ducts in Buffaloes: ISSN: 2226-4485 (Print) ISSN: 2218-6050 (Online)TriandNo ratings yet