You might also like
- CLI Commands List For ZTE RoutetsDocument137 pagesCLI Commands List For ZTE RoutetsIrfan Ul Haq75% (4)
- SM-J701F-J7core PCBDocument2 pagesSM-J701F-J7core PCBSumit mobicare0% (1)
- Peace and LoveDocument3 pagesPeace and LoveÁlvaro Axel Ureta MendozaNo ratings yet
- 72 FullDocument3 pages72 FullLuisa BarbeitoNo ratings yet
- Townsville Daily Bulletin - February 12, 1949Document8 pagesTownsville Daily Bulletin - February 12, 1949Pablo AndresNo ratings yet
- Intro To Psychology - Course OutlineDocument6 pagesIntro To Psychology - Course Outlinesherica.brownNo ratings yet
- 6799 22119 1 PBDocument8 pages6799 22119 1 PBmeglaskaNo ratings yet
- Fault Codes 42-38LUVH26,34,50K-1535003386Document1 pageFault Codes 42-38LUVH26,34,50K-1535003386Firas Al-KanaaniNo ratings yet
- Makateeb e Sadrul Afazil by Zulfaqar Khan NaimiDocument251 pagesMakateeb e Sadrul Afazil by Zulfaqar Khan Naimisunnivoice100% (2)
- AS Chem RecapDocument10 pagesAS Chem RecapShumi TeeNo ratings yet
- Mazahib Ka Taqabuli Jayiza Asal PDFDocument58 pagesMazahib Ka Taqabuli Jayiza Asal PDFShaikhNo ratings yet
- Command Reference (Security)Document189 pagesCommand Reference (Security)MichaëlNo ratings yet
- ZXSDR BS8900 GU360 (Outdoor GSM&UMTS Dual Mode Macro Node B) System DescriptionDocument92 pagesZXSDR BS8900 GU360 (Outdoor GSM&UMTS Dual Mode Macro Node B) System DescriptionbbpncbNo ratings yet
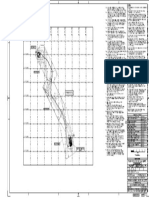
- Grid Map - Kurnool AirportDocument1 pageGrid Map - Kurnool AirportaeeNo ratings yet
- DIgSILENT RUM11 PDFDocument1 pageDIgSILENT RUM11 PDFFERDINADNo ratings yet
- CASE N Series TLB Ops ManualDocument318 pagesCASE N Series TLB Ops ManualDian Sikumbang100% (2)
- DTC Agreement Between Sweden and New ZealandDocument33 pagesDTC Agreement Between Sweden and New ZealandOECD: Organisation for Economic Co-operation and DevelopmentNo ratings yet
- Release NotesDocument17 pagesRelease NoteseelangovanNo ratings yet
- Plano 02Document1 pagePlano 02David RoyerNo ratings yet
- Combined Utility LayoutDocument1 pageCombined Utility LayoutShahul HameedNo ratings yet
- Ccna d2Document5 pagesCcna d2yottasNo ratings yet
- Data Manual: 3.3-V/5-V Dual Universal Asynchronous Receiver/TransmitterDocument61 pagesData Manual: 3.3-V/5-V Dual Universal Asynchronous Receiver/TransmitterSaba IdreesNo ratings yet
- User's Guide: eZ430-RF2500 Development ToolDocument24 pagesUser's Guide: eZ430-RF2500 Development Tooljtm1876No ratings yet
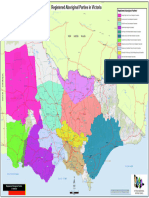
- Statewide Appointed RAPsDocument1 pageStatewide Appointed RAPsLachlan WRIGHTNo ratings yet
- SanitaryDocument1 pageSanitarysergio.anacletoNo ratings yet
- Layout Plan of Omaxe Metro City, Phase-1.: Proposed 50 Mt. Master Plan Green BeltDocument1 pageLayout Plan of Omaxe Metro City, Phase-1.: Proposed 50 Mt. Master Plan Green BeltSantosh Kori - freelancer wordpress joomla web designerNo ratings yet
- Igc 002 (GSR) Igc 001 (Gfu) : Sub 055 Pib 055 SDB 055Document1 pageIgc 002 (GSR) Igc 001 (Gfu) : Sub 055 Pib 055 SDB 055billNo ratings yet
- T843603001V0F1Document1 pageT843603001V0F1deva017No ratings yet
- MAR-IWM-019 - Rev 02 - Wall Setting Out GA A StatusDocument1 pageMAR-IWM-019 - Rev 02 - Wall Setting Out GA A StatusPetru LeontiNo ratings yet
- Performing Accurate PFM Mode Efficiency Measurements: Application ReportDocument7 pagesPerforming Accurate PFM Mode Efficiency Measurements: Application ReportRruga EdibresNo ratings yet
