You might also like
- Lung Cancer Report Sample High enDocument1 pageLung Cancer Report Sample High enBantiNo ratings yet
- Atlas Cancer CervicalDocument458 pagesAtlas Cancer CervicalihsansabridrNo ratings yet
- Cancer Patient's Guide To Overc - Derek HopkoDocument300 pagesCancer Patient's Guide To Overc - Derek HopkoGermán Edgardo MenevichianNo ratings yet
- 2014 WHO Classification of Tumours of The Female Reproductive Organs 2014 PDFDocument309 pages2014 WHO Classification of Tumours of The Female Reproductive Organs 2014 PDFPatología Pemex SurNo ratings yet
- Referensi Paper No 63Document9 pagesReferensi Paper No 63Kevin AnggaraNo ratings yet
- Health Risks From Exposure To Low Levels of Ionizing Radiation, Report in BriefDocument4 pagesHealth Risks From Exposure To Low Levels of Ionizing Radiation, Report in BriefNational Academies of Science, Engineering, and MedicineNo ratings yet
- Hricak 2021Document37 pagesHricak 2021Xiomara CelyNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptGeorge UngureanuNo ratings yet
- BJR 20210389Document10 pagesBJR 20210389Camilo SotomayorNo ratings yet
- Subjective Perception of Radiation RiskDocument8 pagesSubjective Perception of Radiation RiskD. IbanezNo ratings yet
- Radiation-Related Risks of Imaging - UpToDateDocument28 pagesRadiation-Related Risks of Imaging - UpToDateCeleste MartinezNo ratings yet
- BJR 20219004Document4 pagesBJR 20219004Camilo SotomayorNo ratings yet
- Radiation Exposure and Cost Influence Physician Medical Image Decision MakingDocument5 pagesRadiation Exposure and Cost Influence Physician Medical Image Decision Makingكن صديقيNo ratings yet
- Articulo 1Document13 pagesArticulo 1Lucero BallesterosNo ratings yet
- Evaluation of PT Radiation Dose (2021)Document5 pagesEvaluation of PT Radiation Dose (2021)RenadNo ratings yet
- Comparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldDocument8 pagesComparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldAmalia fhyNo ratings yet
- Utilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainDocument4 pagesUtilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainJorge RodriguezNo ratings yet
- Vaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyDocument7 pagesVaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyFlor ZalazarNo ratings yet
- Solar Radiation and The Incidence and Mortality of Leading Invasive Cancers in The United StatesDocument7 pagesSolar Radiation and The Incidence and Mortality of Leading Invasive Cancers in The United StatesMBNo ratings yet
- Editorial: Breast Carcinogenesis: Risk of RadiationDocument3 pagesEditorial: Breast Carcinogenesis: Risk of RadiationGabriela Silva MartinsNo ratings yet
- Predicting Lung Cancers Using Epidemiological Data: A Generative-Discriminative FrameworkDocument12 pagesPredicting Lung Cancers Using Epidemiological Data: A Generative-Discriminative Frameworkswathi sNo ratings yet
- CBCT Dosimetry: Orthodontic ConsiderationsDocument5 pagesCBCT Dosimetry: Orthodontic Considerationsgriffone1No ratings yet
- Regulatory Toxicology and Pharmacology: CommentaryDocument6 pagesRegulatory Toxicology and Pharmacology: CommentaryRodney SalazarNo ratings yet
- Biblio 19Document22 pagesBiblio 19JuanchoNo ratings yet
- Craniopharyngioma 2 PDFDocument9 pagesCraniopharyngioma 2 PDFBea NufuarNo ratings yet
- Assessing The Health Effects Associated With OccupDocument8 pagesAssessing The Health Effects Associated With OccupShivanie RagoonananNo ratings yet
- Breast CA ScreeningDocument8 pagesBreast CA Screeningchristelm_1No ratings yet
- 10 1053@j Semnuclmed 2020 07 005Document10 pages10 1053@j Semnuclmed 2020 07 005anon_813722240No ratings yet
