You might also like
- Histological Examination of The Effect of Concentrated Growth Factor (CGF) On Healing Outcomes After Maxillary Sinus Floor Augmentation SurgeryDocument10 pagesHistological Examination of The Effect of Concentrated Growth Factor (CGF) On Healing Outcomes After Maxillary Sinus Floor Augmentation SurgeryAnthony LiNo ratings yet
- s12903 019 0849 7Document8 pagess12903 019 0849 7Gloria SequeiraNo ratings yet
- 7-Paulo M. Camargo 2009Document9 pages7-Paulo M. Camargo 2009Ashish DambhareNo ratings yet
- Perio Article For PublishingDocument7 pagesPerio Article For PublishingSAGI RATHNA PRASAD me14d210No ratings yet
- 4-Vojislav Lekovic 2002Document8 pages4-Vojislav Lekovic 2002Ashish DambhareNo ratings yet
- Xenogeneic Collagen Matrix vs. Connective Tissue Graft For The Treatment of Multiple Gingival Recession: A Systematic Review and Meta AnalysisDocument24 pagesXenogeneic Collagen Matrix vs. Connective Tissue Graft For The Treatment of Multiple Gingival Recession: A Systematic Review and Meta AnalysisDANTE DELEGUERYNo ratings yet
- Fathiazar 2022 1-3-6mDocument8 pagesFathiazar 2022 1-3-6mMARIA ANTONIETA RODRIGUEZ GALECIONo ratings yet
- Use of Platelet-Rich Fibrin Membrane Following Treatment of Gingival Recession: A Randomized Clinical TrialDocument4 pagesUse of Platelet-Rich Fibrin Membrane Following Treatment of Gingival Recession: A Randomized Clinical TrialAurora Hadijah GodfriedNo ratings yet
- Suzuki K 2020. 3-6 MesesDocument11 pagesSuzuki K 2020. 3-6 MesesMARIA ANTONIETA RODRIGUEZ GALECIONo ratings yet
- 1 ST JC PDF - SindhuDocument32 pages1 ST JC PDF - SindhuDadi SindhuNo ratings yet
- Platelet Rich Plasma in Reconstructive Periodontal Therapy: Selcuk Yılmaz, Gokser Cakar and Sebnem Dirikan IpciDocument23 pagesPlatelet Rich Plasma in Reconstructive Periodontal Therapy: Selcuk Yılmaz, Gokser Cakar and Sebnem Dirikan Ipciade ismailNo ratings yet
- Rotenberg 2014Document6 pagesRotenberg 2014Kyoko CPNo ratings yet
- A Comprehensive Review of Concentrated Growth Factors and Their Novel Applications in Facial Reconstructive and Regenerative MedicineDocument11 pagesA Comprehensive Review of Concentrated Growth Factors and Their Novel Applications in Facial Reconstructive and Regenerative MedicineHiktor TomNo ratings yet
- Platelet Rich FibrinDocument7 pagesPlatelet Rich FibrinNelly AndriescuNo ratings yet
- Jcpe 13086Document10 pagesJcpe 13086jcNo ratings yet
- Comparing Osteogenic Effects Between Concentrated Growth Factors and The Acellular Dermal MatrixDocument5 pagesComparing Osteogenic Effects Between Concentrated Growth Factors and The Acellular Dermal MatrixHiktor TomNo ratings yet
- In Vitro Investigation of Gelatin/Polycaprolactone Nano Bers in Modulating Human Gingival Mesenchymal Stromal CellsDocument15 pagesIn Vitro Investigation of Gelatin/Polycaprolactone Nano Bers in Modulating Human Gingival Mesenchymal Stromal CellsZhongqi ZhaoNo ratings yet
- Role of CGF (Concentrated Growth Factor) in Periodontal RegenerationDocument3 pagesRole of CGF (Concentrated Growth Factor) in Periodontal RegenerationArmareality ArmarealityNo ratings yet
- Clinical StudyDocument11 pagesClinical StudyandreeaNo ratings yet
- Clinical Outcome of Periodontal Regenerative Therapy Using Collagen Membrane and Deproteinized Bovine Bone Mineral: A 2.5-Year Follow-Up StudyDocument8 pagesClinical Outcome of Periodontal Regenerative Therapy Using Collagen Membrane and Deproteinized Bovine Bone Mineral: A 2.5-Year Follow-Up Studyzakia velasufaNo ratings yet
- Tissue Enginering 2Document97 pagesTissue Enginering 2วสวัตติ์ โตแสงชัยNo ratings yet
- 2015 Kin JIACD - Sticky Bone - Sohn Et Al PDFDocument20 pages2015 Kin JIACD - Sticky Bone - Sohn Et Al PDFOscar CabreraNo ratings yet
- Free Gingival Autograftand Subepithelial Connective Tissue Graftforthe Treatmentof Gingival Recession ABrief Reviewand Reportof Three CasesDocument9 pagesFree Gingival Autograftand Subepithelial Connective Tissue Graftforthe Treatmentof Gingival Recession ABrief Reviewand Reportof Three CasessutriNo ratings yet