- Interfacing The MSOP8EVM To MSP430 Processors: Application ReportDocument5 pagesInterfacing The MSOP8EVM To MSP430 Processors: Application ReportosmanatamNo ratings yet
- Reference Guide: TMS320F2833x, 2823x Enhanced Controller Area Network (eCAN)Document82 pagesReference Guide: TMS320F2833x, 2823x Enhanced Controller Area Network (eCAN)nareshb_206No ratings yet
- Frankenstein: 4 Frankenstein Themes Lesson - Notebook March 29, 2011Document4 pagesFrankenstein: 4 Frankenstein Themes Lesson - Notebook March 29, 2011Rebecca MarescaNo ratings yet
- 422 To 420 ConversionDocument18 pages422 To 420 ConversionMarri RohitNo ratings yet
- Digital Isolator Design GuideDocument17 pagesDigital Isolator Design GuideYuvarajaNo ratings yet
- User'S Guide: Tms320Dm644X Dmsoc Vlynq PortDocument49 pagesUser'S Guide: Tms320Dm644X Dmsoc Vlynq PortawaismqsdNo ratings yet
- Design Methodology For MFB Filters in ADC Interface ApplicationsDocument32 pagesDesign Methodology For MFB Filters in ADC Interface ApplicationsKhalehNo ratings yet
- User's Guide: TMS320DM647/DM648 DSP Peripheral Component Interconnect (PCI)Document86 pagesUser's Guide: TMS320DM647/DM648 DSP Peripheral Component Interconnect (PCI)Alb GompNo ratings yet
- Controller Area Network Physical Layer Requirements: Application ReportDocument15 pagesController Area Network Physical Layer Requirements: Application Reportmail87523No ratings yet
- 4 Konfigurasi Bandara TaxiwayDocument31 pages4 Konfigurasi Bandara TaxiwayJoko BintoroNo ratings yet
- How To Use The VPBE and VPFE Driver On TMS320DM643x Devices: Application ReportDocument13 pagesHow To Use The VPBE and VPFE Driver On TMS320DM643x Devices: Application Reportganeshnikam22No ratings yet
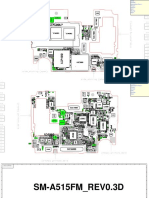
- SM-A515FM REV0.3D SCH PCBDocument12 pagesSM-A515FM REV0.3D SCH PCBiRem MasterNo ratings yet
- Combined (1) - RepairedDocument1 pageCombined (1) - RepairedHEDER GONZALES BENITESNo ratings yet
- Y en Triana La O Trombón 2666666Document1 pageY en Triana La O Trombón 2666666FeniXoN 12No ratings yet
- Ahmadi Finish Layout Hahc-Ah-1-Sh-Ar-00-01 27-12-2021-Hahc-Ah-1-Sh-Ar-00-01Document1 pageAhmadi Finish Layout Hahc-Ah-1-Sh-Ar-00-01 27-12-2021-Hahc-Ah-1-Sh-Ar-00-01NWA INT General Trading & ContractingNo ratings yet
- BGMC T042 B61 M&e SD CW 02Document1 pageBGMC T042 B61 M&e SD CW 02taufik rahimNo ratings yet
- BGMC T042 B61 M&e SD CW 04Document1 pageBGMC T042 B61 M&e SD CW 04taufik rahimNo ratings yet
- Getting Started Guide: Code Composer Studio Development Tools v3.3Document103 pagesGetting Started Guide: Code Composer Studio Development Tools v3.3David Chandy PesantezNo ratings yet
- DSP Control of Electro-Hydraulic Servo ActuatorsDocument26 pagesDSP Control of Electro-Hydraulic Servo ActuatorsJason KentNo ratings yet
- Booting DaVinci EVM From NAND FlashDocument14 pagesBooting DaVinci EVM From NAND FlashkechumasterNo ratings yet
- Technical Data Sheet For HILTI HIS N M16X170Document1 pageTechnical Data Sheet For HILTI HIS N M16X170Vadim TimoșcoNo ratings yet
- Test & CommissioningDocument3 pagesTest & CommissioningFim EventManagementNo ratings yet
- VH Ad 2 VHHH Aoc 3Document1 pageVH Ad 2 VHHH Aoc 3NmNo ratings yet
- L (63) 06 Layout1Document1 pageL (63) 06 Layout1Shreekant KeraiNo ratings yet
- L (63) 07 Layout1Document1 pageL (63) 07 Layout1Shreekant KeraiNo ratings yet
- L (63) 08 Layout1Document1 pageL (63) 08 Layout1Shreekant KeraiNo ratings yet
- 633559-M-E-D010-Stage 4 Pavilion-IFC SetDocument7 pages633559-M-E-D010-Stage 4 Pavilion-IFC SetNon Etabas GadnatamNo ratings yet
