You might also like
- Dimensões Das PapilasDocument7 pagesDimensões Das PapilasAlin OdorNo ratings yet
- piniprato2000Document14 pagespiniprato2000YasuAAA AanzaiNo ratings yet
- Frumuzache Oana PDFDocument8 pagesFrumuzache Oana PDFSergiuPotlogNo ratings yet
- Flap Approaches in Plastic Periodontal and Implant Surgery: Critical Elements in Design and ExecutionDocument15 pagesFlap Approaches in Plastic Periodontal and Implant Surgery: Critical Elements in Design and Executionxiaoxin zhangNo ratings yet
- J 1600-051x 2012 01903 XDocument9 pagesJ 1600-051x 2012 01903 XDiyaa SakrNo ratings yet
- Tensao Do RetalhoDocument14 pagesTensao Do RetalhoAlin OdorNo ratings yet
- Coronally Advanced Flap With and Without VerticalDocument13 pagesCoronally Advanced Flap With and Without VerticalLEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- De Sanctis 2007 Coronally Advanced Flap A ModifiedDocument7 pagesDe Sanctis 2007 Coronally Advanced Flap A ModifiedSebastián BernalNo ratings yet
- Jcpe 12960Document9 pagesJcpe 12960Kyoko CPNo ratings yet
- Does The Dimension of The Graft Influence Patient Morbidity and Root Coverage Outcomes PDFDocument9 pagesDoes The Dimension of The Graft Influence Patient Morbidity and Root Coverage Outcomes PDFImplant DentNo ratings yet
- Cortellini MicroDocument11 pagesCortellini MicroDr. DeeptiNo ratings yet
- Jcpe 13246Document17 pagesJcpe 13246Dr. Pragyan SwainNo ratings yet
- 12 ParoDocument10 pages12 ParoDiana TanasaNo ratings yet
- 8 MC Guire ANDNunn Jop 2003Document16 pages8 MC Guire ANDNunn Jop 2003Mirela1612No ratings yet
- Ferrarotti Et Al. Journal of Clinical Periodontology (2018)Document10 pagesFerrarotti Et Al. Journal of Clinical Periodontology (2018)Jose Luis Bladco MorenoNo ratings yet
- Jper 20-0350 PDFDocument11 pagesJper 20-0350 PDFAnas KneifatiNo ratings yet
- Arocaetal - JCP 2013Document8 pagesArocaetal - JCP 2013Mauro Santiago EspinozaNo ratings yet
- Piezocorticision-Assisted Orthodontics: Efficiency, Safety, and Long-Term Evaluation of The Inflammatory ProcessDocument8 pagesPiezocorticision-Assisted Orthodontics: Efficiency, Safety, and Long-Term Evaluation of The Inflammatory ProcessrakshaNo ratings yet
- Minimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityDocument7 pagesMinimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityAnissa Citra UtamiNo ratings yet
- Decision Makin in Root Coverage Procedures For Esthetic OutcomesDocument11 pagesDecision Makin in Root Coverage Procedures For Esthetic OutcomesZelinschi Dragos ChristianNo ratings yet
- Meza-Mauricio 2021. b-3-6Document12 pagesMeza-Mauricio 2021. b-3-6MARIA ANTONIETA RODRIGUEZ GALECIONo ratings yet
- Pierpaolo Et Al-2012-Periodontology 2000Document27 pagesPierpaolo Et Al-2012-Periodontology 2000Dr. DeeptiNo ratings yet
- 2021 - Papilla Preservation Periodontal Surgery in Periodontal Reconstruction for Deep Combined Intra-suprabony Defects. Retrospective Analysis of a Registry-based CohortDocument7 pages2021 - Papilla Preservation Periodontal Surgery in Periodontal Reconstruction for Deep Combined Intra-suprabony Defects. Retrospective Analysis of a Registry-based CohortJontavius GilbertNo ratings yet
- 14Document8 pages14Maximiliano Jara ContrerasNo ratings yet
- Ahmed Beyli 2019Document6 pagesAhmed Beyli 2019Mounika KinjarapuNo ratings yet
- Zucchelli Desepitelizado 2010Document11 pagesZucchelli Desepitelizado 2010Maximiliano Jara ContrerasNo ratings yet
- Clinical Oral Implants Res - 2022 - Jung - Effect of Peri Implant Mucosal Thickness On Esthetic Outcomes and The EfficacyDocument9 pagesClinical Oral Implants Res - 2022 - Jung - Effect of Peri Implant Mucosal Thickness On Esthetic Outcomes and The EfficacyGustavo BerrioNo ratings yet
- Defectos de Furca y Regeneracion TisularDocument21 pagesDefectos de Furca y Regeneracion TisularSebastián BernalNo ratings yet
- Intramarrow PenetrationDocument20 pagesIntramarrow PenetrationsutriNo ratings yet
- Periodontology 2000 - 2003 - SANZ - Focus On Furcation Defects Guided Tissue RegenerationDocument21 pagesPeriodontology 2000 - 2003 - SANZ - Focus On Furcation Defects Guided Tissue Regenerationcarla lopezNo ratings yet
