You might also like
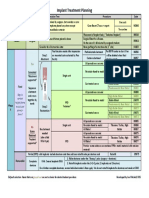
- Implant TX Plan GridDocument1 pageImplant TX Plan GridAhmed BadrNo ratings yet
- Ceu Revalida Ga Oa GPF OpfDocument97 pagesCeu Revalida Ga Oa GPF OpfPAULINE BERNARDONo ratings yet
- Creating Veneer Provisionals Using Silicone Matrices and Models by DentistryDocument11 pagesCreating Veneer Provisionals Using Silicone Matrices and Models by Dentistrycesar amaro100% (1)
- Wire BendingDocument165 pagesWire BendingArsalah Raffat96% (28)
- Marpe Miniscrew Assisted Rapid Palatal ExpansionDocument4 pagesMarpe Miniscrew Assisted Rapid Palatal Expansionaa bbNo ratings yet
- Med Oncology MCQDocument109 pagesMed Oncology MCQdrzika100% (8)
- 50 Landmark Papers in OmfsDocument313 pages50 Landmark Papers in OmfsNidhi Pandey67% (3)
- Bok:978 3 030 96874 8Document533 pagesBok:978 3 030 96874 8CarlosBaculimaNo ratings yet
- Original PDFDocument6 pagesOriginal PDFMamo AmmoNo ratings yet
- Surface Decontamination Protocols For Surgical Treatment of Peri-Implantitis A Systematic Review With Meta-AnalysisDocument18 pagesSurface Decontamination Protocols For Surgical Treatment of Peri-Implantitis A Systematic Review With Meta-Analysiskaue franco100% (1)
- Contemporary Periodontal Surgery: An Illustrated Guide to the Art behind the ScienceFrom EverandContemporary Periodontal Surgery: An Illustrated Guide to the Art behind the ScienceNo ratings yet
- Surgery Without Papilla Incision: Tunneling Ap Procedures in Plastic Periodontal and Implant SurgeryDocument27 pagesSurgery Without Papilla Incision: Tunneling Ap Procedures in Plastic Periodontal and Implant SurgeryankitaNo ratings yet
- Sync2 Specific Competences Tests LRW U7Document11 pagesSync2 Specific Competences Tests LRW U7mfrancodlrubiaNo ratings yet
- The Historical Evolution of Dental Impression MaterialsDocument11 pagesThe Historical Evolution of Dental Impression MaterialsHassanein Al-Hamdani100% (1)
- Liu 2021Document11 pagesLiu 2021jcNo ratings yet
- 1 R Cambios OSEOS POSEXTRACCIONDocument16 pages1 R Cambios OSEOS POSEXTRACCIONfeli.riam24No ratings yet
- Kang2015 KimDocument14 pagesKang2015 KimIkram LyaNo ratings yet
- Untitled 3Document10 pagesUntitled 3Satya AsatyaNo ratings yet
- Scaling Teeth TechniquesDocument12 pagesScaling Teeth TechniqueshanyNo ratings yet
- Comparison of Microsurgical and Conventional Open Flap DebridementDocument9 pagesComparison of Microsurgical and Conventional Open Flap DebridementNoemi LukacsNo ratings yet
- Modern Surgery-First Approach Concept in Cleft-Orthognathic Surgery A Comparative Cohort Study With 3D Quantitative Analysis of Surgical-Occlusion SetupDocument22 pagesModern Surgery-First Approach Concept in Cleft-Orthognathic Surgery A Comparative Cohort Study With 3D Quantitative Analysis of Surgical-Occlusion Setuppedroalmeida37920No ratings yet
- Meza-Mauricio 2021. b-3-6Document12 pagesMeza-Mauricio 2021. b-3-6MARIA ANTONIETA RODRIGUEZ GALECIONo ratings yet
- Grupo 2 Sinjab 2018Document6 pagesGrupo 2 Sinjab 2018m.castillo11No ratings yet
- lim2017Document10 pageslim2017Juliana Gomes BarretoNo ratings yet
- CAT Article 2Document5 pagesCAT Article 2Daal ChawlNo ratings yet
- Ijmse 2015 Vol 2 Issue 4 Page 154-166Document13 pagesIjmse 2015 Vol 2 Issue 4 Page 154-166Sarra TekayaNo ratings yet
- Japid 14 26Document6 pagesJapid 14 26rikaNo ratings yet
- Influence of Suturing Techniques On WounDocument4 pagesInfluence of Suturing Techniques On WounThùy Trang NguyễnNo ratings yet
- 1 s2.0 S0278239108011452 MainDocument7 pages1 s2.0 S0278239108011452 MainAshish VyasNo ratings yet
- Role of Thin Gingival Phenotype and Inadequate Keratinized Mucosa Width ( - 2 MM) As Risk Indicators For Peri Implantitis and Peri Implant MucositisDocument10 pagesRole of Thin Gingival Phenotype and Inadequate Keratinized Mucosa Width ( - 2 MM) As Risk Indicators For Peri Implantitis and Peri Implant MucositisAdil KaukabNo ratings yet
- Qi 47 8 Sculean p653Document7 pagesQi 47 8 Sculean p653zubicvilaNo ratings yet
