You might also like
- Taha 2017Document5 pagesTaha 2017zaheerbdsNo ratings yet
- JIAP January 2015 - A Novel Surgical Approach For Treatment of Class II Furcation Defects Using Marginal Periosteal MembraneDocument12 pagesJIAP January 2015 - A Novel Surgical Approach For Treatment of Class II Furcation Defects Using Marginal Periosteal Membranemạnh nguyễn xuânNo ratings yet
- Ahmed ENDO Vol6 Iss2Document18 pagesAhmed ENDO Vol6 Iss2Lupu SebastianNo ratings yet
- FMR With SplintDocument5 pagesFMR With SplintDr Tarak ChavadaNo ratings yet
- BCR 2013 200316Document4 pagesBCR 2013 200316ay lmaoNo ratings yet
- Letters To The Editor: Orthodontics and The Repair of Gingival RecessionsDocument1 pageLetters To The Editor: Orthodontics and The Repair of Gingival RecessionsAlexandraGuajánNo ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument10 pagesThe International Journal of Periodontics & Restorative DentistryLuis BeltranNo ratings yet
- Comparison of Orthodontic Techniques Used ForDocument5 pagesComparison of Orthodontic Techniques Used ForAdina SerbanNo ratings yet
- Jurnal 3Document5 pagesJurnal 3ayu augustineNo ratings yet
- OsteomaDocument4 pagesOsteomaAnjungAdelNo ratings yet
- Assessment and Management of Endo-Periodontal Lesions: DentistryDocument12 pagesAssessment and Management of Endo-Periodontal Lesions: Dentistryedgar curayNo ratings yet
- Jurnal 3Document5 pagesJurnal 3ayu augustineNo ratings yet
- Class II Deep BiteDocument12 pagesClass II Deep BitehabeebNo ratings yet
- Carlsson 1998Document7 pagesCarlsson 1998gbaez.88No ratings yet
- Multidisciplinary Management and Pulp Vitality Preservation of A Tooth With Extensive Iatrogenic Furcal Root Perforation and Biologic Width ViolationDocument6 pagesMultidisciplinary Management and Pulp Vitality Preservation of A Tooth With Extensive Iatrogenic Furcal Root Perforation and Biologic Width ViolationpoojaNo ratings yet
- Status TMD Pasien GTPDocument7 pagesStatus TMD Pasien GTPzkdlinspaceNo ratings yet
- JurnalDocument4 pagesJurnalAisah AisahNo ratings yet
- 826-Abstract, Key Words, Introduction and Article Text and References-6236-1!10!20230324Document4 pages826-Abstract, Key Words, Introduction and Article Text and References-6236-1!10!20230324Ketut SariasihNo ratings yet
- Healing of Large Periapical Lesion A Non-Surgical EndodonticDocument5 pagesHealing of Large Periapical Lesion A Non-Surgical EndodonticmeryemeNo ratings yet
- (2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKDocument13 pages(2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKBárbara Meza Lewis100% (1)
- Recesion TraducirDocument11 pagesRecesion TraducirsolangeNo ratings yet
- 12 371 sr1Document9 pages12 371 sr1iqbalNo ratings yet
- ADDS AmeloblastomaDocument10 pagesADDS AmeloblastomakaarlaamendezNo ratings yet
- Classification of Facial Peri-Implant Soft Tissue Zucchelli 2019 ColDocument9 pagesClassification of Facial Peri-Implant Soft Tissue Zucchelli 2019 ColSebastián BernalNo ratings yet
- Therapeutic Alternatives For Addressing Pink Esthetic Complications in Single-Tooth Implants: A Proposal For A Clinical Decision TreeDocument12 pagesTherapeutic Alternatives For Addressing Pink Esthetic Complications in Single-Tooth Implants: A Proposal For A Clinical Decision TreeFrancisco VargasNo ratings yet
- Correcting Severe Scissor Bite in An Adult: Case ReportDocument12 pagesCorrecting Severe Scissor Bite in An Adult: Case ReportLikhita ChNo ratings yet
- Conservative ManagementDocument4 pagesConservative ManagementFatima AliNo ratings yet
