You might also like
- Lyons Et Al-2017-Periodontology 2000Document4 pagesLyons Et Al-2017-Periodontology 2000Julio César PlataNo ratings yet
- Kanban COP - Lean Kanban Training PDFDocument14 pagesKanban COP - Lean Kanban Training PDFEdward Schaefer100% (1)
- PD2017 013 PDFDocument36 pagesPD2017 013 PDFChico Hermanu BrillianNo ratings yet
- Dental Implants Are Contraindicated In...Document5 pagesDental Implants Are Contraindicated In...Lia DietrichNo ratings yet
- 2022 - Implant Failure Rate and The Prevalence of Associated Risk FactorsDocument8 pages2022 - Implant Failure Rate and The Prevalence of Associated Risk FactorsVõHoàngThủyTiênNo ratings yet
- Risk Factors in Early Implant Failure: A Meta-AnalysisDocument9 pagesRisk Factors in Early Implant Failure: A Meta-AnalysisstortoNo ratings yet
- A Multifactorial Analysis To Identify Predictors of Implant Failure and Peri-Implant Bone LossDocument10 pagesA Multifactorial Analysis To Identify Predictors of Implant Failure and Peri-Implant Bone LossstortoNo ratings yet
- Dreyer - Et - Al-2018-J Periodon ResDocument25 pagesDreyer - Et - Al-2018-J Periodon ResAFKs GamerNo ratings yet
- Bone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewDocument12 pagesBone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewJarvin Miguel Buitrago GalindezNo ratings yet
- Survival of Dental Implants at Sites After Implant Failure: A Systematic ReviewDocument7 pagesSurvival of Dental Implants at Sites After Implant Failure: A Systematic ReviewNetra TaleleNo ratings yet
- Risk Factors in Bone Augmentation Procedures: Peter K. Moy - Tara AghalooDocument15 pagesRisk Factors in Bone Augmentation Procedures: Peter K. Moy - Tara Aghalooxiaoxin zhangNo ratings yet
- Risk Factors Associated With Early Implant Failure: A 5-Year Retrospective Clinical StudyDocument6 pagesRisk Factors Associated With Early Implant Failure: A 5-Year Retrospective Clinical StudystortoNo ratings yet
- Ramanauskaite 2016Document14 pagesRamanauskaite 2016Dr. Henner ValcarcelNo ratings yet
- 10 1111@jcpe 13362Document9 pages10 1111@jcpe 13362Dr.Niveditha SNo ratings yet
- Shetty Et Al. 2008Document10 pagesShetty Et Al. 2008EmmanuelRajapandianNo ratings yet
- Recommendations For Implant-Supported Full-Arch Rehabilitations in Edentulous Patients: The Oral Reconstruction Foundation Consensus ReportDocument13 pagesRecommendations For Implant-Supported Full-Arch Rehabilitations in Edentulous Patients: The Oral Reconstruction Foundation Consensus Reportsergio bernardesNo ratings yet
- Bilhan 2012Document7 pagesBilhan 2012laur112233No ratings yet
- Preface: Oral Maxillofacial Surg Clin N Am 19 (2007) XiDocument139 pagesPreface: Oral Maxillofacial Surg Clin N Am 19 (2007) XiZainab SalmanNo ratings yet
- Periodontally Compromised vs. Periodontally Healthy Patients and Dental Implants: A Systematic Review and Meta-AnalysisDocument19 pagesPeriodontally Compromised vs. Periodontally Healthy Patients and Dental Implants: A Systematic Review and Meta-AnalysisLuis Fernando RodriguesNo ratings yet
- Impacted Central Incisors Factors Affecting Prognosis and Treatment Duration 2015 American Journal of Orthodontics and Dentofacial OrthopedicsDocument8 pagesImpacted Central Incisors Factors Affecting Prognosis and Treatment Duration 2015 American Journal of Orthodontics and Dentofacial OrthopedicskjunaidNo ratings yet
- Necessity Factors and Predictors of Dental Crowding TreatmentDocument7 pagesNecessity Factors and Predictors of Dental Crowding TreatmentLuciaTrinovenaLaseNo ratings yet
- Wang 2015Document9 pagesWang 2015barbara buhlerNo ratings yet
- Ortodontia e Lesões Não CariosasDocument7 pagesOrtodontia e Lesões Não CariosasEliane dos santos rodriguesNo ratings yet
- Clinical Oral Implants Res - 2015 - Sousa - A Systematic Review of Implant Outcomes in Treated Periodontitis PatientsDocument58 pagesClinical Oral Implants Res - 2015 - Sousa - A Systematic Review of Implant Outcomes in Treated Periodontitis Patientskokorafat636No ratings yet
