You might also like
- Vulval CancerDocument9 pagesVulval CancerSana LodhiNo ratings yet
- Vulvar Cancer: An Overview of Epidemiology, Risk Factors, Presentation, Pathophysiology, Staging, and TreatmentDocument8 pagesVulvar Cancer: An Overview of Epidemiology, Risk Factors, Presentation, Pathophysiology, Staging, and TreatmentLisa Raihan LutfiaNo ratings yet
- ONCOLOGICAL GYNECOLOGY-Malignant Diseases of The Vulva and Modalities of Treatment by Prof - Dr.Vesna AntovskaDocument22 pagesONCOLOGICAL GYNECOLOGY-Malignant Diseases of The Vulva and Modalities of Treatment by Prof - Dr.Vesna AntovskaVesna AntovskaNo ratings yet
- Management of CA Vulva 2Document33 pagesManagement of CA Vulva 2api-3705046No ratings yet
- Cancer of The Vulva FIGO 2018Document42 pagesCancer of The Vulva FIGO 2018Abi BazarNo ratings yet
- Bladder Cancer 1Document31 pagesBladder Cancer 1Anas HamadNo ratings yet
- Vulval CaDocument54 pagesVulval CaChethana BhatNo ratings yet
- en Dome Trial CarcinomaDocument31 pagesen Dome Trial Carcinomadr_asalehNo ratings yet
- ONCOLOGICAL GYNECOLOGY - Malignant Tumors of The Vagina and Modalities of TreatmentDocument9 pagesONCOLOGICAL GYNECOLOGY - Malignant Tumors of The Vagina and Modalities of TreatmentVesna AntovskaNo ratings yet
- Breast Cancer Study Case PDFDocument8 pagesBreast Cancer Study Case PDFLuna LinNo ratings yet
- Vaginal CarcinomaDocument8 pagesVaginal CarcinomaMutiarawati MithrataelúwånzhùNo ratings yet
- Diagnosis and Treatment of Vulvar Precancerous Lesions and CancerDocument4 pagesDiagnosis and Treatment of Vulvar Precancerous Lesions and CancerSyahril FauziNo ratings yet
- Testicular TumorsDocument6 pagesTesticular Tumorsyoussef.aziz2020No ratings yet
- Epidemiology: Ultrasound Pelvic MRIDocument18 pagesEpidemiology: Ultrasound Pelvic MRIKercia BeatrizNo ratings yet
- د.معد Tumers of Vagina-2 (Muhadharaty)Document25 pagesد.معد Tumers of Vagina-2 (Muhadharaty)Ali EmadNo ratings yet
- Vulvular CancerDocument5 pagesVulvular CancerSyahril FauziNo ratings yet
- Rectal Ca:: Malueth Abraham, MBCHB ViDocument32 pagesRectal Ca:: Malueth Abraham, MBCHB ViMalueth AnguiNo ratings yet
- Oesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHDocument50 pagesOesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHMalgh Kh100% (2)
- Cervical Cancer BMJDocument4 pagesCervical Cancer BMJMaria Camila Ortiz UsugaNo ratings yet
- Cancer Cervix: BY Ahmed Magdy ElmohandesDocument34 pagesCancer Cervix: BY Ahmed Magdy ElmohandesAhmed ElmohandesNo ratings yet
- CPG Gyne VulvarDocument9 pagesCPG Gyne Vulvarpuji arisNo ratings yet
- Vaginal Cuff Removal in Endometrial Carcinoma: Dr. Hira SalmanDocument38 pagesVaginal Cuff Removal in Endometrial Carcinoma: Dr. Hira SalmandrhirasalmanNo ratings yet
- Mantero La 2016Document7 pagesMantero La 2016Dolly JazmiNo ratings yet
- Carcinoma Penis Management GuideDocument63 pagesCarcinoma Penis Management GuideBibek GhimireNo ratings yet
- 120520200benign Malignant Lesions of Vulva VaginaDocument22 pages120520200benign Malignant Lesions of Vulva Vaginaraph faithNo ratings yet
- Wilms Tumour: Nitha K 2 Year MSC NursingDocument40 pagesWilms Tumour: Nitha K 2 Year MSC NursingNITHA K100% (1)
- Malignant Ovarian TumourDocument46 pagesMalignant Ovarian Tumourahmed shorshNo ratings yet