- Silva 2012Document6 pagesSilva 2012Rafał PokrowieckiNo ratings yet
- Orthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewDocument5 pagesOrthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewNatasha Ank100% (1)
- 7 OsteosarcomaDocument4 pages7 OsteosarcomaDodNo ratings yet
- Vetromilla 2014Document7 pagesVetromilla 2014r1comfupchNo ratings yet
- Odontoma: Case Series & Report of Cases Complicated by Infection and Multiple DenticlesDocument6 pagesOdontoma: Case Series & Report of Cases Complicated by Infection and Multiple DenticlesRamdaniar N. DianaNo ratings yet
- Berlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarDocument7 pagesBerlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarISAI FLORES PÉREZNo ratings yet
- Narrow-Diameter Implants Versus Regular-Diameter Implants For Rehabilitation of The Anterior Region: A Systematic Review and Meta-AnalysisDocument9 pagesNarrow-Diameter Implants Versus Regular-Diameter Implants For Rehabilitation of The Anterior Region: A Systematic Review and Meta-Analysiscarlos andres giraldoNo ratings yet
- Eej 48303 Case - Series MahalaxmiDocument8 pagesEej 48303 Case - Series MahalaxmiBurakNo ratings yet
- NakamuraDocument11 pagesNakamuraMairaMaraviChavezNo ratings yet
- Cephalometric Evaluation of Vertical Dimension of Occlusion in Varying MalocclusionsDocument6 pagesCephalometric Evaluation of Vertical Dimension of Occlusion in Varying MalocclusionsAnonymous 9PcFdakHcNo ratings yet
- Bopt PanizDocument9 pagesBopt PanizIvan CarreraNo ratings yet
- Three Dimensional Position of Impacted Maxillary Canines - Prevalence, Associated Pathology and Introduction To A New Classification SystemDocument7 pagesThree Dimensional Position of Impacted Maxillary Canines - Prevalence, Associated Pathology and Introduction To A New Classification SystemDalia Zamora GarciaNo ratings yet
- Guia Anterior - Gonzalez Hernandez-61-2Document12 pagesGuia Anterior - Gonzalez Hernandez-61-2Fred TorresNo ratings yet
- Article 1525485399Document4 pagesArticle 1525485399anisah fadilahNo ratings yet
- 10 1016@j Ijom 2020 09 025Document7 pages10 1016@j Ijom 2020 09 025Muhammad Azhar ImranNo ratings yet
- 1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2Document10 pages1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2waf51No ratings yet
- Osteo MaDocument4 pagesOsteo MaoptavianaNo ratings yet
- Emergency Management of Temporomandibular Joint Dislocation With Manual ReductionDocument5 pagesEmergency Management of Temporomandibular Joint Dislocation With Manual ReductionRisallah CintaNo ratings yet
- Santamaria MP. - Connective tissue graft plus resin-modified glass ionomer restoration for the treatment of gingival recession associated with non carious cervical lesion a randomized controlled clinical trialDocument8 pagesSantamaria MP. - Connective tissue graft plus resin-modified glass ionomer restoration for the treatment of gingival recession associated with non carious cervical lesion a randomized controlled clinical trialgabrielaNo ratings yet
- 6-Year-Follo Up. 3 Steps Techniques. Francesca Valati-1 PDFDocument25 pages6-Year-Follo Up. 3 Steps Techniques. Francesca Valati-1 PDFAdriana CoronadoNo ratings yet
- Laterally Closed Tunnel Sculean Allen IJPRD 2018 PDFDocument11 pagesLaterally Closed Tunnel Sculean Allen IJPRD 2018 PDFVladAlexandruSerseaNo ratings yet
- Implications of Periodontal Status in The Success of Different Types of Fixed Prosthetic ConstructionsDocument8 pagesImplications of Periodontal Status in The Success of Different Types of Fixed Prosthetic ConstructionsGhimpu DanielaNo ratings yet