- Comparison of Infrabony Defects Treated With Enamel Matrix Derivative Versus Guided Tissue Regeneration With A Nonresorbable MembraneDocument8 pagesComparison of Infrabony Defects Treated With Enamel Matrix Derivative Versus Guided Tissue Regeneration With A Nonresorbable MembraneSartori & BovenziNo ratings yet
- Ijmse 2015 Vol 2 Issue 4 Page 154-166Document13 pagesIjmse 2015 Vol 2 Issue 4 Page 154-166Sarra TekayaNo ratings yet
- Efficacy of A Harvest Graft Substitute For Recession Coverage and Soft Tissue Volume Augmentation. A Randomized Controlled TrialDocument21 pagesEfficacy of A Harvest Graft Substitute For Recession Coverage and Soft Tissue Volume Augmentation. A Randomized Controlled TrialGabriela Lou GomezNo ratings yet
- Practical Applications: Decision Making in Gingival Recession Treatment: Scientific Evidence and Clinical ExperienceDocument12 pagesPractical Applications: Decision Making in Gingival Recession Treatment: Scientific Evidence and Clinical ExperienceAlexa LoyaNo ratings yet
- Santamaria MP. - Connective tissue graft plus resin-modified glass ionomer restoration for the treatment of gingival recession associated with non carious cervical lesion a randomized controlled clinical trialDocument8 pagesSantamaria MP. - Connective tissue graft plus resin-modified glass ionomer restoration for the treatment of gingival recession associated with non carious cervical lesion a randomized controlled clinical trialgabrielaNo ratings yet
- Clinical and Histological Evaluation ofDocument9 pagesClinical and Histological Evaluation ofJean Pierre Romero FebresNo ratings yet
- Australian Dental Journal: Graft Stabilization With Cyanoacrylate Decreases Shrinkage of Free Gingival GraftsDocument8 pagesAustralian Dental Journal: Graft Stabilization With Cyanoacrylate Decreases Shrinkage of Free Gingival GraftsVictor HernandezNo ratings yet
- Giovanpaolo Pini-Prato, Carlo Baldi, Roberto Rotundo, Debora Franceschi, Leonardo Muzzi. The Treatment of Gingival Recession Associated With Deep Corono-RadicularDocument11 pagesGiovanpaolo Pini-Prato, Carlo Baldi, Roberto Rotundo, Debora Franceschi, Leonardo Muzzi. The Treatment of Gingival Recession Associated With Deep Corono-RadicularJulio César PlataNo ratings yet
- Tavelli Et Al-2018-Journal of PeriodontologyDocument16 pagesTavelli Et Al-2018-Journal of PeriodontologyMartty BaNo ratings yet
- 190 Disc Repositioning Does It Really WorkDocument23 pages190 Disc Repositioning Does It Really WorkAngélica Valenzuela AndrighiNo ratings yet
- Medip, ISJ-5301 ODocument4 pagesMedip, ISJ-5301 OJesus EspinozaNo ratings yet
- J Clinic Periodontology - 2019 - Dai - Long Term Stability of Root Coverage Procedures For Single Gingival Recessions ADocument14 pagesJ Clinic Periodontology - 2019 - Dai - Long Term Stability of Root Coverage Procedures For Single Gingival Recessions ADr.Niveditha SNo ratings yet
- Aroca 2018Document16 pagesAroca 2018Mauro Santiago EspinozaNo ratings yet
- J Clinic Periodontology - 2021 - Jentsch - Flapless Application of Enamel Matrix Derivative in Periodontal Retreatment ADocument9 pagesJ Clinic Periodontology - 2021 - Jentsch - Flapless Application of Enamel Matrix Derivative in Periodontal Retreatment ATamara Pereira SanchezNo ratings yet
- CranioplastyDocument10 pagesCranioplastyMohab MohamedNo ratings yet
- Australian Dental JournalDocument7 pagesAustralian Dental JournalmanikantatssNo ratings yet
- Medición Tomográfica de La EncíaDocument8 pagesMedición Tomográfica de La EncíaOlga Vasquez SotoNo ratings yet
- Surgical Treatment of Peri-Implantitis: 3 - Year Results From A Randomized Controlled Clinical TrialDocument10 pagesSurgical Treatment of Peri-Implantitis: 3 - Year Results From A Randomized Controlled Clinical TrialFabian SanabriaNo ratings yet
- PALATALBANDAGEJPERIODocument12 pagesPALATALBANDAGEJPERIOAnonymous Y9FLG5kQdNo ratings yet
- Atm ArtDocument6 pagesAtm ArtYessyka EscalanteNo ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case Reportscarlos javier andraadeNo ratings yet