- PEMF - Mandibular FractureDocument7 pagesPEMF - Mandibular FractureMáté TóthNo ratings yet
- Comparison of Periosteal Pedicle Graft and Subepithelial Connective Tissue Graft For The Treatment of Gingival Recession DefectsDocument7 pagesComparison of Periosteal Pedicle Graft and Subepithelial Connective Tissue Graft For The Treatment of Gingival Recession DefectsEsha AroraNo ratings yet
- Over Sem EsplintarDocument9 pagesOver Sem EsplintarClaudia BrilhanteNo ratings yet
- Periodontology 2000 - 2003 - SANZ - Focus On Furcation Defects Guided Tissue RegenerationDocument21 pagesPeriodontology 2000 - 2003 - SANZ - Focus On Furcation Defects Guided Tissue Regenerationcarla lopezNo ratings yet
- Decision Makin in Root Coverage Procedures For Esthetic OutcomesDocument11 pagesDecision Makin in Root Coverage Procedures For Esthetic OutcomesZelinschi Dragos ChristianNo ratings yet
- 385 PDFDocument10 pages385 PDFAly OsmanNo ratings yet
- Treatment Outcomes For Mandibular Mini-Implant-Retained Overdentures: A Systematic ReviewDocument8 pagesTreatment Outcomes For Mandibular Mini-Implant-Retained Overdentures: A Systematic ReviewPhung NguyenNo ratings yet
- Art 1Document38 pagesArt 1Juan José Chacón BalderramaNo ratings yet
- Retrospective Study of Pulpectomy With Vitapex and LSTR With Three Antibiotics Combination (3mix) For Non-Vital Pulp Treatment in Primary TeethDocument10 pagesRetrospective Study of Pulpectomy With Vitapex and LSTR With Three Antibiotics Combination (3mix) For Non-Vital Pulp Treatment in Primary TeethJavier Farias VeraNo ratings yet
- DMD6B Group 3 PeriodonticsDocument40 pagesDMD6B Group 3 PeriodonticsJAMMILA CLAIRE REANo ratings yet
- Effectiveness and Efficacy of Thermoformed and 3D Printed PDFDocument7 pagesEffectiveness and Efficacy of Thermoformed and 3D Printed PDFGhimpu DanielaNo ratings yet
- Chirurgie Endo Topics With Cover Page v2Document263 pagesChirurgie Endo Topics With Cover Page v2Saida SisiliaNo ratings yet
- The Effect of Resin Infiltration On Proximal Caries Lesions in Primary and Permanent Teeth. A Systematic Review and Meta-Analysis of Clinical TrialsDocument10 pagesThe Effect of Resin Infiltration On Proximal Caries Lesions in Primary and Permanent Teeth. A Systematic Review and Meta-Analysis of Clinical Trialsmae leeNo ratings yet
- 10 1111@cid 12881Document9 pages10 1111@cid 12881everaldocruzNo ratings yet
- Surgical Versus Non-Surgical Treatment of Mandibular Condylar Fractures: A Meta-AnalysisDocument22 pagesSurgical Versus Non-Surgical Treatment of Mandibular Condylar Fractures: A Meta-AnalysisHNo ratings yet
- Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocument6 pagesJournal of Oral and Maxillofacial Surgery, Medicine, and PathologyVirginia BujorNo ratings yet
- 10.1186@s40729 019 0157 7Document9 pages10.1186@s40729 019 0157 7mlnunezNo ratings yet
- Surgical Treatment of Peri-Implantitis: 3 - Year Results From A Randomized Controlled Clinical TrialDocument10 pagesSurgical Treatment of Peri-Implantitis: 3 - Year Results From A Randomized Controlled Clinical TrialFabian SanabriaNo ratings yet
- Clinical Oral Implants Res - 2022 - Jung - Effect of Peri Implant Mucosal Thickness On Esthetic Outcomes and The EfficacyDocument9 pagesClinical Oral Implants Res - 2022 - Jung - Effect of Peri Implant Mucosal Thickness On Esthetic Outcomes and The EfficacyGustavo BerrioNo ratings yet
- Comparación de Las Tasas de Complicaciones A 2 Años Entre Técnicas Comunes para La Reconstrucción Mamaria PosmastectomíaDocument14 pagesComparación de Las Tasas de Complicaciones A 2 Años Entre Técnicas Comunes para La Reconstrucción Mamaria PosmastectomíadiogenesNo ratings yet
- Minimal Invasiveness in The Reconstructive Treatment of Peri-Implantitis DefectsDocument18 pagesMinimal Invasiveness in The Reconstructive Treatment of Peri-Implantitis Defectsmahesh kumarNo ratings yet
- Clinical Benefits of Ridge Preservation For Implant Placement Compared To Natural Healing in Maxillary Teeth - A Retrospective StudyDocument10 pagesClinical Benefits of Ridge Preservation For Implant Placement Compared To Natural Healing in Maxillary Teeth - A Retrospective StudyCamilo Andrés Sabogal ArguelloNo ratings yet