- Assignment On Occupational Health Hazards of Employees Working in Diagnostic Radiology DepartmentDocument15 pagesAssignment On Occupational Health Hazards of Employees Working in Diagnostic Radiology DepartmentkeerthanamsjNo ratings yet
- 1 s2.0 S2452109422001890Document6 pages1 s2.0 S2452109422001890Raul Matute MartinNo ratings yet
- Effective Dose of Dental CBCT LudlowDocument25 pagesEffective Dose of Dental CBCT LudlowMaríaPazSalinasVillagraNo ratings yet
- 10 1016@j Critrevonc 2020 102962Document16 pages10 1016@j Critrevonc 2020 102962bouh aichetouNo ratings yet
- Examenes Radiologicos y Riesgo de Cancer en PacientesDocument27 pagesExamenes Radiologicos y Riesgo de Cancer en PacientesMaría Isabel Clara Aponte OrtizNo ratings yet
- CBCT Dosimetry Orthodontic ConsiderationsDocument5 pagesCBCT Dosimetry Orthodontic ConsiderationsElzaMMartinsNo ratings yet
- Chapt 1 PeterDocument63 pagesChapt 1 PeterSamson PeterNo ratings yet
- Computed Tomography (CT) Radiation Dose, Patient Safety, and Diagnostic Imaging Quality AssuranceDocument11 pagesComputed Tomography (CT) Radiation Dose, Patient Safety, and Diagnostic Imaging Quality AssuranceAlejandroNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofIsmail Eko SaputraNo ratings yet
- Quantitative Ultrasound Characterization of Responses To Radiotherapy in Cancer Mouse ModelsDocument10 pagesQuantitative Ultrasound Characterization of Responses To Radiotherapy in Cancer Mouse Modelstaufiqur776No ratings yet
- Medical RadiationDocument5 pagesMedical RadiationNadeem NadeemNo ratings yet
- Kei10344 FMDocument4 pagesKei10344 FMbbkanilNo ratings yet
- International Journal of Engineering Research and DevelopmentDocument8 pagesInternational Journal of Engineering Research and DevelopmentIJERDNo ratings yet
- Cancer Risk in 680 000 People Exposed To ComputedDocument18 pagesCancer Risk in 680 000 People Exposed To ComputedRomina VillaseñorNo ratings yet
- Computed Tomography - An Increasing Source of Radiation ExposureDocument8 pagesComputed Tomography - An Increasing Source of Radiation ExposureMANUEL ALEJANDRO LEÓNNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- RescateDocument9 pagesRescateLorena Sánchez PérezNo ratings yet
- Analysis of Cancer Risks in Populations Near Nuclear FacilitiesDocument4 pagesAnalysis of Cancer Risks in Populations Near Nuclear FacilitiesNational Academies of Science, Engineering, and MedicineNo ratings yet
- CancerDocument9 pagesCancerMARIA JOSE RIVERA AVILANo ratings yet
- Article 5Document10 pagesArticle 5Tashu SardaNo ratings yet
- Joc 20074Document9 pagesJoc 20074Eugenia BriciucNo ratings yet
- Internal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionDocument3 pagesInternal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionmarrajoanaNo ratings yet
- Excess Lifetime Cancer Risk Assessment of Radiographers at Some Radiography Facilities in Warri, Delta StateDocument5 pagesExcess Lifetime Cancer Risk Assessment of Radiographers at Some Radiography Facilities in Warri, Delta Stateukerunakpesiri.avwerosuoNo ratings yet
- SBRT PDFDocument14 pagesSBRT PDFrubenNo ratings yet
- Tecnicas Imagenelogicas CancerDocument8 pagesTecnicas Imagenelogicas CancerFranNo ratings yet
- Adjustment of Lifetime Risks of Space Radiation Induced Cancer by T - 2015 - HelDocument51 pagesAdjustment of Lifetime Risks of Space Radiation Induced Cancer by T - 2015 - Helpo hongNo ratings yet
- NIH Public Access: Standardization and Optimization of Computed Tomography Protocols To Achieve Low-DoseDocument14 pagesNIH Public Access: Standardization and Optimization of Computed Tomography Protocols To Achieve Low-DoseMillerNo ratings yet
- Merkell MetaDocument9 pagesMerkell MetaGonzalo RubioNo ratings yet
