You might also like
- 1-Comprehensive Silver Full Body Checkup - PO3444322131-391Document21 pages1-Comprehensive Silver Full Body Checkup - PO3444322131-391xiaomi giaNo ratings yet
- 1-Gym Male Package - PO3183398202-954Document12 pages1-Gym Male Package - PO3183398202-954Divya KNo ratings yet
- Kidney FunctionDocument19 pagesKidney FunctionFarooq Bin MahfoozNo ratings yet
- PMC DSR 2017-18 For Rehabilitation of BridgeDocument5 pagesPMC DSR 2017-18 For Rehabilitation of BridgeDHRUV PuneNo ratings yet
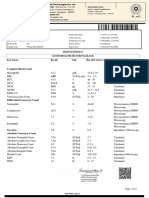
- Haematology Test Name Result Unit Bio. Ref. Range MethodDocument28 pagesHaematology Test Name Result Unit Bio. Ref. Range MethodVijaya SheelamNo ratings yet
- 1-Glucose - Postprandial - PO2611259108-802Document16 pages1-Glucose - Postprandial - PO2611259108-802Meet PatelNo ratings yet
- 1-Fever Package Extensive - PO2346586276-204Document9 pages1-Fever Package Extensive - PO2346586276-204Ishant ChaudharyNo ratings yet
- 1-Comprehensive Full Body Checkup - PO3310643047-461Document19 pages1-Comprehensive Full Body Checkup - PO3310643047-461newskishore100% (1)
- Falaan ReportDocument4 pagesFalaan ReportAzeem ChauhanNo ratings yet
- 1-Good Health Premium Package - PO1065281239-651Document19 pages1-Good Health Premium Package - PO1065281239-651Renu ChoudharyNo ratings yet
- Report 3f90266bDocument18 pagesReport 3f90266bSK TacNo ratings yet
- CTM400 JD 6090 Engine Service Manual PDFDocument420 pagesCTM400 JD 6090 Engine Service Manual PDFDaniel Ostapovich100% (6)
- Laboratory Investigation Report: Kindly Correlate With Clinical FindingsDocument3 pagesLaboratory Investigation Report: Kindly Correlate With Clinical FindingsNaveen 1802406No ratings yet
- Report 6737931eDocument19 pagesReport 6737931eNeevinternational NeevNo ratings yet
- Concrete Masonry - Free Standing WallsDocument42 pagesConcrete Masonry - Free Standing WallsDaniel Liew100% (7)
- Date 15/feb/2024 12:05PM 31/jul/23 11:10AM Unit Bio Ref IntervalDocument4 pagesDate 15/feb/2024 12:05PM 31/jul/23 11:10AM Unit Bio Ref IntervalrajorajisunnyNo ratings yet
- 1-Senior Citizen Advanced Package - PO3427386675-856Document18 pages1-Senior Citizen Advanced Package - PO3427386675-856Ravi PrakashNo ratings yet
- Dhrivesh: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval MethodDocument18 pagesDhrivesh: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval MethodDhruvesh Shekhar100% (1)
- FOURTH Quarter - Module 1: Structure and Functions of The Digestive SystemDocument5 pagesFOURTH Quarter - Module 1: Structure and Functions of The Digestive SystemChristian jade Quijano100% (1)
- Haematology Test Name Result Unit Bio. Ref. Range MethodDocument3 pagesHaematology Test Name Result Unit Bio. Ref. Range MethodSaurabh Prakash DixitNo ratings yet
- Report 400d0061Document18 pagesReport 400d0061Santosh BhandarkarNo ratings yet
- 1-Dengue IgG & IgM - PO2709736085-377Document12 pages1-Dengue IgG & IgM - PO2709736085-377TV UNITNo ratings yet
- 1-Basic Health Screening (Includes 29 Tests) - PO2403760062-868Document5 pages1-Basic Health Screening (Includes 29 Tests) - PO2403760062-868SMILLING CLOUDNo ratings yet
- S Chidambaram: Haematology Good Health Package Test Name Result Unit Bio Ref - Interval MethodDocument11 pagesS Chidambaram: Haematology Good Health Package Test Name Result Unit Bio Ref - Interval MethodRamkumar SundaramNo ratings yet
- Date 28/mar/2023 09:29AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument10 pagesDate 28/mar/2023 09:29AM Unit Bio Ref Interval: Laboratory Investigation ReportbhailogofficiaNo ratings yet
