You might also like
- Long-Term Skeletal and DentoalveolarDocument10 pagesLong-Term Skeletal and DentoalveolaremadNo ratings yet
- Jurnal Bedah OnkologiDocument7 pagesJurnal Bedah OnkologiFieraNo ratings yet
- Estabilidad Clase IiiDocument5 pagesEstabilidad Clase Iiimarcela0426No ratings yet
- Aroca 2018Document16 pagesAroca 2018Mauro Santiago EspinozaNo ratings yet
- 4) 2023 Surgical Management of Ostomy ComplicationsDocument16 pages4) 2023 Surgical Management of Ostomy ComplicationsAnnaKnakNo ratings yet
- Meza-Mauricio 2021. b-3-6Document12 pagesMeza-Mauricio 2021. b-3-6MARIA ANTONIETA RODRIGUEZ GALECIONo ratings yet
- (2019) Pini Prato. EVOLUCIÓN TÉCNICAS MUCOGINGIVALDocument7 pages(2019) Pini Prato. EVOLUCIÓN TÉCNICAS MUCOGINGIVALDaniel EchegarayNo ratings yet
- Maxillary Protraction With Rapid Maxillary Expansion and Facemask Versus Skeletal Anchorage With Mini-Implants in Class III Patients A Non-Randomized Clinical TrialDocument11 pagesMaxillary Protraction With Rapid Maxillary Expansion and Facemask Versus Skeletal Anchorage With Mini-Implants in Class III Patients A Non-Randomized Clinical TrialMariana SantosNo ratings yet
- Management of Mandibular Third Molar Surgery To PRDocument5 pagesManagement of Mandibular Third Molar Surgery To PRVilmar Faria de AlvarengaNo ratings yet
- Epidemiological Characterization of Tibial Plateau FracturesDocument7 pagesEpidemiological Characterization of Tibial Plateau FracturesArmando RodriguezNo ratings yet
- AnnMaxillofacSurg62204-7504388 020504Document6 pagesAnnMaxillofacSurg62204-7504388 020504mascoNo ratings yet
- Qureshi 2019Document8 pagesQureshi 2019Jefferson RuizNo ratings yet
- Practical ApplicationsDocument9 pagesPractical ApplicationsCristian OneaNo ratings yet
- Mandibular Third Molar Extraction: Perceived Surgical Difficulty in Relation To Professional TrainingDocument12 pagesMandibular Third Molar Extraction: Perceived Surgical Difficulty in Relation To Professional TrainingKemas IrsanNo ratings yet
- Microneedles in Clinical Practice - An Exploratory Study Into The Opinions of Healthcare Professionals and The PublicDocument12 pagesMicroneedles in Clinical Practice - An Exploratory Study Into The Opinions of Healthcare Professionals and The Publicapt Muthia Fadhila MFarmNo ratings yet
- Class. of Maxillectomy DefectsDocument10 pagesClass. of Maxillectomy DefectsJASPREETKAUR0410No ratings yet
- 130 / 5.000 Resultados de tradução Resultado da tradução Reconstrução do cume alveolar com malhas de titânio e colocação simultânea de implantes: Um estudo clínico retrospectivo e multicêntricoDocument13 pages130 / 5.000 Resultados de tradução Resultado da tradução Reconstrução do cume alveolar com malhas de titânio e colocação simultânea de implantes: Um estudo clínico retrospectivo e multicêntricoJuliana Gomes BarretoNo ratings yet
- 10.1186@s40729 019 0157 7Document9 pages10.1186@s40729 019 0157 7mlnunezNo ratings yet
- Minimal Invasiveness in The Reconstructive Treatment of Peri-Implantitis DefectsDocument18 pagesMinimal Invasiveness in The Reconstructive Treatment of Peri-Implantitis Defectsmahesh kumarNo ratings yet
- Qi 47 8 Sculean p653Document7 pagesQi 47 8 Sculean p653zubicvilaNo ratings yet
- Journal of Periodontology - 2015 - Chambrone - Periodontal Soft Tissue Root Coverage Procedures a Systematic Review From (1)Document44 pagesJournal of Periodontology - 2015 - Chambrone - Periodontal Soft Tissue Root Coverage Procedures a Systematic Review From (1)HONG JIN TANNo ratings yet
- JCDP 20 957Document6 pagesJCDP 20 957Priyanka GandhiNo ratings yet
- Meyer Lu Eckel 2012Document5 pagesMeyer Lu Eckel 2012Ahmed El SharkawyNo ratings yet
- 203 PDFDocument8 pages203 PDFJambul Wak Wak WakNo ratings yet
- Jurnal 1Document7 pagesJurnal 1Gilang Kurnia HirawatiNo ratings yet
- Novel Methodologies and Technologies To Assess Mid-Palatal Suture Maturation: A Systematic ReviewDocument15 pagesNovel Methodologies and Technologies To Assess Mid-Palatal Suture Maturation: A Systematic ReviewnicoNo ratings yet
- Stability Factors After Double-Jaw Surgery in Class III MalocclusionDocument12 pagesStability Factors After Double-Jaw Surgery in Class III Malocclusionortodoncia 2022No ratings yet