- Peri-Implant Soft Tissue Phenotype Modification and Its Impact On Peri-Implant Health: A Systematic Review and Network Meta-AnalysisDocument24 pagesPeri-Implant Soft Tissue Phenotype Modification and Its Impact On Peri-Implant Health: A Systematic Review and Network Meta-AnalysisAazariNo ratings yet
- In Vitro and in Vivo Effects of Concentrated Growth Factor On CelDocument23 pagesIn Vitro and in Vivo Effects of Concentrated Growth Factor On CelalhomdiyahyaNo ratings yet
- Meza-Mauricio 2021. b-3-6Document12 pagesMeza-Mauricio 2021. b-3-6MARIA ANTONIETA RODRIGUEZ GALECIONo ratings yet
- PB11 4678 R2Document15 pagesPB11 4678 R2CAMILO ANDRÉS SABOGAL ARGUELLONo ratings yet
- 2019 Autogenous Soft Tissue Grafting For Periodontal and Peri-Implant Plastic Surgical ReconstructionDocument8 pages2019 Autogenous Soft Tissue Grafting For Periodontal and Peri-Implant Plastic Surgical Reconstructionayu calisthaNo ratings yet
- Case Series: Single-Flap Approach in Periodontal Regeneration For Intraosseous Defects: Case SeriesDocument6 pagesCase Series: Single-Flap Approach in Periodontal Regeneration For Intraosseous Defects: Case SeriesJoshua Diaz QuiquijanaNo ratings yet
- 5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Document21 pages5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Ahmed BadrNo ratings yet
- Journal Homepage: - : IntroductionDocument10 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Platelet Rich PlasmaDocument3 pagesPlatelet Rich PlasmaInternational Organization of Scientific Research (IOSR)100% (1)
- (2019) Pini Prato. EVOLUCIÓN TÉCNICAS MUCOGINGIVALDocument7 pages(2019) Pini Prato. EVOLUCIÓN TÉCNICAS MUCOGINGIVALDaniel EchegarayNo ratings yet
- Parvini Free Gingival 2020Document26 pagesParvini Free Gingival 2020SergioNo ratings yet
- Single Gingival Recession Associated With Non-Carious Cervical Lesion Treated by Partial RestorationDocument24 pagesSingle Gingival Recession Associated With Non-Carious Cervical Lesion Treated by Partial RestorationGabriela Lou GomezNo ratings yet
- Jop 2015 140376 PDFDocument4 pagesJop 2015 140376 PDFCynthia Ayumi Kamogawa MafraNo ratings yet
- Guided Bone Regeneration Simultaneous With Implant Placement Using Bovine-DerivedDocument13 pagesGuided Bone Regeneration Simultaneous With Implant Placement Using Bovine-DerivedCamilo Andrés Sabogal ArguelloNo ratings yet
- Injectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?Document9 pagesInjectable Platelet Rich Fibrin (i-PRF) : Opportunities in Regenerative Dentistry?Bruno MañonNo ratings yet
- Regenerative Potential of Cultured Gingival Fibroblasts - RCTDocument12 pagesRegenerative Potential of Cultured Gingival Fibroblasts - RCTDr.Niveditha SNo ratings yet
- Mukogingivalna Kurs 2014Document52 pagesMukogingivalna Kurs 2014Berin BunticNo ratings yet
- Lu 2019Document10 pagesLu 2019CAMILO ANDRÉS SABOGAL ARGUELLONo ratings yet
- In Vitro Biocompatibility of Biohybrid Polymers Membrane Evaluated in Human Gingival FibroblastsDocument9 pagesIn Vitro Biocompatibility of Biohybrid Polymers Membrane Evaluated in Human Gingival Fibroblasts赵忠琪No ratings yet
- Use of PRP, PRF and CGF in Periodontal Regeneration andDocument23 pagesUse of PRP, PRF and CGF in Periodontal Regeneration andmaria teresa pertuz rondonNo ratings yet
- Cth artikel Final Efficacy and Cost Analysis of a Fish Skin Graft vs Standard of Care in the Management of Chronic Diabetic Foot Ulcers: A Prospective, Multicenter, Randomized Controlled Clinical TrialDocument21 pagesCth artikel Final Efficacy and Cost Analysis of a Fish Skin Graft vs Standard of Care in the Management of Chronic Diabetic Foot Ulcers: A Prospective, Multicenter, Randomized Controlled Clinical TrialanabkddosenNo ratings yet
- JIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelDocument8 pagesJIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelLouis HutahaeanNo ratings yet
- Tecnica XenogenicaDocument9 pagesTecnica XenogenicaferNo ratings yet
- RetrieveDocument10 pagesRetrieveDANTE DELEGUERYNo ratings yet