- Dafpus 1Document8 pagesDafpus 1Winda WidhyastutiNo ratings yet
- Apiko 2Document7 pagesApiko 2Asri DamayantiNo ratings yet
- Complete Dentures: An Introduction: ProstheticsDocument68 pagesComplete Dentures: An Introduction: ProstheticsSahana RangarajanNo ratings yet
- His To LogieDocument5 pagesHis To Logiekhawla boukhNo ratings yet
- Gingival RecessionDocument23 pagesGingival RecessionRizki Yuli amandaNo ratings yet
- Restoration of Occlusal Plane and Esthetics in Severely Worn DentitionDocument4 pagesRestoration of Occlusal Plane and Esthetics in Severely Worn DentitionUJ CommunicationNo ratings yet
- Developing Class III MaloclussionsDocument18 pagesDeveloping Class III MaloclussionsJ.A.C.No ratings yet
- Ankylosis TMJDocument13 pagesAnkylosis TMJKrithika AcNo ratings yet
- V M A B D D I P AC R: Ertical Andibular Lveolar ONE Istraction and Ental Mplant Lacement: ASE EportDocument5 pagesV M A B D D I P AC R: Ertical Andibular Lveolar ONE Istraction and Ental Mplant Lacement: ASE EportDr. Jalisson VicenteNo ratings yet
- The Z-Plasty Technique On The Frenectomy ApproachDocument5 pagesThe Z-Plasty Technique On The Frenectomy ApproachVineet ArunNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
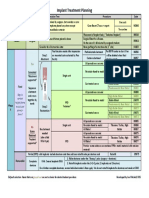
- Implant TX Plan GridDocument1 pageImplant TX Plan GridAhmed BadrNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- 1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureDocument4 pages1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureingronaldNo ratings yet
- Working OnDocument1 pageWorking OnAhmed BadrNo ratings yet
- Med Oncology MCQDocument109 pagesMed Oncology MCQdrzika100% (8)
- Original PDFDocument6 pagesOriginal PDFMamo AmmoNo ratings yet
- 6038ed9dcef5d IJAR-35170Document5 pages6038ed9dcef5d IJAR-35170Ahmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- Successful Intraoral Film RadiographyDocument10 pagesSuccessful Intraoral Film RadiographyAhmed BadrNo ratings yet
- Prognosis 2021Document10 pagesPrognosis 2021Ahmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- M Vista in Class 3Document12 pagesM Vista in Class 3Ahmed BadrNo ratings yet
- Vista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpDocument7 pagesVista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpAhmed BadrNo ratings yet
- MetaanalysisDocument12 pagesMetaanalysisAhmed BadrNo ratings yet
- Korkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeDocument10 pagesKorkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeAhmed BadrNo ratings yet
- AA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Document10 pagesAA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Ahmed BadrNo ratings yet
- Combinin Tunnel With Douple PapillaDocument12 pagesCombinin Tunnel With Douple PapillaAhmed BadrNo ratings yet
- 22 CE CreditsDocument11 pages22 CE CreditsAhmed BadrNo ratings yet
- Content ServerDocument10 pagesContent ServerAhmed BadrNo ratings yet
- 5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Document21 pages5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Ahmed BadrNo ratings yet
- Sticky BoneDocument7 pagesSticky BoneAhmed BadrNo ratings yet
- Guidelines For Immediate ImplanttDocument11 pagesGuidelines For Immediate ImplanttAhmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- 3A 2B Immediate ImplantDocument6 pages3A 2B Immediate ImplantAhmed BadrNo ratings yet
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocument5 pagesMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNo ratings yet