- Date 03/aug/2023 07:32AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument12 pagesDate 03/aug/2023 07:32AM Unit Bio Ref Interval: Laboratory Investigation ReportRishabh GuptaNo ratings yet
- SAES-A-401 - Nov. 3, 2013 PDFDocument41 pagesSAES-A-401 - Nov. 3, 2013 PDFLainhatanhNo ratings yet
- Po4009507960 540Document15 pagesPo4009507960 540PRADEEP KUMARNo ratings yet
- 1-Good Health Silver Package PO1380261394-553Document15 pages1-Good Health Silver Package PO1380261394-553Pramod YadavNo ratings yet
- Report C6f5558eDocument6 pagesReport C6f5558eAnkita ShrivastavaNo ratings yet
- Good Health Package PDFDocument8 pagesGood Health Package PDFRatan Swami SrivastavaNo ratings yet
- Gulrez Ali: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval MethodDocument17 pagesGulrez Ali: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval MethodGulrez AliNo ratings yet
- Complete Blood CountDocument2 pagesComplete Blood CountKhushi KumariNo ratings yet
- Capability-Based DevelopmentDocument46 pagesCapability-Based DevelopmentEero HosiaisluomaNo ratings yet
- Connection ApplicationDocument35 pagesConnection ApplicationLeo KhkNo ratings yet
- Khaleel Ur Rahman: Haematology Fever PackageDocument5 pagesKhaleel Ur Rahman: Haematology Fever Packageaashi77No ratings yet
- 1-Complete Blood Count - PO1106326185-399Document8 pages1-Complete Blood Count - PO1106326185-399Arup KumarNo ratings yet
- Report 220719 195623Document11 pagesReport 220719 195623Abdullah AlviNo ratings yet
- Uti Malaria TyphoidDocument4 pagesUti Malaria TyphoidniketaNo ratings yet
- Green Infrastructure Case StudiesDocument76 pagesGreen Infrastructure Case StudiesAr Arunima RaneNo ratings yet
- La Consolacion University Philippines Catmon, City of Malolos, BulacanDocument12 pagesLa Consolacion University Philippines Catmon, City of Malolos, BulacanDhaveKiezerLagbasEsguerraNo ratings yet
- Test Name Result Biological Ref. Interval Method: EDTA Whole BloodDocument4 pagesTest Name Result Biological Ref. Interval Method: EDTA Whole BloodAngouliu PanmeiNo ratings yet
- PdfText - 2023-06-01T222329.740Document8 pagesPdfText - 2023-06-01T222329.740Rahul NemadeNo ratings yet
- Report 0bd39992Document8 pagesReport 0bd39992NEETFIXNo ratings yet
- Cyanide-Free SLSDocument5 pagesCyanide-Free SLSmrkazi361No ratings yet
- PHLB1400496733 PDFDocument15 pagesPHLB1400496733 PDFurmobilehacked123No ratings yet
- GOR2208631Document6 pagesGOR2208631SakshiNo ratings yet
- Test Name Result Biological Ref. Interval Method: EDTA Whole BloodDocument2 pagesTest Name Result Biological Ref. Interval Method: EDTA Whole BloodYogesh BansalNo ratings yet
- D Seshagiri Rao-08Nov2023-Health CheDocument7 pagesD Seshagiri Rao-08Nov2023-Health CheSUNSHINE DIAGNOSTICSNo ratings yet
- Narayan CH Dey-73Document2 pagesNarayan CH Dey-73Sanjoy DasNo ratings yet
- Lab Report NewDocument1 pageLab Report NewNaman DagarNo ratings yet
- Don't Know Love - 1004584Document14 pagesDon't Know Love - 1004584baapj39No ratings yet
- MS - PDF - Viewer - 777432810Document37 pagesMS - PDF - Viewer - 777432810yogi4478No ratings yet
- HeaderDocument4 pagesHeaderatul kumarNo ratings yet
- 1-Kidney Function Test - PO3921596584-773 - 230517 - 125229Document7 pages1-Kidney Function Test - PO3921596584-773 - 230517 - 125229Moksh GujjarNo ratings yet
- CholeDocument12 pagesCholeaquacrystal538No ratings yet
