You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Spleen Lec.1Document30 pagesSpleen Lec.1AmmarNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
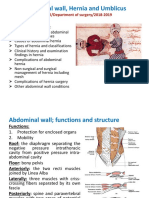
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Document46 pagesAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Second Trimester MiscarriageDocument5 pagesSecond Trimester MiscarriageAmmarNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Menstrual Cycle: - Assistance Professor Dr. Wissam Akram - Fifth Year Lecture - 2020-2021Document23 pagesMenstrual Cycle: - Assistance Professor Dr. Wissam Akram - Fifth Year Lecture - 2020-2021AmmarNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Induced Abortion: Dr. Ali Murad Dr. Wassan NoriDocument12 pagesInduced Abortion: Dr. Ali Murad Dr. Wassan NoriAmmarNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Invasive Disease of VulvaDocument5 pagesInvasive Disease of VulvaAmmarNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 7 - HydrocephalusDocument4 pages7 - HydrocephalusAmmarNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 6 - Intracranial MassDocument5 pages6 - Intracranial MassAmmarNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 5 - Space Occupying LesionsDocument39 pages5 - Space Occupying LesionsAmmarNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- EndometrisisDocument10 pagesEndometrisisAmmarNo ratings yet
- 4 - Raised ICPDocument6 pages4 - Raised ICPAmmarNo ratings yet
- DR Mohamed Al Tamiami:5 Class Lecture 1 OnDocument6 pagesDR Mohamed Al Tamiami:5 Class Lecture 1 OnAmmarNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Head Injury 2: (DR Mohamed A. J. Al Tamimi)Document10 pagesHead Injury 2: (DR Mohamed A. J. Al Tamimi)AmmarNo ratings yet
- Juvenile Idiopathic ArthritisDocument4 pagesJuvenile Idiopathic ArthritisAmmarNo ratings yet
- Peripheral NeuropathyDocument7 pagesPeripheral NeuropathyAmmarNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- "Neonatal Infections" Lecture 1: Pediatrics Dr. Sawsan AliDocument5 pages"Neonatal Infections" Lecture 1: Pediatrics Dr. Sawsan AliAmmarNo ratings yet
- Wound HealingDocument70 pagesWound HealingSachin KpNo ratings yet
- Surgery Ospe 322Document322 pagesSurgery Ospe 322fbf50269No ratings yet
- AFA ReviwerDocument21 pagesAFA ReviwerLovely day ybanezNo ratings yet
- BCAAs and Body Composition - Art de Vany On LineDocument2 pagesBCAAs and Body Composition - Art de Vany On LineDellNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- HistamineDocument21 pagesHistamineMartina Alarcon Acevedo100% (1)
- Intensive Care Management of The Head Injured Patient: Review ArticleDocument14 pagesIntensive Care Management of The Head Injured Patient: Review ArticlerickyGKNo ratings yet
- Treatment of Sacroiliac Joint DysfunctionDocument46 pagesTreatment of Sacroiliac Joint DysfunctionMichel Bakker100% (5)
- HIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10Document116 pagesHIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10joe joeNo ratings yet
- Report Text LatihanDocument12 pagesReport Text Latihanbenta pasyahNo ratings yet
- Health 9 Module 1&2 G9 2020Document31 pagesHealth 9 Module 1&2 G9 2020Acos JibsonNo ratings yet
- Revalida 1Document3 pagesRevalida 1herrabiel solisNo ratings yet
- A Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)Document7 pagesA Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)NyomanGinaHennyKristiantiNo ratings yet
- Persuasive LetterDocument2 pagesPersuasive Letterapi-341527188No ratings yet
- Plasmodium Infection (Malaria) : Medical ParasitologyDocument7 pagesPlasmodium Infection (Malaria) : Medical ParasitologyBalisi Manuel FranciscoNo ratings yet
- PrepositionsDocument10 pagesPrepositionsZahoor Ul HaqNo ratings yet
- TURP SyndromeDocument13 pagesTURP SyndromeWindy Ari WijayaNo ratings yet
- The Role of Chronic PainDocument23 pagesThe Role of Chronic PainNovia RambakNo ratings yet
- Chapter 6 The Circulatory System of MammalsDocument30 pagesChapter 6 The Circulatory System of MammalsRethenaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Etiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDateDocument22 pagesEtiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDatecuentaparatrabajosdelau10No ratings yet
- A Study On Knowledge and Practice of Mothers of Under-Five ChildrenDocument6 pagesA Study On Knowledge and Practice of Mothers of Under-Five ChildrenRirin PurbaNo ratings yet
- Review - Spinal Cord Injury - 2Document1 pageReview - Spinal Cord Injury - 2Sarah MendozaNo ratings yet
- Script For OrientationDocument2 pagesScript For OrientationAngela CudiaNo ratings yet
- Trauma ToraksDocument30 pagesTrauma ToraksMichael KwanNo ratings yet
- Helicobacter Pylori. One Bacterium and A Broad Spectrum of Human Disease! An OverviewDocument14 pagesHelicobacter Pylori. One Bacterium and A Broad Spectrum of Human Disease! An OverviewAlexandru CozmaNo ratings yet
- CellCommunication Assessment3Document6 pagesCellCommunication Assessment3Michaela Maria GarciaNo ratings yet
- CHAPTER 4: Modifiable Risk Factors of Lifestyle Diseases: SmokingDocument4 pagesCHAPTER 4: Modifiable Risk Factors of Lifestyle Diseases: SmokingShimah100% (2)
- Chromosome Walking: and David S. Hogness in The Early 1980'sDocument4 pagesChromosome Walking: and David S. Hogness in The Early 1980'sprakash singhNo ratings yet
- Examinatin in Intensive CareDocument731 pagesExaminatin in Intensive Careyankee1111100% (1)
- The Benefits of Cider VinegarDocument15 pagesThe Benefits of Cider VinegarAldoSolsaNo ratings yet
- 02 - Recalibrating Gavi 5.0 in Light of COVID-19 and Successful Replenis..Document19 pages02 - Recalibrating Gavi 5.0 in Light of COVID-19 and Successful Replenis..aman_sasanNo ratings yet