- 2010 Sofia Aroca SoteloDocument52 pages2010 Sofia Aroca SoteloAhmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- A Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureDocument11 pagesA Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureAhmed BadrNo ratings yet
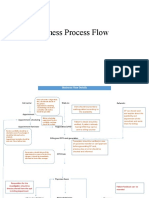
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Vyankatesh City-IIDocument17 pagesVyankatesh City-IIapi-27095887No ratings yet
- Michael Simonov CVDocument2 pagesMichael Simonov CVAnonymous QioCrCEVNo ratings yet
- Manual Handling DefinitionDocument2 pagesManual Handling DefinitionRaj KumarNo ratings yet
- CXC Csec English A June 2015 p1Document16 pagesCXC Csec English A June 2015 p1Rihanna Johnson100% (1)
- 02 2020 Tuaha Adil and Dr. Faisal JamilDocument39 pages02 2020 Tuaha Adil and Dr. Faisal JamilKhadijaNo ratings yet
- Second Circuit Public Charge RulingDocument110 pagesSecond Circuit Public Charge RulingLaw&CrimeNo ratings yet
- New Text DocumentDocument2 pagesNew Text DocumenteqweNo ratings yet
- Jonsen 4 Box MethodDocument5 pagesJonsen 4 Box MethodsawsanNo ratings yet
- Ims 1 10 18Document2 pagesIms 1 10 18Katherine UrregoNo ratings yet
- I-Stat 1 Quick Reference Guide 716942-00l CompressedDocument7 pagesI-Stat 1 Quick Reference Guide 716942-00l Compressedنجلاء الطلحيNo ratings yet
- Job Safety Analysis: Abqaiq Plants OperationDocument5 pagesJob Safety Analysis: Abqaiq Plants OperationZia ur RehmanNo ratings yet
- Rickets - A Brief View With Homoeopathic ApproachDocument32 pagesRickets - A Brief View With Homoeopathic ApproachDr. Sandeep Anwane100% (1)
- 28 CryptorchidismDocument23 pages28 CryptorchidismFaisal Ibn MushtaqNo ratings yet
- Complete Holistic Guide To Working Out in The GymDocument218 pagesComplete Holistic Guide To Working Out in The Gympsichi21No ratings yet
- Policy That Implemented in Kota SamarahanDocument9 pagesPolicy That Implemented in Kota SamarahanIskandar IskandarNo ratings yet
- Power2 340-H44: Operation ManualDocument166 pagesPower2 340-H44: Operation ManualDmitrii PustoshkinNo ratings yet
- KP Astrology Rules of PredictionDocument4 pagesKP Astrology Rules of PredictionRajeshNo ratings yet
- AAFP Board Review ClinchersDocument53 pagesAAFP Board Review ClinchersJessica E Isom100% (2)
- Nursing Care Plan For Patients With FractureDocument3 pagesNursing Care Plan For Patients With Fracture_cezca_89% (168)
- Pengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseDocument9 pagesPengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseTjatur SurantullohNo ratings yet
- Readers Digest Asia Feburary 2021Document134 pagesReaders Digest Asia Feburary 2021FURY FURIONNo ratings yet
- Indian Research Funding AgenciesDocument6 pagesIndian Research Funding AgencieskcchtphdNo ratings yet
- YMCA Program Guide - 2016Document44 pagesYMCA Program Guide - 2016Pickens County YMCANo ratings yet
- Assessment of PersonalityDocument3 pagesAssessment of PersonalityRahman ButtNo ratings yet
- Research Proposal-1Document28 pagesResearch Proposal-1sowsthikaNo ratings yet
- JUVENILE Justice ProjectDocument24 pagesJUVENILE Justice ProjectyashaNo ratings yet
- Valid RRR Application 2013 - 2017 PDFDocument22,467 pagesValid RRR Application 2013 - 2017 PDFAyub NaveedNo ratings yet
- Chevron Thailand Employee and Contractor Handbook EngDocument200 pagesChevron Thailand Employee and Contractor Handbook EngAndré Lima100% (1)
- Prevalence of High Risk Pregnancy in Rural DharwadDocument4 pagesPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNo ratings yet