You might also like
- Items of Work For RoadsDocument6 pagesItems of Work For Roadsjhc1123No ratings yet
- Standard Welding Procedure SpecificationsDocument2 pagesStandard Welding Procedure SpecificationsAnonymous dh6DITNo ratings yet
- Bipap Ventilation Basic and MonitoringDocument33 pagesBipap Ventilation Basic and MonitoringPradip ChougaleNo ratings yet
- Quiz 2 Principles of DesignDocument4 pagesQuiz 2 Principles of DesignJovito Reyes0% (1)
- Dr. Rosi - CPAPDocument65 pagesDr. Rosi - CPAPtom24No ratings yet
- Noninvasive Ventilation in ChildrenDocument96 pagesNoninvasive Ventilation in ChildrenbhongskirnNo ratings yet
- CH 19-Noninvasive VentilationDocument65 pagesCH 19-Noninvasive VentilationGhaida AlshehriNo ratings yet
- DR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineDocument22 pagesDR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineP Vinod KumarNo ratings yet
- Auto-Peep (Intrinsic Peep)Document49 pagesAuto-Peep (Intrinsic Peep)Spring Bommie100% (1)
- Continuous Positive Airway Pressure (CPAP)Document53 pagesContinuous Positive Airway Pressure (CPAP)indiamahesh100% (1)
- NIV TeachingDocument12 pagesNIV TeachingZahraa Al-MayahiNo ratings yet
- Ventilatory MNGTDocument31 pagesVentilatory MNGTlianrose448No ratings yet
- Federal Democratic Republic of Ethiopia Ministry of HealthDocument43 pagesFederal Democratic Republic of Ethiopia Ministry of HealthdagemNo ratings yet
- Cpap 2011-13Document5 pagesCpap 2011-13Rajender SinghNo ratings yet
- Role of Physiotherapy in ICUDocument68 pagesRole of Physiotherapy in ICUprasanna3k100% (2)
- NIPPVDocument35 pagesNIPPVAnusha VergheseNo ratings yet
- BiPAP ManyDocument47 pagesBiPAP ManyHarshit RastogiNo ratings yet
- Resp TestDocument7 pagesResp TestKong KongNo ratings yet
- Weaning From VentilatorDocument45 pagesWeaning From VentilatorJerinNo ratings yet
- Wa0010.Document80 pagesWa0010.Amritha GeorgeNo ratings yet
- AMV 1 Lec and LabDocument63 pagesAMV 1 Lec and Lablady birdNo ratings yet
- Basics of Mechanical VentilationDocument208 pagesBasics of Mechanical VentilationAnonymous ORleRr100% (1)
- Cpap-Bipap: Sussan Soltani Mohammadi - MDDocument41 pagesCpap-Bipap: Sussan Soltani Mohammadi - MDbandarascbNo ratings yet
- Weaning Ventilator Protocol For LiberationDocument3 pagesWeaning Ventilator Protocol For LiberationBonny ChristianNo ratings yet
- CPAP in PretermDocument25 pagesCPAP in PretermNasrNo ratings yet
- Critical Care Clinical Procedures 2023Document38 pagesCritical Care Clinical Procedures 2023nucahersheyskatNo ratings yet
- Oxygen Delivery Devices: Reported By: Marvin PermisonDocument18 pagesOxygen Delivery Devices: Reported By: Marvin PermisonMedeah Faye AbesNo ratings yet
- Lung Expansion RevisionDocument89 pagesLung Expansion RevisionPatrick RoqueNo ratings yet
- Ventilator 1 1Document36 pagesVentilator 1 1Misha NazirNo ratings yet
- Aha Ventilación Modulo 3Document11 pagesAha Ventilación Modulo 3Juan Carlos GomezNo ratings yet
- Mechanical VentilationDocument19 pagesMechanical VentilationAashay DwivediNo ratings yet
- NIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDocument38 pagesNIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDr mahi sNo ratings yet
- Non-Invasive Ventilation 2Document25 pagesNon-Invasive Ventilation 2Ramanesh DNo ratings yet
- Manual Hyper InflationDocument39 pagesManual Hyper InflationDeepa SuvarnaNo ratings yet
- CpapDocument33 pagesCpapAtikah Putri AtmojoNo ratings yet
- Intermittent Positive Pressure BreathingDocument12 pagesIntermittent Positive Pressure BreathingHitesh RohitNo ratings yet
- Management of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Document7 pagesManagement of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Abhishek GoelNo ratings yet
- BipapDocument26 pagesBipapTnem NatNo ratings yet
- Niv in CopdDocument54 pagesNiv in Copdmahmod omerNo ratings yet
- AnswersDocument4 pagesAnswersKhadijah AhmedNo ratings yet
- Non Invasive Ventilation - DR RinaDocument76 pagesNon Invasive Ventilation - DR RinaTitik sukamtiNo ratings yet
- Blue 717 CPAP GuidelinesDocument18 pagesBlue 717 CPAP GuidelinesElrasheid AwoodaNo ratings yet
- Lung Expansion TherapyDocument108 pagesLung Expansion TherapyJean NoronhaNo ratings yet
- Practical Application of CPAP: Dr. Srinivas MurkiDocument8 pagesPractical Application of CPAP: Dr. Srinivas MurkiRaji MohanNo ratings yet
- Intubation and O2 Basics - Chuko EditDocument34 pagesIntubation and O2 Basics - Chuko EditJon Chuko100% (1)
- WeaningDocument55 pagesWeaningKamal Mohamed100% (1)
- BAL ProsedurDocument2 pagesBAL ProsedurisnanrNo ratings yet
- Respiratory Care ModalitiesDocument63 pagesRespiratory Care ModalitiesErica Clerigo LandichoNo ratings yet
- Lung Expansion 1Document31 pagesLung Expansion 11trindogg100% (2)
- Respiratory Medical Residents PresentationDocument50 pagesRespiratory Medical Residents PresentationRayhan ShariffNo ratings yet
- Indications For Mechanical VentilationDocument25 pagesIndications For Mechanical VentilationKenneth Jay EdnacoNo ratings yet
- BipapDocument26 pagesBipapالغائب الحاضرNo ratings yet
- Final VentilatorDocument62 pagesFinal VentilatorDrmirfat AlkashifNo ratings yet
- Suctioning Trache Care NebuDocument11 pagesSuctioning Trache Care NebuROLAND LAURENCE BARGO JARDIOLINNo ratings yet
- Weaning From Mechanical Ventilation: Akella Chendrasekhar MD FACS FCCPDocument37 pagesWeaning From Mechanical Ventilation: Akella Chendrasekhar MD FACS FCCPNadiya AshifNo ratings yet
- Mechanical Ventilation: Reported By: Sembrana Ii, Gloria TRINIDAD, Anna PatriciaDocument55 pagesMechanical Ventilation: Reported By: Sembrana Ii, Gloria TRINIDAD, Anna PatriciaElaine IsalosNo ratings yet
- DT Ventilasi MekanikDocument53 pagesDT Ventilasi MekanikRadinal MauludiNo ratings yet
- Why This Topic?Document6 pagesWhy This Topic?duhsknwsNo ratings yet
- Ventilated Patient Care.Document25 pagesVentilated Patient Care.Rashmi BoraNo ratings yet
- Monitoring & Care of Ventilated ChildrenDocument12 pagesMonitoring & Care of Ventilated ChildrenRajakumar Padur Sivaraman100% (2)
- Lp3 Ventilatia MecanicaDocument43 pagesLp3 Ventilatia MecanicaAlexandra SerbanNo ratings yet