- Registered Nurses Knowledge On Wound CareDocument35 pagesRegistered Nurses Knowledge On Wound Careyarec79954No ratings yet
- How To Intervene in The Caries Process: Proximal Caries in Adolescents and Adults - A Systematic Review and Meta-AnalysisDocument14 pagesHow To Intervene in The Caries Process: Proximal Caries in Adolescents and Adults - A Systematic Review and Meta-AnalysisLaura ImreNo ratings yet
- Sternectomy Bota Et AlDocument10 pagesSternectomy Bota Et AlOli BotaNo ratings yet
- Fsurg 10 1151327Document7 pagesFsurg 10 1151327theomnagarowner2811No ratings yet
- Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocument6 pagesJournal of Oral and Maxillofacial Surgery, Medicine, and PathologyVirginia BujorNo ratings yet
- Regeneracion AAPDocument23 pagesRegeneracion AAPSebastián BernalNo ratings yet
- Criteria For Root Coverage ProceduresDocument14 pagesCriteria For Root Coverage ProceduresGabriel OgandoNo ratings yet
- Efeito das membranas de colágeno reticuladas versus não reticuladas no osso: uma revisão sistemáticaDocument10 pagesEfeito das membranas de colágeno reticuladas versus não reticuladas no osso: uma revisão sistemáticaJuliana Gomes BarretoNo ratings yet
- Xenogeneic Collagen Matrix vs. Connective Tissue Graft For The Treatment of Multiple Gingival Recession: A Systematic Review and Meta AnalysisDocument24 pagesXenogeneic Collagen Matrix vs. Connective Tissue Graft For The Treatment of Multiple Gingival Recession: A Systematic Review and Meta AnalysisDANTE DELEGUERYNo ratings yet
- SSRN Id4283125Document19 pagesSSRN Id4283125sasi dharanNo ratings yet
- (2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKDocument13 pages(2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKBárbara Meza Lewis100% (1)
- Time To Surgery and Survival in Breast Cancer: Research Open AccessDocument8 pagesTime To Surgery and Survival in Breast Cancer: Research Open AccessTatianaPadillaNo ratings yet
- Classification System For Full EdentulismDocument4 pagesClassification System For Full EdentulismmandakinimohanNo ratings yet
- Cervical Margin Relocation in Indirect Adhesive Re - 2018 - Journal of ProsthodoDocument8 pagesCervical Margin Relocation in Indirect Adhesive Re - 2018 - Journal of ProsthodoIvy MedNo ratings yet
- Surgery JournalDocument7 pagesSurgery JournalJane Arian BerzabalNo ratings yet
- Journal of Prosthodontic Research: Jelena Juloski, Serhat Köken, Marco FerrariDocument8 pagesJournal of Prosthodontic Research: Jelena Juloski, Serhat Köken, Marco FerrariAarónNo ratings yet
- Journal of Prosthodontic Research: Jelena Juloski, Serhat Köken, Marco FerrariDocument8 pagesJournal of Prosthodontic Research: Jelena Juloski, Serhat Köken, Marco FerrariAli Al-QaysiNo ratings yet
- Pneumatic Vitreolysis Versus Vitrectomy For The Treatment of Vitreomacular Traction Syndrome and Macular Holes Complication Analysis and Systematic Review With Meta-Analysis of Functional OutcomesDocument16 pagesPneumatic Vitreolysis Versus Vitrectomy For The Treatment of Vitreomacular Traction Syndrome and Macular Holes Complication Analysis and Systematic Review With Meta-Analysis of Functional Outcomesmistic0No ratings yet
- PB11 4678 R2Document15 pagesPB11 4678 R2CAMILO ANDRÉS SABOGAL ARGUELLONo ratings yet
- Int J of Nursing Knowl - 2021 - Capilla D AzDocument9 pagesInt J of Nursing Knowl - 2021 - Capilla D AzSuharyatno nizarNo ratings yet
- Mascara Facial 2Document7 pagesMascara Facial 2afperdomo8403No ratings yet
- Int Endodontic J - 2022 - Ordinola Zapata - Present Status and Future Directions of Intracanal MedicamentsDocument24 pagesInt Endodontic J - 2022 - Ordinola Zapata - Present Status and Future Directions of Intracanal Medicamentspau casseNo ratings yet
- Kinesio TapingDocument19 pagesKinesio TapingMuhammad Azhar ImranNo ratings yet
- Appendicitis During The COVID-19 Pandemic: Lessons Learnt From A District General HospitalDocument6 pagesAppendicitis During The COVID-19 Pandemic: Lessons Learnt From A District General HospitalAzam alausyNo ratings yet
- Minimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported OutcomeDocument17 pagesMinimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported Outcomemahesh kumarNo ratings yet