- Labreportnew - 2023-10-17T102750.286Document2 pagesLabreportnew - 2023-10-17T102750.286sidlab202No ratings yet
- 1-Glucose - Postprandial YOGESHDocument19 pages1-Glucose - Postprandial YOGESHMeet PatelNo ratings yet
- ThyagarajDocument1 pageThyagarajrbllaboratoryNo ratings yet
- Date 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument12 pagesDate 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportChauhanNo ratings yet
- Mrs. V.dhana LakshmiDocument1 pageMrs. V.dhana LakshmiAnonymous lSZ9JVNo ratings yet
- Date 17/mar/2024 02:39PM Unit Bio Ref Interval: Laboratory Investigation ReportDocument11 pagesDate 17/mar/2024 02:39PM Unit Bio Ref Interval: Laboratory Investigation Reportarunsharma6221No ratings yet
- MR JoshanramDocument4 pagesMR JoshanrammuthurajctNo ratings yet
- Rama ReportDocument15 pagesRama ReportAnkush NayyarNo ratings yet
- Date 23/apr/2023 12:20PM Unit Bio Ref Interval: Kindly Correlate With Clinical FindingsDocument14 pagesDate 23/apr/2023 12:20PM Unit Bio Ref Interval: Kindly Correlate With Clinical FindingsashiNo ratings yet
- Header-1Document5 pagesHeader-1Sanchit NigamNo ratings yet
- Molecular Tools for the Detection and Quantification of Toxigenic CyanobacteriaFrom EverandMolecular Tools for the Detection and Quantification of Toxigenic CyanobacteriaRainer KurmayerNo ratings yet
- E-Lock: Digital Signature SolutionsDocument4 pagesE-Lock: Digital Signature SolutionsSuchit KumarNo ratings yet
- SpritzerDocument152 pagesSpritzerSYARMILA BINTI HASHIMNo ratings yet
- BadmintonDocument3 pagesBadmintonPratikRoyNo ratings yet
- Gen 004 P1 ReviewerDocument6 pagesGen 004 P1 Reviewerfernandezmaekyla1330No ratings yet
- Revuto Token SaleDocument1 pageRevuto Token Salekiranmai27No ratings yet
- AgriRise April-June 2023Document68 pagesAgriRise April-June 2023Kishore TataNo ratings yet
- Husham Issa Al-SaleemDocument21 pagesHusham Issa Al-SaleemlmiitobnykhpvdwuzyNo ratings yet
- SB - 7 SB - 7 WithdrawalDocument1 pageSB - 7 SB - 7 Withdrawal07raghuram5879100% (1)
- A Watch by Peter Henlein in LondonDocument13 pagesA Watch by Peter Henlein in LondonbahchovanskiNo ratings yet
- 3Document24 pages3Iris Bustamante PájaroNo ratings yet
- Govt. Pilot High School Rawalakot AJK Pre-Board ExamDocument2 pagesGovt. Pilot High School Rawalakot AJK Pre-Board ExamAbdul qadeerNo ratings yet
- List of Medical Professionals-SPADocument8 pagesList of Medical Professionals-SPANoemí GuzmartNo ratings yet
- First-Order Partial DerivativesDocument4 pagesFirst-Order Partial DerivativesRochelle ParedesNo ratings yet
- BH2 0316 en en-US PDFDocument955 pagesBH2 0316 en en-US PDFВячеславГрузевскийNo ratings yet
- Auntie Annes Allergen Information 2023Document1 pageAuntie Annes Allergen Information 2023BHAVESHNo ratings yet
- Introduction To Surveying: Basics of TraversingDocument33 pagesIntroduction To Surveying: Basics of Traversingjaffna100% (1)
- GTP 19 Application FormDocument5 pagesGTP 19 Application FormGaluh Kusuma Kencana Putri0% (1)
- 5kW On Grid Solar System Price With Subsidy SchemeDocument2 pages5kW On Grid Solar System Price With Subsidy SchemeAruna ReddyNo ratings yet
- Shijo Resume OctDocument1 pageShijo Resume OctMs.cimnasunny MNo ratings yet
- PDF Cooling Towers Problems 1 A Cooling Tower Is Located On A Mountain Where DDDocument17 pagesPDF Cooling Towers Problems 1 A Cooling Tower Is Located On A Mountain Where DDhabboNo ratings yet
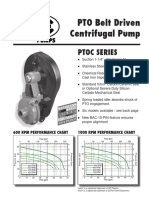
- Ptoc 03-13Document4 pagesPtoc 03-13Matias Contreras KöbrichNo ratings yet