- Joka Soho+Master Plan-Model - SaptarshiDocument1 pageJoka Soho+Master Plan-Model - SaptarshiDiswag vlogNo ratings yet
- Case Selection For FPDDocument2 pagesCase Selection For FPDAmar BhochhibhoyaNo ratings yet
- Necrotizing Ulcerative GingivitisDocument24 pagesNecrotizing Ulcerative Gingivitissvk_chatterjeeNo ratings yet
- Brosencephalon's Internal MedicineDocument340 pagesBrosencephalon's Internal Medicinejtsk2100% (1)
- .Nursing Care Plan For Chronic Ill Patient2Document3 pages.Nursing Care Plan For Chronic Ill Patient2Anthonio MuenhoNo ratings yet
- Pharmaceutical Waste Management An Overview: Atul Kadam, Shitalkumar Patil, Sachin Patil, Anil TumkurDocument7 pagesPharmaceutical Waste Management An Overview: Atul Kadam, Shitalkumar Patil, Sachin Patil, Anil TumkurNafi Hasan ZahidNo ratings yet
- Project 5 Louise Nicole Yu - Resume 2019Document1 pageProject 5 Louise Nicole Yu - Resume 2019api-457735342No ratings yet
- LPLT12448 : LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Document6 pagesLPLT12448 : LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Kumar ManglamNo ratings yet
- Sample Lit Review WritingDocument9 pagesSample Lit Review WritingMarine LecomteNo ratings yet
- Behavioral Parent Training For ADHD Children A Mixed Methods StudyDocument6 pagesBehavioral Parent Training For ADHD Children A Mixed Methods Studyadinda puspita dewiNo ratings yet
- Physicians 10-2022Document38 pagesPhysicians 10-2022PRC BaguioNo ratings yet
- Gyne - Case 11 Lower Genital UTI PDFDocument2 pagesGyne - Case 11 Lower Genital UTI PDFcbac1990No ratings yet
- NHD Process PaperDocument3 pagesNHD Process Paperapi-491295292No ratings yet
- Approach To Abdominal PainDocument22 pagesApproach To Abdominal PainOmar AbdillahiNo ratings yet
- NCP FinalDocument5 pagesNCP FinalYoongiNo ratings yet
- Non ComplianceDocument29 pagesNon ComplianceFaraz Qurban Rajper100% (2)
- Dental HygieneDocument3 pagesDental Hygieneapi-507354264No ratings yet
- Texas Medical BoardDocument10 pagesTexas Medical Boardildefonso ortizNo ratings yet
- Management of Side Effects and Complication in Medical AbortionDocument10 pagesManagement of Side Effects and Complication in Medical AbortionmariaNo ratings yet
- Corticosteroids: Prof. Dr. Shah MuradDocument51 pagesCorticosteroids: Prof. Dr. Shah MuradnehascribdjoshiNo ratings yet
- Central Venous CatheterizationDocument71 pagesCentral Venous CatheterizationNobel LaureateNo ratings yet
- WMed Residency Match 2023Document3 pagesWMed Residency Match 2023WWMTNo ratings yet
- Prolonged LabourDocument36 pagesProlonged LabourQuay Kar Ying75% (4)
- 0527C BRIGHT IDEAS NUMBER 5 - Risk Assessment Tool - SB - V1Document1 page0527C BRIGHT IDEAS NUMBER 5 - Risk Assessment Tool - SB - V1sunrise755No ratings yet
- Digital Ischemic Compression Technique Aims at Evoking Temporary IschaemicDocument2 pagesDigital Ischemic Compression Technique Aims at Evoking Temporary IschaemicNAvi SinghNo ratings yet
- Dental HospitalDocument7 pagesDental HospitalNISHANTKUMAR PATELNo ratings yet
- Dysphagia As A Unique Presentation PostersDocument1 pageDysphagia As A Unique Presentation Postershadzrie imanNo ratings yet
- Whole-Body FDG PET Imaging in OncologyDocument305 pagesWhole-Body FDG PET Imaging in OncologyTurki100% (5)
- Week 5Document4 pagesWeek 5Ashley CastroNo ratings yet
- College of Nursing, Pharmacy and Allied Health SciencesDocument4 pagesCollege of Nursing, Pharmacy and Allied Health SciencesNiña AmatoNo ratings yet
- 2023 MayDocument33 pages2023 Maymemer XDNo ratings yet