- Jerd 12812Document15 pagesJerd 12812snkidNo ratings yet
- Maxillofacial Prosthetic Rehabilitation A SurveyDocument7 pagesMaxillofacial Prosthetic Rehabilitation A Surveyirfan dNo ratings yet
- Mohsenmalekigorji A 10 598 6 dd9233c - fc15bbDocument10 pagesMohsenmalekigorji A 10 598 6 dd9233c - fc15bbmohsenNo ratings yet
- Decontamination of Titanium Implant Surface and Re-Osseointegration To Treat Peri-Implantitis: A Literature ReviewDocument12 pagesDecontamination of Titanium Implant Surface and Re-Osseointegration To Treat Peri-Implantitis: A Literature ReviewAlejandra Del PilarNo ratings yet
- Facial Implant Gingival Level and Thickness Changes Following Maxillary AnteriorDocument10 pagesFacial Implant Gingival Level and Thickness Changes Following Maxillary AnteriorFelipe CastroNo ratings yet
- Evaluation of Open Bite Closure Using Clear AligneDocument9 pagesEvaluation of Open Bite Closure Using Clear AligneManuel CastilloNo ratings yet
- Defectos de Furca y Regeneracion TisularDocument21 pagesDefectos de Furca y Regeneracion TisularSebastián BernalNo ratings yet
- 203 PDFDocument8 pages203 PDFJambul Wak Wak WakNo ratings yet
- Treatment For Adult Mandibular Condylar Process Fractures - A Network Meta-Analysis of Randomized Clinical TrialsDocument18 pagesTreatment For Adult Mandibular Condylar Process Fractures - A Network Meta-Analysis of Randomized Clinical TrialsBedah Mulut dan Maksilofasial 2023No ratings yet
- PROTOCOLO de Carga de Coronas Sobre ImplanteDocument17 pagesPROTOCOLO de Carga de Coronas Sobre ImplanteJohnny CHNo ratings yet
- Fficacy and Patient's Acceptance of Alternative: E Methods For Caries Removal-A Systematic ReviewDocument26 pagesFficacy and Patient's Acceptance of Alternative: E Methods For Caries Removal-A Systematic ReviewDarell Josue Valdez AquinoNo ratings yet
- Intramarrow PenetrationDocument20 pagesIntramarrow PenetrationsutriNo ratings yet
- Surgery-First Approach in Orthognathic PatientsDocument15 pagesSurgery-First Approach in Orthognathic PatientsAlvaro jose Uribe TamaraNo ratings yet
- Aatika 8Document7 pagesAatika 8Abhishek GuptaNo ratings yet
- Comparison of Two Incision Designs For Surgical ReDocument5 pagesComparison of Two Incision Designs For Surgical ReSooraj SNo ratings yet
- Soft Tissue Phenotype Modifcation Impacts On Peri Implant Stability - A Comparative Cohort Study - HL Wang 2022Document12 pagesSoft Tissue Phenotype Modifcation Impacts On Peri Implant Stability - A Comparative Cohort Study - HL Wang 2022Claudio GuzmanNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Working OnDocument1 pageWorking OnAhmed BadrNo ratings yet
- Successful Intraoral Film RadiographyDocument10 pagesSuccessful Intraoral Film RadiographyAhmed BadrNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- 6038ed9dcef5d IJAR-35170Document5 pages6038ed9dcef5d IJAR-35170Ahmed BadrNo ratings yet
- 1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureDocument4 pages1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureingronaldNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- M Vista in Class 3Document12 pagesM Vista in Class 3Ahmed BadrNo ratings yet
- AA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Document10 pagesAA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Ahmed BadrNo ratings yet
- Korkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeDocument10 pagesKorkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeAhmed BadrNo ratings yet
- Prognosis 2021Document10 pagesPrognosis 2021Ahmed BadrNo ratings yet
- Vista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpDocument7 pagesVista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpAhmed BadrNo ratings yet
- Combinin Tunnel With Douple PapillaDocument12 pagesCombinin Tunnel With Douple PapillaAhmed BadrNo ratings yet
- Content ServerDocument10 pagesContent ServerAhmed BadrNo ratings yet