- Non-Medial Infectious Orbital Cellulitis: Etiology, Causative Organisms, Radiologic Findings, Management and ComplicationsDocument11 pagesNon-Medial Infectious Orbital Cellulitis: Etiology, Causative Organisms, Radiologic Findings, Management and ComplicationsPutri Sari DewiNo ratings yet
- Treatment Results For Patients With Squamous-Cell Carcinoma of The Anus, A Single Institution Retrospective AnalysisDocument10 pagesTreatment Results For Patients With Squamous-Cell Carcinoma of The Anus, A Single Institution Retrospective AnalysisJENIFER KARINA PUTZ LORENZINo ratings yet
- ArticleDocument9 pagesArticleAna Lazar IvanNo ratings yet
- Importance of Periodontal Phenotype in Periodontics and Restorative Dentistry: A Systematic ReviewDocument10 pagesImportance of Periodontal Phenotype in Periodontics and Restorative Dentistry: A Systematic ReviewNawaf RuwailiNo ratings yet
- Soft Tissue Augmentation Techniques in Implants Placed and Provisionalized Immediately. A Systematic Review.Document13 pagesSoft Tissue Augmentation Techniques in Implants Placed and Provisionalized Immediately. A Systematic Review.andreita_loppNo ratings yet
- Jurnal PlastiksDocument5 pagesJurnal PlastiksbdhNo ratings yet
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceFrom EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- 6038ed9dcef5d IJAR-35170Document5 pages6038ed9dcef5d IJAR-35170Ahmed BadrNo ratings yet
- Working OnDocument1 pageWorking OnAhmed BadrNo ratings yet
- Med Oncology MCQDocument109 pagesMed Oncology MCQdrzika100% (8)
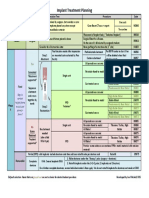
- Implant TX Plan GridDocument1 pageImplant TX Plan GridAhmed BadrNo ratings yet
- 1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureDocument4 pages1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureingronaldNo ratings yet
- Prognosis 2021Document10 pagesPrognosis 2021Ahmed BadrNo ratings yet
- Original PDFDocument6 pagesOriginal PDFMamo AmmoNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- Successful Intraoral Film RadiographyDocument10 pagesSuccessful Intraoral Film RadiographyAhmed BadrNo ratings yet
- Sticky BoneDocument7 pagesSticky BoneAhmed BadrNo ratings yet
- Vista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpDocument7 pagesVista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpAhmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- MetaanalysisDocument12 pagesMetaanalysisAhmed BadrNo ratings yet
- Content ServerDocument10 pagesContent ServerAhmed BadrNo ratings yet
- Korkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeDocument10 pagesKorkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeAhmed BadrNo ratings yet
- Combinin Tunnel With Douple PapillaDocument12 pagesCombinin Tunnel With Douple PapillaAhmed BadrNo ratings yet
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocument5 pagesMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNo ratings yet
- 5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Document21 pages5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Ahmed BadrNo ratings yet
- Guidelines For Immediate ImplanttDocument11 pagesGuidelines For Immediate ImplanttAhmed BadrNo ratings yet
- Periodontal Plastic Surgery For The Management of Altered Passive EruptionDocument3 pagesPeriodontal Plastic Surgery For The Management of Altered Passive EruptionAhmed BadrNo ratings yet
- 22 CE CreditsDocument11 pages22 CE CreditsAhmed BadrNo ratings yet
- 3A 2B Immediate ImplantDocument6 pages3A 2B Immediate ImplantAhmed BadrNo ratings yet
- AA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Document10 pagesAA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Ahmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- 2010 Sofia Aroca SoteloDocument52 pages2010 Sofia Aroca SoteloAhmed BadrNo ratings yet
- A Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureDocument11 pagesA Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureAhmed BadrNo ratings yet
- ArticulatorsDocument52 pagesArticulatorsBharath KondaveetiNo ratings yet
- Brenda Gamez, SDH: Rotation ExperiencesDocument2 pagesBrenda Gamez, SDH: Rotation Experiencesapi-507804349No ratings yet