- 00-Treatment of Periodontal Intrabony Defects Using Bovine Porous Bone Mineral and Guided Tissue Regeneration With:without Platelet-Rich FibrinDocument8 pages00-Treatment of Periodontal Intrabony Defects Using Bovine Porous Bone Mineral and Guided Tissue Regeneration With:without Platelet-Rich FibrinaemontoNo ratings yet
- Minimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported OutcomeDocument17 pagesMinimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported Outcomemahesh kumarNo ratings yet
- Frumuzache Oana PDFDocument8 pagesFrumuzache Oana PDFSergiuPotlogNo ratings yet
- J Clinic Periodontology - 2019 - Dai - Long Term Stability of Root Coverage Procedures For Single Gingival Recessions ADocument14 pagesJ Clinic Periodontology - 2019 - Dai - Long Term Stability of Root Coverage Procedures For Single Gingival Recessions ADr.Niveditha SNo ratings yet
- Management of Two-Wall Infra - Bony DefecDocument6 pagesManagement of Two-Wall Infra - Bony DefecbubuvulpeaNo ratings yet
- Liu 2021Document11 pagesLiu 2021jcNo ratings yet
- Cite Share Labial Strip Gingival Graft For The Reconstruction of Severely Distorted Mucogingival Defects - Urban 2020Document9 pagesCite Share Labial Strip Gingival Graft For The Reconstruction of Severely Distorted Mucogingival Defects - Urban 2020Claudio GuzmanNo ratings yet
- Root Coverage For Single Deep Gingival RecessionsDocument9 pagesRoot Coverage For Single Deep Gingival RecessionsMichal PerkowskiNo ratings yet
- Autogenous Soft Tissue Grafting For Periodontal and Peri-Implant Plastic Surgical ReconstructionDocument8 pagesAutogenous Soft Tissue Grafting For Periodontal and Peri-Implant Plastic Surgical ReconstructionjeeveshNo ratings yet
- Improved Growth Factor Delivery and Cellular Activity Using Concentrated Platelet-Rich Fibrin (C-PRF) When Compared With Traditional Injectable (i-PRF) ProtocolsDocument11 pagesImproved Growth Factor Delivery and Cellular Activity Using Concentrated Platelet-Rich Fibrin (C-PRF) When Compared With Traditional Injectable (i-PRF) Protocolsxiaoxin zhangNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- T Berridge2019Document8 pagesT Berridge2019Joshua Diaz QuiquijanaNo ratings yet
- Working OnDocument1 pageWorking OnAhmed BadrNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- Successful Intraoral Film RadiographyDocument10 pagesSuccessful Intraoral Film RadiographyAhmed BadrNo ratings yet
- Original PDFDocument6 pagesOriginal PDFMamo AmmoNo ratings yet
- 6038ed9dcef5d IJAR-35170Document5 pages6038ed9dcef5d IJAR-35170Ahmed BadrNo ratings yet
- Med Oncology MCQDocument109 pagesMed Oncology MCQdrzika100% (8)
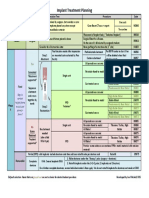
- Implant TX Plan GridDocument1 pageImplant TX Plan GridAhmed BadrNo ratings yet
- 1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureDocument4 pages1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureingronaldNo ratings yet
- Vista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpDocument7 pagesVista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpAhmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- Prognosis 2021Document10 pagesPrognosis 2021Ahmed BadrNo ratings yet
- Sticky BoneDocument7 pagesSticky BoneAhmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- MetaanalysisDocument12 pagesMetaanalysisAhmed BadrNo ratings yet
- M Vista in Class 3Document12 pagesM Vista in Class 3Ahmed BadrNo ratings yet
- Content ServerDocument10 pagesContent ServerAhmed BadrNo ratings yet
- Periodontal Plastic Surgery For The Management of Altered Passive EruptionDocument3 pagesPeriodontal Plastic Surgery For The Management of Altered Passive EruptionAhmed BadrNo ratings yet
- Guidelines For Immediate ImplanttDocument11 pagesGuidelines For Immediate ImplanttAhmed BadrNo ratings yet
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocument5 pagesMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNo ratings yet
- 5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Document21 pages5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Ahmed BadrNo ratings yet
- Combinin Tunnel With Douple PapillaDocument12 pagesCombinin Tunnel With Douple PapillaAhmed BadrNo ratings yet
- 22 CE CreditsDocument11 pages22 CE CreditsAhmed BadrNo ratings yet