- Guidelines For Immediate ImplanttDocument11 pagesGuidelines For Immediate ImplanttAhmed BadrNo ratings yet
- 22 CE CreditsDocument11 pages22 CE CreditsAhmed BadrNo ratings yet
- 5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Document21 pages5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Ahmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- Periodontal Plastic Surgery For The Management of Altered Passive EruptionDocument3 pagesPeriodontal Plastic Surgery For The Management of Altered Passive EruptionAhmed BadrNo ratings yet
- Sticky BoneDocument7 pagesSticky BoneAhmed BadrNo ratings yet
- 3A 2B Immediate ImplantDocument6 pages3A 2B Immediate ImplantAhmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- 2010 Sofia Aroca SoteloDocument52 pages2010 Sofia Aroca SoteloAhmed BadrNo ratings yet
- A Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureDocument11 pagesA Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureAhmed BadrNo ratings yet
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocument5 pagesMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNo ratings yet
- Gingival Diseases - Their Aetiology, Prevention and Treatment PDFDocument246 pagesGingival Diseases - Their Aetiology, Prevention and Treatment PDFnaresh sharma0% (1)
- Ipa Extentions Unicode 14.0 U0250Document6 pagesIpa Extentions Unicode 14.0 U0250ygurseyNo ratings yet
- Fiber Post Vs Metal PostDocument13 pagesFiber Post Vs Metal PostOdontología UnibeNo ratings yet
- Dental InsuranceDocument3 pagesDental InsurancemcrblxbxiaeqdyzxjoNo ratings yet
- Mechanics For Gummy Smile CorrectionDocument20 pagesMechanics For Gummy Smile Correctionsandeep kumar senguptaNo ratings yet
- Anatomi EyelidDocument9 pagesAnatomi EyelidFelyana GunawanNo ratings yet
- Metabolic Conditions Didc ClassDocument14 pagesMetabolic Conditions Didc ClassSiddique SaandNo ratings yet
- Learn tooth anatomy with flashcardsDocument4 pagesLearn tooth anatomy with flashcardsVenetia RamdathNo ratings yet
- SEO-Optimized Title for Dental Pulp and Endodontics DocumentDocument7 pagesSEO-Optimized Title for Dental Pulp and Endodontics DocumentVicka RainNo ratings yet
- Project Report On ColgateDocument44 pagesProject Report On ColgateSATAN REVOLT67% (3)
- 1aomsi Consent Form FinalDocument8 pages1aomsi Consent Form FinalPaul MathaiNo ratings yet
- Rguhs Thesis Topics in PeriodonticsDocument5 pagesRguhs Thesis Topics in PeriodonticsSara Perez100% (2)
- 16 Anjali Gheware PDFDocument4 pages16 Anjali Gheware PDFRahulLife'sNo ratings yet
- Dental College Inspection ReportDocument16 pagesDental College Inspection ReportSatya AsatyaNo ratings yet
- Ear Nose Throat Exam Features GuideDocument4 pagesEar Nose Throat Exam Features GuideMawj MandwieNo ratings yet
- Denture Stomatitis Causes and TreatmentDocument4 pagesDenture Stomatitis Causes and TreatmentNovia SillaNo ratings yet
- Laser Physics and Application in Fixed ProsthodonticsDocument8 pagesLaser Physics and Application in Fixed ProsthodonticsJoelle OthmanNo ratings yet
- Nomenclature of A GearDocument3 pagesNomenclature of A GearRajandra Verma100% (1)
- Analysis of Surface Roughness of Enamel and Dentin After Laser TreatmentDocument10 pagesAnalysis of Surface Roughness of Enamel and Dentin After Laser TreatmentmustafaNo ratings yet
- LUSSI, 2019. The Use of Fluoride For The Prevention of Dental Erosion and Erosive Tooth Wear in Children and Adolescents PDFDocument11 pagesLUSSI, 2019. The Use of Fluoride For The Prevention of Dental Erosion and Erosive Tooth Wear in Children and Adolescents PDFJohnatan MeirelesNo ratings yet
- Art 2 Protesis RemovibleDocument14 pagesArt 2 Protesis RemovibleLaurita Ayala ChiquilloNo ratings yet
- 2020 Naldeman Premature Loss of Primary Anterior TeethDocument26 pages2020 Naldeman Premature Loss of Primary Anterior TeethDiego Andres Hincapie HerreraNo ratings yet
- Clinical Assessment of Short Implants Retsining Removsble Partial DenturesDocument7 pagesClinical Assessment of Short Implants Retsining Removsble Partial DenturesLouis HutahaeanNo ratings yet