- Cervical Cancer Screening and Risk FactorsDocument54 pagesCervical Cancer Screening and Risk FactorsBi PinNo ratings yet
- Riker ABSITE ReviewDocument36 pagesRiker ABSITE Reviewsgod34No ratings yet
- Chapter 2 - VaginaDocument1 pageChapter 2 - VaginaalexandrumascanNo ratings yet
- Treatment of Lung NeoplasmsDocument18 pagesTreatment of Lung NeoplasmsVenzNo ratings yet
- Journal ReadingDocument41 pagesJournal ReadingEndorfin AdrenalinNo ratings yet
- AnalcancerpptDocument46 pagesAnalcancerpptAnant KumarNo ratings yet
- Untitled 1Document17 pagesUntitled 1Tiberiu CttNo ratings yet
- Current Trends in Extended Lymph Node Dissection For Esophageal CarcinomaDocument6 pagesCurrent Trends in Extended Lymph Node Dissection For Esophageal CarcinomaYacine Tarik AizelNo ratings yet
- Cervical Cancer Risk Factors and ScreeningDocument53 pagesCervical Cancer Risk Factors and Screeningthamizh555No ratings yet
- Vulvar and Vaginal TumorDocument43 pagesVulvar and Vaginal TumorAdam EldiNo ratings yet
- Pathologic Types: o o o oDocument2 pagesPathologic Types: o o o orexzordNo ratings yet
- Colorectal Cancer : Presented By: Anas Jolani - Amiral Aiman - Ahmed FathiDocument55 pagesColorectal Cancer : Presented By: Anas Jolani - Amiral Aiman - Ahmed FathiRashed ShatnawiNo ratings yet
- 2011 Sun Myint Anal CAncer Follow-UpDocument5 pages2011 Sun Myint Anal CAncer Follow-UpgammasharkNo ratings yet
- Salivary Gland TumorDocument62 pagesSalivary Gland Tumordeepak kumarNo ratings yet
- Endometrial Cancer Treatment OptionsDocument18 pagesEndometrial Cancer Treatment OptionsKirsten NVNo ratings yet
- Treatment of Breast Cancer: DR - Syed Alam ZebDocument51 pagesTreatment of Breast Cancer: DR - Syed Alam ZebSucipto HartonoNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- Cervical CancerDocument36 pagesCervical CancerDebabrata SatapathyNo ratings yet
- NAL Eoplasms: Jonathan S. ViernesDocument24 pagesNAL Eoplasms: Jonathan S. ViernesironNo ratings yet
- Cervical Cancer: Predominately Squamous Cell CancerDocument1 pageCervical Cancer: Predominately Squamous Cell CancerAila CamachoNo ratings yet
- What Do You Need To Know About Breast Cancer: DR / Mokhtar Gusmallah Clinical OncologistDocument26 pagesWhat Do You Need To Know About Breast Cancer: DR / Mokhtar Gusmallah Clinical OncologistjehemirNo ratings yet
- Radioguided Sentinel Lymph Node Biopsy in Breast Cancer SurgeryDocument18 pagesRadioguided Sentinel Lymph Node Biopsy in Breast Cancer Surgerybickxy_katiNo ratings yet
- ABC - Oral CancerDocument4 pagesABC - Oral Cancerdewishinta12No ratings yet
- Wikipedia - Vulvar Cancer (For CHECK)Document7 pagesWikipedia - Vulvar Cancer (For CHECK)vitruvianxyzNo ratings yet
- Pathology: Human PapillomavirusDocument15 pagesPathology: Human Papillomavirussandeepv08No ratings yet
- Breast TreatmentDocument6 pagesBreast TreatmentzainabNo ratings yet
- Anus and Rectum: Sam Grasso2019 Cara Reitz 2018 Joshua Dilday2017 Jake Swann 2016Document49 pagesAnus and Rectum: Sam Grasso2019 Cara Reitz 2018 Joshua Dilday2017 Jake Swann 2016Naresh DuthaluriNo ratings yet
- Carcinoma Breast GuideDocument8 pagesCarcinoma Breast GuideYeshvi s100% (1)
- Vulvar Carcinoma: Dilemma, Debates, and Decisions: By: Dr. Puspita SariDocument13 pagesVulvar Carcinoma: Dilemma, Debates, and Decisions: By: Dr. Puspita SariPuspita SariNo ratings yet