- Role of Thin Gingival Phenotype and Inadequate Keratinized Mucosa Width ( - 2 MM) As Risk Indicators For Peri Implantitis and Peri Implant MucositisDocument10 pagesRole of Thin Gingival Phenotype and Inadequate Keratinized Mucosa Width ( - 2 MM) As Risk Indicators For Peri Implantitis and Peri Implant MucositisAdil KaukabNo ratings yet
- 2019 Zhang - A Study On The Prevalence of Dental Anxiety Pain Perception and TheirDocument8 pages2019 Zhang - A Study On The Prevalence of Dental Anxiety Pain Perception and Theirfabian.balazs.93No ratings yet
- Ne 3Document8 pagesNe 3Zaid DewachiNo ratings yet
- Removable Prosthodontics: Denture AdhesivesDocument2 pagesRemovable Prosthodontics: Denture AdhesivespaulinaNo ratings yet
- Bruxism and Dental Implants - A Meta-AnalysisDocument12 pagesBruxism and Dental Implants - A Meta-AnalysisKenigal14No ratings yet
- Altered Expectations On Dental Implant Therapy Views of Patients Referred For Treatment of Peri-ImplantitisDocument6 pagesAltered Expectations On Dental Implant Therapy Views of Patients Referred For Treatment of Peri-ImplantitisSantiago Durango HurtadoNo ratings yet
- Jap 4 109Document7 pagesJap 4 109Buzatu IonelNo ratings yet
- 1 R Cambios OSEOS POSEXTRACCIONDocument16 pages1 R Cambios OSEOS POSEXTRACCIONfeli.riam24No ratings yet
- Daubert Et Al-2015-Journal of PeriodontologyDocument11 pagesDaubert Et Al-2015-Journal of PeriodontologyMUNAZNo ratings yet
- Alsaadi2007 Factores SistemicosDocument8 pagesAlsaadi2007 Factores SistemicosTorres MauricioNo ratings yet
- Is Dental Treatment of An Infected Tooth A Risk Factor For Locally Invasive Spread of InfectionDocument8 pagesIs Dental Treatment of An Infected Tooth A Risk Factor For Locally Invasive Spread of InfectionCarlos R. ValladaresNo ratings yet
- Laser en OrtodonciaDocument7 pagesLaser en OrtodonciaDiana ElíasNo ratings yet
- Is There An Association Between The Use of Antidepressants and Complications Involving Dental Implantes - A Systematic Review and Meta-AnalysisDocument8 pagesIs There An Association Between The Use of Antidepressants and Complications Involving Dental Implantes - A Systematic Review and Meta-AnalysisCaio GonçalvesNo ratings yet
- 1 s2.0 S030057121830037X MainDocument6 pages1 s2.0 S030057121830037X MainusrazvanNo ratings yet
- Bornstein, M. M., Cionca, N., & Mombelli, A. (2009)Document17 pagesBornstein, M. M., Cionca, N., & Mombelli, A. (2009)tefaNo ratings yet
- Oral and Dental Alterations and Growth Disruption Following Chemotherapy in Long-Term Survivors of Childhood MalignanciesDocument9 pagesOral and Dental Alterations and Growth Disruption Following Chemotherapy in Long-Term Survivors of Childhood MalignanciesGeorgia.annaNo ratings yet
- Scs 0b013e31826b8267Document5 pagesScs 0b013e31826b8267ANGELA ROMERONo ratings yet
- Shih 2016Document6 pagesShih 2016fatimahNo ratings yet
- Chen 2019Document9 pagesChen 2019Tiara HapkaNo ratings yet
- 10.1016@j.ajodo.2020.01.004 White Spot Lesion AlignerDocument8 pages10.1016@j.ajodo.2020.01.004 White Spot Lesion AlignerLima JúniorNo ratings yet
- Afraccion PDFDocument9 pagesAfraccion PDFzayraNo ratings yet
- Prevalence of Denture Stomatitis Among Complete Denture Wearers in AljoufDocument6 pagesPrevalence of Denture Stomatitis Among Complete Denture Wearers in AljoufnivehthaaNo ratings yet
- Effectiveness of Interceptive Orthodontic Treatment in Reducing MalocclusionsDocument8 pagesEffectiveness of Interceptive Orthodontic Treatment in Reducing MalocclusionsAriana de LeonNo ratings yet
- Dentistry 12 00083Document13 pagesDentistry 12 00083adiNo ratings yet
- Soft Tissue Augmentation Procedures For Mucogingival Defects in Esthetic SitesDocument31 pagesSoft Tissue Augmentation Procedures For Mucogingival Defects in Esthetic Sitesilich sevillaNo ratings yet
- ONMD2110Document9 pagesONMD2110Laura OchoaNo ratings yet
- Thematic Abstract Review: Systemic Factors Affecting Implant Survival?Document3 pagesThematic Abstract Review: Systemic Factors Affecting Implant Survival?Natalia Camila Rodríguez LatorreNo ratings yet
- GOBBATODocument11 pagesGOBBATOBianca MarcheziNo ratings yet