- 1.gagging and Its Management in Prosthodontic PatientsDocument25 pages1.gagging and Its Management in Prosthodontic PatientsMithileshwari Patil100% (1)
- Choose The Correct Answer: Choose The Correct Answer:: Retention & StabilityDocument29 pagesChoose The Correct Answer: Choose The Correct Answer:: Retention & StabilityMostafa ElsayedNo ratings yet
- Maxillary Canine Transpositions: Classification, Prevalence and TreatmentDocument8 pagesMaxillary Canine Transpositions: Classification, Prevalence and Treatmentjohnmax100% (2)
- 020 Over Dentures.Document60 pages020 Over Dentures.Khan MustafaNo ratings yet
- MCN Oral Surgery Referral Guidelines For Gdps Oct 2022V1 001Document24 pagesMCN Oral Surgery Referral Guidelines For Gdps Oct 2022V1 001Triman AhluwaliaNo ratings yet
- Ref1. Applications of Propolis in Dentistry, A ReviewDocument8 pagesRef1. Applications of Propolis in Dentistry, A ReviewbungaNo ratings yet
- From Birth Till Palatoplasty Prosthetic.20Document5 pagesFrom Birth Till Palatoplasty Prosthetic.20Maria FernandaNo ratings yet
- Tieng Anh 5 Unit 11 ReviewDocument19 pagesTieng Anh 5 Unit 11 Review20140513- Hoàng Thị Giang - TH Bích Sơn Việt YênNo ratings yet
- Measure Posterior Teeth Arrangement With Intercondylar DistanceDocument5 pagesMeasure Posterior Teeth Arrangement With Intercondylar DistanceBharath KondaveetiNo ratings yet
- 3MIXTATINDocument45 pages3MIXTATINShameena KnNo ratings yet
- Chola Ms Family Healthline Insurance PolicyDocument40 pagesChola Ms Family Healthline Insurance Policyhappy39No ratings yet
- Assessing Periodontal DiseaseDocument4 pagesAssessing Periodontal Diseaseمؤمل رياض سعد كاظمNo ratings yet
- Evaluation of Soft-Tissue Changes in Young Adults Treated With The Forsus Fatigue-Resistant DeviceDocument11 pagesEvaluation of Soft-Tissue Changes in Young Adults Treated With The Forsus Fatigue-Resistant DeviceDominikaSkórkaNo ratings yet
- Comparing The OutcomeDocument4 pagesComparing The OutcomeHafiz RabbiNo ratings yet
- The Effectiveness of Stem Cells Grafting On Regeneration of Dental Pulp: A Systematic Review and Meta-AnalysisDocument11 pagesThe Effectiveness of Stem Cells Grafting On Regeneration of Dental Pulp: A Systematic Review and Meta-AnalysisIJAR JOURNALNo ratings yet
- AIR AbrasionDocument5 pagesAIR Abrasionzubair ahmedNo ratings yet
- Referat EnglezaDocument3 pagesReferat EnglezaMira SlavNo ratings yet
- 11-Try-In and Cementation of CrownsDocument10 pages11-Try-In and Cementation of CrownsElias EspinozaNo ratings yet
- Prevalence of Iatrogenic Perforations According To Their Location and Affected Root SurfacesDocument7 pagesPrevalence of Iatrogenic Perforations According To Their Location and Affected Root SurfacesIJAR JOURNALNo ratings yet
- Ca. Ca.: - .,.1b1h1tlesDocument179 pagesCa. Ca.: - .,.1b1h1tleshNo ratings yet
- Mcqs PDFDocument12 pagesMcqs PDFAmrit63% (8)
- 1.postnatal Growth and DevelopmentDocument135 pages1.postnatal Growth and DevelopmentAJPEDO LIFENo ratings yet
- Review of Matrix Metalloproteinases' Effect On The Hybrid Dentin Bond Layer Stability and Chlorhexidine Clinical Use To Prevent Bond FailureDocument6 pagesReview of Matrix Metalloproteinases' Effect On The Hybrid Dentin Bond Layer Stability and Chlorhexidine Clinical Use To Prevent Bond FailureAlex KwokNo ratings yet
- Poor Personal Hygiene PriorityDocument4 pagesPoor Personal Hygiene PrioritycamziiiNo ratings yet
- NIDCR Dental Clinical Research FellowshipDocument2 pagesNIDCR Dental Clinical Research FellowshipGulara KerimovaNo ratings yet
- 41 ST JC - SindhuDocument8 pages41 ST JC - SindhuDadi SindhuNo ratings yet
- Chronological Age Estimation Based On Mandibular Third Molar Development From Digital Panoramic Radiograph in A South Kerala PopulDocument3 pagesChronological Age Estimation Based On Mandibular Third Molar Development From Digital Panoramic Radiograph in A South Kerala PopulSyabilla FatihNo ratings yet
- 3D Technologies For Precision in Orthodontics - 2018 - Seminars in Orthodontics PDFDocument7 pages3D Technologies For Precision in Orthodontics - 2018 - Seminars in Orthodontics PDFOmy J. CruzNo ratings yet