- Branchial Cleft Anomalies: Diagnosis and TreatmentDocument20 pagesBranchial Cleft Anomalies: Diagnosis and TreatmentMelita GanNo ratings yet
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceFrom EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceNo ratings yet
- Colorectal Surgery: Clinical Care and ManagementFrom EverandColorectal Surgery: Clinical Care and ManagementBruce GeorgeNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- 22 - Postoperative Complications and Managament IIDocument39 pages22 - Postoperative Complications and Managament IIAmmarNo ratings yet
- Spleen Lec.2Document17 pagesSpleen Lec.2AmmarNo ratings yet
- Second Trimester MiscarriageDocument5 pagesSecond Trimester MiscarriageAmmarNo ratings yet
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
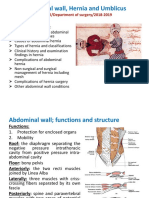
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Document46 pagesAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarNo ratings yet
- Spleen Lec.1Document30 pagesSpleen Lec.1AmmarNo ratings yet
- Bariatric and Metabolic SurgeryDocument32 pagesBariatric and Metabolic SurgeryAmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Induced Abortion: Dr. Ali Murad Dr. Wassan NoriDocument12 pagesInduced Abortion: Dr. Ali Murad Dr. Wassan NoriAmmarNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- Polycystic Ovary Syndrome: Learning ObjectivesDocument8 pagesPolycystic Ovary Syndrome: Learning ObjectivesAmmarNo ratings yet
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarNo ratings yet
- Menstrual cycle clinical considerationsDocument23 pagesMenstrual cycle clinical considerationsAmmarNo ratings yet
- Recurrent MiscarriageDocument9 pagesRecurrent MiscarriageAmmarNo ratings yet
- Malignant Disease of The Body of The UterusDocument12 pagesMalignant Disease of The Body of The UterusAmmarNo ratings yet
- INVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTDocument5 pagesINVASIVE DISEASE OF THE VULVA: RECOGNITION, STAGING, AND TREATMENTAmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- EndometrisisDocument10 pagesEndometrisisAmmarNo ratings yet
- 11 - Spinal Cord Injuries Lec.2Document4 pages11 - Spinal Cord Injuries Lec.2AmmarNo ratings yet
- IntersexDocument10 pagesIntersexAmmarNo ratings yet
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- 9 - Spinal Cord InjuriesDocument61 pages9 - Spinal Cord InjuriesAmmarNo ratings yet
- 7 - HydrocephalusDocument4 pages7 - HydrocephalusAmmarNo ratings yet
- 5 - Space Occupying LesionsDocument39 pages5 - Space Occupying LesionsAmmarNo ratings yet
- Intracranial Mass DiagnosisDocument5 pagesIntracranial Mass DiagnosisAmmarNo ratings yet
- 4 - Raised ICPDocument6 pages4 - Raised ICPAmmarNo ratings yet
- 10 - Spinal Cord Injuries Lec.1Document7 pages10 - Spinal Cord Injuries Lec.1AmmarNo ratings yet
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- Head Injury 2: (DR Mohamed A. J. Al Tamimi)Document10 pagesHead Injury 2: (DR Mohamed A. J. Al Tamimi)AmmarNo ratings yet
- Summary of Nursing TheoriesDocument1 pageSummary of Nursing TheoriesNica Nario Asuncion100% (1)
- Muskuloskeletal Disorder Menggunakan: Analisa Dan Penilaian Risiko Metode Manual Tasks Risk Assessment (Mantra)Document8 pagesMuskuloskeletal Disorder Menggunakan: Analisa Dan Penilaian Risiko Metode Manual Tasks Risk Assessment (Mantra)Dirgntra AlanNo ratings yet