- IJOMI 2015 Thematic Extract - C I RatioDocument3 pagesIJOMI 2015 Thematic Extract - C I RatioZhiyi LinNo ratings yet
- Tooth-Implant Supported RemovableDocument29 pagesTooth-Implant Supported RemovabletaniaNo ratings yet
- Onam 2022Document24 pagesOnam 2022Elvia Maria Rios BeltranNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptsulistiyaNo ratings yet
- MID 2 SJ - bdj.2012.1008Document5 pagesMID 2 SJ - bdj.2012.1008Green SleevesNo ratings yet
- Magneticfields PDFDocument5 pagesMagneticfields PDFSergio Di VitantonioNo ratings yet
- Cre2 10Document15 pagesCre2 10jhonatan gaspariNo ratings yet
- Implant Failures-Diagnosis and ManagementDocument10 pagesImplant Failures-Diagnosis and ManagementDr Tarak ChavadaNo ratings yet
- Weltman Et Al., 2010 PDFDocument15 pagesWeltman Et Al., 2010 PDFplayer osamaNo ratings yet
- A Short Guide For Feature Engineering and Feature SelectionDocument32 pagesA Short Guide For Feature Engineering and Feature SelectionjainnitkNo ratings yet
- Kerala University PHD Course Work Exam SyllabusDocument4 pagesKerala University PHD Course Work Exam Syllabuslozuzimobow3100% (2)
- Magic Porridge Pot-story+BilderDocument4 pagesMagic Porridge Pot-story+BilderSylvester PhilipNo ratings yet
- Extended AbstractDocument4 pagesExtended Abstractadi_6294No ratings yet
- Fforde Economic StrategyDocument29 pagesFforde Economic StrategyDinhThuyNo ratings yet
- B2 Unit 4 Reading Plus LessonDocument2 pagesB2 Unit 4 Reading Plus LessonIruneNo ratings yet
- Business Law Syllabus (BLT)Document4 pagesBusiness Law Syllabus (BLT)Glene NallaNo ratings yet
- The Contemporary World Lesson 2Document32 pagesThe Contemporary World Lesson 2WENDELL VERGARANo ratings yet
- 850 SQ MM AAC Conductor PDFDocument1 page850 SQ MM AAC Conductor PDFSamyak DeoraNo ratings yet
- CW-80 ManualDocument12 pagesCW-80 ManualBrian YostNo ratings yet
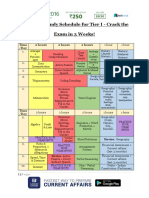
- SSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Document3 pagesSSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Tushita80% (15)
- Occlusal Considerations in Implant Therapy Clinical Guidelines With Biomechanical Rationale PDFDocument10 pagesOcclusal Considerations in Implant Therapy Clinical Guidelines With Biomechanical Rationale PDFSoares MirandaNo ratings yet
- A Brief History of DerivativesDocument12 pagesA Brief History of DerivativesPranab SahooNo ratings yet
- Humanities SculptureDocument15 pagesHumanities SculpturehungrynomadphNo ratings yet
- CH 1 Cases - Mcqs CH 1 Cases - McqsDocument55 pagesCH 1 Cases - Mcqs CH 1 Cases - McqsChaudhary AdeelNo ratings yet
- Understanding: Sexual HarassmentDocument8 pagesUnderstanding: Sexual HarassmentAlex TwahirwaNo ratings yet
- Cae Grammar TensesDocument4 pagesCae Grammar TensesYana MarinkovaNo ratings yet
- PPP Projects at A Glance. Madhya PradeshDocument7 pagesPPP Projects at A Glance. Madhya PradeshPPPnewsNo ratings yet
- Background: The Islamic World of Academy of ScienceDocument5 pagesBackground: The Islamic World of Academy of ScienceNusrat MaqboolNo ratings yet
- Bernardo Carpio - Mark Bryan NatontonDocument18 pagesBernardo Carpio - Mark Bryan NatontonMark Bryan NatontonNo ratings yet
- Anatomy and Physiology Outline PDFDocument2 pagesAnatomy and Physiology Outline PDFHampson MalekanoNo ratings yet
- Yr 10 2016 You Are What You Eat ProgDocument10 pagesYr 10 2016 You Are What You Eat Progapi-322152156No ratings yet
- Drugs: Samkox Productions 0774852021Document2 pagesDrugs: Samkox Productions 0774852021MichaelNo ratings yet
- Risk Management Framework at DCB BankDocument10 pagesRisk Management Framework at DCB BankRavi KumarNo ratings yet
- Welcome Olusegun Ajayi: Faqs Contact UsDocument3 pagesWelcome Olusegun Ajayi: Faqs Contact UsOlusegun AjayiNo ratings yet
- DM Plan Manda Upazila Noagaon District - English Version-2014Document104 pagesDM Plan Manda Upazila Noagaon District - English Version-2014CDMP BangladeshNo ratings yet
- Modernism Revisited Five Fascist ModernismDocument25 pagesModernism Revisited Five Fascist ModernismUdrea FanicaNo ratings yet
- Hammer Pulse TempDocument12 pagesHammer Pulse Temppeter911cm100% (1)