- Safe SuctioningDocument31 pagesSafe SuctioningKatrina Ponce100% (2)
- Baremos Sexual Desire Inventory MEN WomenDocument1 pageBaremos Sexual Desire Inventory MEN WomenGabriNo ratings yet
- Mcbe2798 e 10 1Document42 pagesMcbe2798 e 10 1Manh DuyNo ratings yet
- Sa 387Document6 pagesSa 387ismaelarchilacastilloNo ratings yet
- The Mole ConceptDocument12 pagesThe Mole ConceptVictor OkosunNo ratings yet
- Real Time DC Water Tank Level Control Using Arduino Mega 2560Document6 pagesReal Time DC Water Tank Level Control Using Arduino Mega 2560Sam ArNo ratings yet
- ACP Supplement For SVR AUG 2017Document104 pagesACP Supplement For SVR AUG 2017Kasun WijerathnaNo ratings yet
- Basic Labour Rate ListDocument6 pagesBasic Labour Rate ListmaheshNo ratings yet
- DSP Lab RecordDocument97 pagesDSP Lab RecordLikhita UttamNo ratings yet
- Unit Operation QBDocument7 pagesUnit Operation QBsmg26thmayNo ratings yet
- Police Log July 30, 2016Document16 pagesPolice Log July 30, 2016MansfieldMAPoliceNo ratings yet
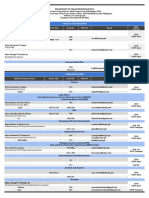
- Updated DOTr Directory As of 29 October 2021Document9 pagesUpdated DOTr Directory As of 29 October 2021Twinkle MiguelNo ratings yet
- 1 Aerodynamics Lecture - Viscous FlowDocument70 pages1 Aerodynamics Lecture - Viscous Flowccoyure100% (2)
- BITEBUDZ COMPANY EME Kemerut 1Document31 pagesBITEBUDZ COMPANY EME Kemerut 1Mark LightNo ratings yet
- Temba KauDocument50 pagesTemba KaufauzanNo ratings yet
- Ste FannyDocument17 pagesSte FannyElmer DE LA CruzNo ratings yet
- ActuatorsDocument24 pagesActuatorsharishcsharmaNo ratings yet
- Thank You For Your Order: Power & Signal Group PO BOX 856842 MINNEAPOLIS, MN 55485-6842Document1 pageThank You For Your Order: Power & Signal Group PO BOX 856842 MINNEAPOLIS, MN 55485-6842RuodNo ratings yet
- H250 H250 H250 H250: Variable Area Flowmeter With 3W2 Angular Position TransmitterDocument40 pagesH250 H250 H250 H250: Variable Area Flowmeter With 3W2 Angular Position TransmitterJustine MarashanyeNo ratings yet
- CekocideDocument1 pageCekocideKaren Claire HorcaNo ratings yet
- JBL Constant Beamwidth Technology - CBT Series Passive Controlled-Coverage ColumnsDocument12 pagesJBL Constant Beamwidth Technology - CBT Series Passive Controlled-Coverage ColumnsTom HampleNo ratings yet
- Montague Street Cable Car, Wall Street FerryDocument23 pagesMontague Street Cable Car, Wall Street FerryBob DiamondNo ratings yet
- Irving Hallowell - Ojibwa Ontology, Behavior and World ViewDocument24 pagesIrving Hallowell - Ojibwa Ontology, Behavior and World ViewFa Di LaNo ratings yet
- Vandex Plug: Rapid-Setting, Crystalline Hydraulic CementDocument2 pagesVandex Plug: Rapid-Setting, Crystalline Hydraulic CementQuerubin EboliNo ratings yet
- Assignment 33 PDFDocument9 pagesAssignment 33 PDFsayan mukherjeeNo ratings yet
- Scientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewDocument18 pagesScientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewsrichainuluNo ratings yet
- EmpathyDocument5 pagesEmpathyHijaab KhaanNo ratings yet
- Polynesian MigrationsDocument2 pagesPolynesian Migrationskinneyjeffrey100% (1)