- Journal No. 3 "Specialized Leaves"Document10 pagesJournal No. 3 "Specialized Leaves"Ej AgsaldaNo ratings yet
- The Abreviated Ajahn Brahm - Concise Instructions For Skillful Meditation PDFDocument8 pagesThe Abreviated Ajahn Brahm - Concise Instructions For Skillful Meditation PDFJean Bessaudou Jan BessNo ratings yet
- New Flowers - FlowerMedDocument5 pagesNew Flowers - FlowerMedAndré CamargoNo ratings yet
- Analiza PESTDocument16 pagesAnaliza PESTIoana Ciobanu100% (1)
- HB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiDocument23 pagesHB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiMudassar Roomi100% (1)
- Preparation of nursery and seed bedsDocument7 pagesPreparation of nursery and seed bedsShree PinnintiNo ratings yet
- Inflammatory Bowel DiseaseDocument27 pagesInflammatory Bowel DiseaseMihai VladescuNo ratings yet
- AmoniacoDocument2 pagesAmoniacoAlejandra Morales0% (1)
- Pre-Job Hazard AnalysisDocument4 pagesPre-Job Hazard AnalysisFiras HamanNo ratings yet
- MDocument47 pagesMKumara55No ratings yet
- En - Ineos Bichlor ElectrolyserDocument8 pagesEn - Ineos Bichlor Electrolyserbarun1977No ratings yet
- TheEconomist 2020 12 10Document296 pagesTheEconomist 2020 12 10merlindebergNo ratings yet
- Delhi-HC-Cruelty by WifeDocument19 pagesDelhi-HC-Cruelty by WifeSachin BansalNo ratings yet
- Nuclear Radioactivity WorksheetDocument3 pagesNuclear Radioactivity Worksheet14569874No ratings yet
- The Sinew (Tendino-Muscular) Meridians - Jade Institute ClassesDocument10 pagesThe Sinew (Tendino-Muscular) Meridians - Jade Institute ClassespanisajNo ratings yet
- ASME I & ASME VIII FundamentalsDocument55 pagesASME I & ASME VIII FundamentalsFabio Peres de Lima100% (2)
- CHALLENGES - IN - DEVELOPING - MARGINAL - FIELD - COMPLEXITY, - CO MPILATION - & - IMPROVEMENT - NEEDED - Nik - Edit - 3Document22 pagesCHALLENGES - IN - DEVELOPING - MARGINAL - FIELD - COMPLEXITY, - CO MPILATION - & - IMPROVEMENT - NEEDED - Nik - Edit - 3Wan Mohd ShaharizuanNo ratings yet
- PBR Design for Phthalic Anhydride Production (20k tons/yrDocument40 pagesPBR Design for Phthalic Anhydride Production (20k tons/yrAjay YadavNo ratings yet
- Food Fundamentals 10 - E - Margaret McWilliamsDocument497 pagesFood Fundamentals 10 - E - Margaret McWilliamspedropereza88No ratings yet
- Intelli Trac X1Document2 pagesIntelli Trac X1nadjibnetNo ratings yet
- CHN Notes SummaryDocument6 pagesCHN Notes SummaryAlec AnonNo ratings yet
- Procedures For Analysis of Citrus Products PDFDocument193 pagesProcedures For Analysis of Citrus Products PDFluis100% (2)
- Aims & ObjectiveDocument80 pagesAims & Objectivevishaldhande007No ratings yet
- Tie Systems: The Right Solution For All Wall Formwork: Waterproof Gas-Proof Fire Resistant Soundproof Radiation-ProofDocument16 pagesTie Systems: The Right Solution For All Wall Formwork: Waterproof Gas-Proof Fire Resistant Soundproof Radiation-Proofidesawy1982No ratings yet
- CH 5 - Cyprus RestaurantDocument15 pagesCH 5 - Cyprus RestaurantmazenfarhatNo ratings yet
- FAA Instrument Rating Oral Exam PrepDocument8 pagesFAA Instrument Rating Oral Exam Prepvino chandrakumarNo ratings yet
- Pharmacy Service VA Design Guide: Final DraftDocument75 pagesPharmacy Service VA Design Guide: Final DraftAhmad Gamal Elden MAhanyNo ratings yet