- Soft Tissue Phenotype Modifcation Impacts On Peri Implant Stability - A Comparative Cohort Study - HL Wang 2022Document12 pagesSoft Tissue Phenotype Modifcation Impacts On Peri Implant Stability - A Comparative Cohort Study - HL Wang 2022Claudio GuzmanNo ratings yet
- The Effectiveness of Immediate Triamcinolone Acetonide Injection After Auricular Keloid Surgery: A Prospective Randomized Controlled TrialDocument8 pagesThe Effectiveness of Immediate Triamcinolone Acetonide Injection After Auricular Keloid Surgery: A Prospective Randomized Controlled TrialMarande LisaNo ratings yet
- CLR 33 353Document9 pagesCLR 33 353Paul PalomequeNo ratings yet
- (2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKDocument13 pages(2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKBárbara Meza Lewis100% (1)
- Clinical Outcome of Non-Surgical Root Canal Treatment Using A Single-Cone Technique With Endosequence Bioceramic Sealer: A Retrospective AnalysisDocument5 pagesClinical Outcome of Non-Surgical Root Canal Treatment Using A Single-Cone Technique With Endosequence Bioceramic Sealer: A Retrospective AnalysisDani Jm TjNo ratings yet
- Journal ProstoDocument6 pagesJournal ProstoAvila Aita Harun RasyidNo ratings yet
- Single Gingival Recession Associated With Non-Carious Cervical Lesion Treated by Partial RestorationDocument24 pagesSingle Gingival Recession Associated With Non-Carious Cervical Lesion Treated by Partial RestorationGabriela Lou GomezNo ratings yet
- Advances in Periodontal Surgery: A Clinical Guide to Techniques and Interdisciplinary ApproachesFrom EverandAdvances in Periodontal Surgery: A Clinical Guide to Techniques and Interdisciplinary ApproachesSalvador NaresNo ratings yet
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceFrom EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceNo ratings yet
- Med Oncology MCQDocument109 pagesMed Oncology MCQdrzika100% (8)
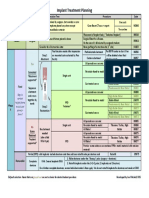
- Implant TX Plan GridDocument1 pageImplant TX Plan GridAhmed BadrNo ratings yet
- Working OnDocument1 pageWorking OnAhmed BadrNo ratings yet
- Successful Intraoral Film RadiographyDocument10 pagesSuccessful Intraoral Film RadiographyAhmed BadrNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- 6038ed9dcef5d IJAR-35170Document5 pages6038ed9dcef5d IJAR-35170Ahmed BadrNo ratings yet
- 1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureDocument4 pages1 Quarter 2 Quarter 3 Quarter 4 Quarter: Product Introduction Cost Reduction Introduction of New FeatureingronaldNo ratings yet
- Vista ct1)Document7 pagesVista ct1)Ahmed BadrNo ratings yet
- Original PDFDocument6 pagesOriginal PDFMamo AmmoNo ratings yet
- M Vista in Class 3Document12 pagesM Vista in Class 3Ahmed BadrNo ratings yet
- AA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Document10 pagesAA Imediate Impalnt With Provisionalization in Ethetic Zone Jop.2014.130632Ahmed BadrNo ratings yet
- MetaanalysisDocument12 pagesMetaanalysisAhmed BadrNo ratings yet
- Prognosis 2021Document10 pagesPrognosis 2021Ahmed BadrNo ratings yet
- Vista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpDocument7 pagesVista Technique and Platelet-Rich Fibrin Membrane For Treatment of Multiple Adjacent Gingival Recessions - 6 Month Follow-UpAhmed BadrNo ratings yet
- Combinin Tunnel With Douple PapillaDocument12 pagesCombinin Tunnel With Douple PapillaAhmed BadrNo ratings yet
- Korkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeDocument10 pagesKorkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeAhmed BadrNo ratings yet
- Guidelines For Immediate ImplanttDocument11 pagesGuidelines For Immediate ImplanttAhmed BadrNo ratings yet
- 22 CE CreditsDocument11 pages22 CE CreditsAhmed BadrNo ratings yet
- 5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Document21 pages5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Ahmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- Periodontal Plastic Surgery For The Management of Altered Passive EruptionDocument3 pagesPeriodontal Plastic Surgery For The Management of Altered Passive EruptionAhmed BadrNo ratings yet