- Assessment of Polygenic Architecture and Risk PredDocument14 pagesAssessment of Polygenic Architecture and Risk PredanonymousNo ratings yet
- 1 s2.0 S0360301623077350 MainDocument4 pages1 s2.0 S0360301623077350 Mainjohapatino46No ratings yet
- Fonc 13 1162683Document2 pagesFonc 13 1162683vinadata01No ratings yet
- Ferrucci 2014Document6 pagesFerrucci 2014Bobby JimNo ratings yet
- Clinical Oncology: C.W. Williamson, H.C. Liu, J. Mayadev, L.K. MellDocument12 pagesClinical Oncology: C.W. Williamson, H.C. Liu, J. Mayadev, L.K. MellSebastian GarciaNo ratings yet
- Total Marrow Irradiation: A Comprehensive ReviewFrom EverandTotal Marrow Irradiation: A Comprehensive ReviewJeffrey Y. C. WongNo ratings yet
- Glioma Imaging: Physiologic, Metabolic, and Molecular ApproachesFrom EverandGlioma Imaging: Physiologic, Metabolic, and Molecular ApproachesWhitney B. PopeNo ratings yet
- Dentistry 07 00093Document18 pagesDentistry 07 00093Rafa LopezNo ratings yet
- CALGB Schema FinalDocument1 pageCALGB Schema FinalMohamed MahmoudNo ratings yet
- Biochemistry of CancerDocument5 pagesBiochemistry of CancerManasa YNo ratings yet
- BJC 201328Document7 pagesBJC 201328PraveenNo ratings yet
- Ancient Greek and Greco-Roman Methods in Modern Surgical Treatment of CancerDocument3 pagesAncient Greek and Greco-Roman Methods in Modern Surgical Treatment of CancerAlexia ToumpaNo ratings yet
- Pathologic Fractures: H.T. Temple, MD Walter W. Virkus, MDDocument68 pagesPathologic Fractures: H.T. Temple, MD Walter W. Virkus, MDb BNo ratings yet
- Briettavasser Job 15 Letter 12Document2 pagesBriettavasser Job 15 Letter 12api-669728207No ratings yet
- Imunohistochimie LNHDocument4 pagesImunohistochimie LNHHaralambie SarbuNo ratings yet
- Mammography For Breast Cancer ScreeningDocument26 pagesMammography For Breast Cancer Screeningaufar syehanNo ratings yet
- Pancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyDocument4 pagesPancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyMolla WariNo ratings yet
- Gyne LE 2: Stage IVA Is Characterized byDocument49 pagesGyne LE 2: Stage IVA Is Characterized byĐinesh IlavarasanNo ratings yet
- Applied Therapeutics Tenth Edition-2268-2272Document5 pagesApplied Therapeutics Tenth Edition-2268-2272Yuu WidaaNo ratings yet
- Onco Quiz 1Document2 pagesOnco Quiz 1Andrea Mae BernardoNo ratings yet
- IPMN Versus Ampullary AdenomaDocument6 pagesIPMN Versus Ampullary AdenomaedwardNo ratings yet
- HemangiomaDocument15 pagesHemangiomaGrace Febryanti Toding0% (1)
- Surgery Subspecialty - Skin CancerDocument2 pagesSurgery Subspecialty - Skin CancerJonathan AiresNo ratings yet
- Neck Dissection: Tyson J. Nielsen and Audrey B. ErmanDocument3 pagesNeck Dissection: Tyson J. Nielsen and Audrey B. ErmanEndika GGNo ratings yet
- Bloody MaryDocument2 pagesBloody MaryManolache AnaNo ratings yet
- Cáncer de PancreasDocument8 pagesCáncer de PancreasMARIA GABRIELA HERNANDEZ GONTOLNo ratings yet
- Bi RadsDocument5 pagesBi Radsjitendra guptaNo ratings yet
- Fleischner Society Guideline PDFDocument14 pagesFleischner Society Guideline PDFBiswarup PurkayasthaNo ratings yet
- Volum Rezumate ZMN 2023 1Document56 pagesVolum Rezumate ZMN 2023 1LuthienFreyNo ratings yet
- Ductal Carcinoma in SituDocument13 pagesDuctal Carcinoma in SitudrkrsticNo ratings yet
- პათოლოგიური ანატომიაDocument19 pagesპათოლოგიური ანატომიაTea TodriaNo ratings yet
- Chapter 4 Study Guide ANSWERS For The Test Review 2015Document14 pagesChapter 4 Study Guide ANSWERS For The Test Review 2015Wengelu evanNo ratings yet
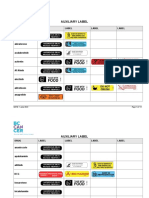
- Auxiliary Label LISTDocument14 pagesAuxiliary Label LISTAbdur RachmanNo ratings yet