- AA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Document10 pagesAA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Ahmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- A Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureDocument11 pagesA Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureAhmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- 3A 2B Immediate ImplantDocument6 pages3A 2B Immediate ImplantAhmed BadrNo ratings yet
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- 2010 Sofia Aroca SoteloDocument52 pages2010 Sofia Aroca SoteloAhmed BadrNo ratings yet
- Ims 1 10 18Document2 pagesIms 1 10 18Katherine UrregoNo ratings yet
- Tec. Qx. Russell Taylor HumeralDocument32 pagesTec. Qx. Russell Taylor HumeralAlvaro_086No ratings yet
- A Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFDocument5 pagesA Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFhahahapsuNo ratings yet
- Basics of Therapeutic DietsDocument12 pagesBasics of Therapeutic DietstiruchanurNo ratings yet
- Jhs Learner DataDocument3 pagesJhs Learner Dataapi-377500541No ratings yet
- Internship PresentationDocument23 pagesInternship Presentationapi-556937362No ratings yet
- Curriculum Vitae - Aditya Pratama PutraDocument3 pagesCurriculum Vitae - Aditya Pratama PutraIan SeptiantoNo ratings yet
- Prevalence of High Risk Pregnancy in Rural DharwadDocument4 pagesPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNo ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- Manual Handling DefinitionDocument2 pagesManual Handling DefinitionRaj KumarNo ratings yet
- Readers Digest Asia Feburary 2021Document134 pagesReaders Digest Asia Feburary 2021FURY FURIONNo ratings yet
- Nursing Care Plan For Patients With FractureDocument3 pagesNursing Care Plan For Patients With Fracture_cezca_89% (168)
- Xcelera Brochure Updated (English)Document24 pagesXcelera Brochure Updated (English)Pablo Rosas100% (1)
- Responsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFDocument64 pagesResponsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFPyae PyaeNo ratings yet
- Research Proposal-1Document28 pagesResearch Proposal-1sowsthikaNo ratings yet
- Winter Safety Toolbox TalkDocument18 pagesWinter Safety Toolbox TalkKristina100% (1)
- Data Legacy InsuranceCos SourceRSDocument48 pagesData Legacy InsuranceCos SourceRSrishu1527No ratings yet
- Assessment Diagnosis Outcomes Intervention Evaluation: Mabini Colleges, Inc. College of Nursing and MidwiferyDocument3 pagesAssessment Diagnosis Outcomes Intervention Evaluation: Mabini Colleges, Inc. College of Nursing and MidwiferyKathrina Mendoza HembradorNo ratings yet
- Developing Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersDocument6 pagesDeveloping Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersEugene GudimaNo ratings yet
- 48069B - Ferrofos 5260 (GB-ENG)Document6 pages48069B - Ferrofos 5260 (GB-ENG)danielNo ratings yet
- YMCA Program Guide - 2016Document44 pagesYMCA Program Guide - 2016Pickens County YMCANo ratings yet
- Hba1C: Quality System CertifiedDocument4 pagesHba1C: Quality System CertifiedNonameNo ratings yet
- RA 7164 Nursing Act of 1991Document8 pagesRA 7164 Nursing Act of 1991Filipino Nurses CentralNo ratings yet
- Stacey Wilson-Web V-Sept 2014Document6 pagesStacey Wilson-Web V-Sept 2014api-247917310No ratings yet
- HaloperidolDocument1 pageHaloperidolSalma AKNo ratings yet
- What Concentration Is The Best To Kill GermsDocument3 pagesWhat Concentration Is The Best To Kill GermsAncaja, Jameir 1CNo ratings yet
- PuppetryDocument183 pagesPuppetryÉva Hegedüsné50% (2)
- A Synopsis On: Consumer's Perception Towards Packaged Cold-Pressed Juices and Brand " PVT LTDDocument3 pagesA Synopsis On: Consumer's Perception Towards Packaged Cold-Pressed Juices and Brand " PVT LTDNationalinstituteDsnrNo ratings yet
- Presentations Day 1 - Session 1 - Presentation 06 - Sri LankaDocument29 pagesPresentations Day 1 - Session 1 - Presentation 06 - Sri LankaAnkur MishraNo ratings yet
- Family Systems Therapy and AddictionDocument30 pagesFamily Systems Therapy and AddictionthegavmanNo ratings yet