- Sticky BoneDocument7 pagesSticky BoneAhmed BadrNo ratings yet
- 3A 2B Immediate ImplantDocument6 pages3A 2B Immediate ImplantAhmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- 2010 Sofia Aroca SoteloDocument52 pages2010 Sofia Aroca SoteloAhmed BadrNo ratings yet
- A Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureDocument11 pagesA Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureAhmed BadrNo ratings yet
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocument5 pagesMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNo ratings yet
- Healing Healthcare Through PhilosophyDocument23 pagesHealing Healthcare Through PhilosophyZlom ProfNo ratings yet
- NURS1027 Course Outline FALL 2010Document11 pagesNURS1027 Course Outline FALL 2010Lee KyoJeongNo ratings yet
- Toward Nanotechnology-Enabled Approaches Against The COVID-19 PandemicDocument24 pagesToward Nanotechnology-Enabled Approaches Against The COVID-19 Pandemicmadcraft9832No ratings yet
- Fungal Infections of The Skin: Dr. M. DissanayakeDocument52 pagesFungal Infections of The Skin: Dr. M. Dissanayakev_vijayakanth7656100% (1)
- SMEDA Private HospitalDocument23 pagesSMEDA Private Hospitalomerzafar100% (1)
- List of Master TemplatesDocument3 pagesList of Master TemplatesFlemingdonchcNo ratings yet
- Managing Anxiety and Pain in Ovarian CancerDocument5 pagesManaging Anxiety and Pain in Ovarian CancerDanica CumlatNo ratings yet
- 7051N3M126Q411U7Document69 pages7051N3M126Q411U7naldihasibuanNo ratings yet
- HS - I Don't Feel Weel TodayDocument10 pagesHS - I Don't Feel Weel Todaychie NbaNo ratings yet
- Parvo Treatment 101Document114 pagesParvo Treatment 101Mathilda JoanesNo ratings yet
- Invigilation Time Table 2022Document3 pagesInvigilation Time Table 2022ThomasNo ratings yet
- IGC 2 - Element 7 - Chemical HazardsDocument67 pagesIGC 2 - Element 7 - Chemical HazardsHim SiwakotiNo ratings yet
- HCIN 545 Project 2 Group C: - Haripriya Munagala - Anu Mathew - Jo Tzu LiuDocument19 pagesHCIN 545 Project 2 Group C: - Haripriya Munagala - Anu Mathew - Jo Tzu LiuDoris LiuNo ratings yet
- AOCase Control CohortstudydesignsDocument6 pagesAOCase Control CohortstudydesignsakshayajainaNo ratings yet
- Antibiotic Prophylaxis in Pediatric Odontology. An UpdateDocument6 pagesAntibiotic Prophylaxis in Pediatric Odontology. An UpdateJavier Farias VeraNo ratings yet
- Concept MapDocument9 pagesConcept Mapapi-608044542No ratings yet
- Types of shock surgery updatesDocument1 pageTypes of shock surgery updatesskNo ratings yet
- Hiv-Sle Case StudyDocument8 pagesHiv-Sle Case StudycathyNo ratings yet
- Literature Review On PCRDocument6 pagesLiterature Review On PCRafdtzfutn100% (1)
- Clinical Guidelines in Primary Care 3rdDocument12 pagesClinical Guidelines in Primary Care 3rdmimi100% (1)
- Korean Hand Acupuncture: A Unique and Highly Efficacious Branch of OMDocument4 pagesKorean Hand Acupuncture: A Unique and Highly Efficacious Branch of OMElanghovan ArumugamNo ratings yet
- cs3 Protocol-V2.5Document8 pagescs3 Protocol-V2.5CheferishNo ratings yet
- Aap 2009Document538 pagesAap 2009toniassaf100% (1)
- Division Memorandum: Examination of Deped Employees (Teaching and Non-Teaching Personnel) and inDocument3 pagesDivision Memorandum: Examination of Deped Employees (Teaching and Non-Teaching Personnel) and inJiwon KimNo ratings yet
- The Evolution of Professional NursingDocument47 pagesThe Evolution of Professional NursingkrizaricaNo ratings yet
- FLEP ScoreDocument6 pagesFLEP ScoreSaravanan SuthanthiranathanNo ratings yet
- Pediatrics 8 1202Document5 pagesPediatrics 8 1202ahmed yahyaNo ratings yet
- Zuku Visual Flashnotes GDV CondensedDocument1 pageZuku Visual Flashnotes GDV CondensedShubham HarishNo ratings yet
- Manav Rachna International School: ScheduleDocument3 pagesManav Rachna International School: SchedulesachinNo ratings yet
- Assignment 5.1 OHS Legislation - DiazDocument3 pagesAssignment 5.1 OHS Legislation - DiazADRIAN GABRIEL DIAZNo ratings yet