You might also like
- Herbs by Sebastian DebskiDocument9 pagesHerbs by Sebastian DebskiYakuma HotaruNo ratings yet
- Skin Beauty InjectionsDocument12 pagesSkin Beauty Injectionst3kla100% (1)
- Yoga For DepressionDocument12 pagesYoga For DepressionSoulyogaNo ratings yet
- 9.2018.occlusal Onlays As A Modern Treatment Concept For The Reconstruction of Severely Worn Occlusal SurfacespdfDocument14 pages9.2018.occlusal Onlays As A Modern Treatment Concept For The Reconstruction of Severely Worn Occlusal Surfacespdfluis alejandroNo ratings yet
- Maple Syrup Urine Disease (MSUD)Document28 pagesMaple Syrup Urine Disease (MSUD)Dr. Mohammed Al Ja’fari, MDNo ratings yet
- CM692 Im6129 Yh135 PDFDocument90 pagesCM692 Im6129 Yh135 PDFmoises100% (1)
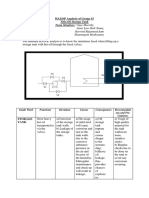
- HAZOP Analysis of Group 15: Isaac Law Shek Xiang Harvind Rajamanickam Shanmugam MuthusamyDocument2 pagesHAZOP Analysis of Group 15: Isaac Law Shek Xiang Harvind Rajamanickam Shanmugam Muthusamyvijaymoorthy14No ratings yet
- Taking Body MeasurementsDocument86 pagesTaking Body MeasurementsMariel Liza HernandezNo ratings yet
- One Stage Aesthetic and Functional Reconstruction of Major Lower Lip DefectsDocument5 pagesOne Stage Aesthetic and Functional Reconstruction of Major Lower Lip DefectsDr. Hilder HernandezNo ratings yet
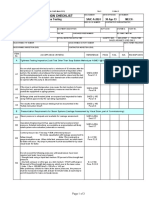
- SAIC-A-2024 Rev 6 Leakness Tightness TestDocument3 pagesSAIC-A-2024 Rev 6 Leakness Tightness Testpookkoya thangalNo ratings yet
- Presurgical Infant Orthopedics For Cleft Lip and PDocument6 pagesPresurgical Infant Orthopedics For Cleft Lip and PPark JiminNo ratings yet
- Botswana-Upenn Partnership: Basic SetswanaDocument10 pagesBotswana-Upenn Partnership: Basic SetswanakhumisoNo ratings yet
- Jianhua Liu (Editor), Bing Shi (Editor) - Atlas of Lip and Nose Plastic and Cosmetic Surgery-Springer (2021)Document199 pagesJianhua Liu (Editor), Bing Shi (Editor) - Atlas of Lip and Nose Plastic and Cosmetic Surgery-Springer (2021)Uyen NguyenNo ratings yet
- Treatment Trends in PeriodonticsDocument8 pagesTreatment Trends in Periodonticspatricia sotoNo ratings yet
- The Lips-45 Injection Techniques For Esthetic Lip TreatmentDocument347 pagesThe Lips-45 Injection Techniques For Esthetic Lip TreatmentOscar Parra de Carrizosa100% (1)
- Lip RepositioningDocument5 pagesLip RepositioningNurul Novita SuhartonoNo ratings yet
- Lip LiftDocument14 pagesLip LiftGuilherme BergantonNo ratings yet
- ITR Filing Project Report by VenkyDocument38 pagesITR Filing Project Report by VenkyVyankatesh Gotalkar50% (6)
- SJZ 108Document8 pagesSJZ 108Guilherme BergantonNo ratings yet
- Ann Burns and Fire Disasters 22 90Document7 pagesAnn Burns and Fire Disasters 22 90alinutza_childNo ratings yet
- Marcus 2017Document17 pagesMarcus 2017Desrainy InhardiniNo ratings yet
- Gox 9 E3999Document3 pagesGox 9 E3999lorena gurdzNo ratings yet
- Lip Lowering SurgeryDocument15 pagesLip Lowering SurgeryPrathik RaiNo ratings yet
- Clinical Practice Guideline For The Use of Fillers in Non Surgical RhinoplastyDocument25 pagesClinical Practice Guideline For The Use of Fillers in Non Surgical RhinoplastyDachi DavitashviliNo ratings yet
- Liprepositioning Techniquesand Modifications: Dimitris N. TatakisDocument12 pagesLiprepositioning Techniquesand Modifications: Dimitris N. TatakisWayan Sutresna YasaNo ratings yet
- Ultraconservative Approach For Caries ManagementDocument12 pagesUltraconservative Approach For Caries ManagementRajsandeep SinghNo ratings yet
- Sjac 126Document18 pagesSjac 126dukedevils27No ratings yet
- Case Report On Lip Repositioning: A Boon For Gummy Smile PatientsDocument7 pagesCase Report On Lip Repositioning: A Boon For Gummy Smile Patientsanshum guptaNo ratings yet
- JAMA Facial Plastic Surgery: Novel Use of A Volumizing Hyaluronic Acid Filler For Treatment of Infraorbital HollowsDocument23 pagesJAMA Facial Plastic Surgery: Novel Use of A Volumizing Hyaluronic Acid Filler For Treatment of Infraorbital HollowsDr. Hilder HernandezNo ratings yet
- Periodontal Approach To Esthetic Dentistry: February 2015Document6 pagesPeriodontal Approach To Esthetic Dentistry: February 2015silpayNo ratings yet
- Periodontal Approach To Esthetic Dentistry: February 2015Document6 pagesPeriodontal Approach To Esthetic Dentistry: February 2015Joshua Diaz QuiquijanaNo ratings yet
- Article Direct Lip Lift Sashimi TechniqueDocument7 pagesArticle Direct Lip Lift Sashimi TechniqueMichelly Mendonça AlvarengaNo ratings yet
- A Safe and Effective Lip Augmentation Method: The Step-by-Step Φ (Phi) TechniqueDocument7 pagesA Safe and Effective Lip Augmentation Method: The Step-by-Step Φ (Phi) TechniqueDr. Hilder HernandezNo ratings yet
- Children 11 00332 v2Document12 pagesChildren 11 00332 v2salahoveNo ratings yet
- Knowledge, Awareness and Practice On Application of Presurgical Nasoalveolar Moulding For Cleft Lip and Palate PatientsDocument8 pagesKnowledge, Awareness and Practice On Application of Presurgical Nasoalveolar Moulding For Cleft Lip and Palate PatientsArshid KhandayNo ratings yet
- A Lip Exercises in Orthodontics: A Review Article: April 2022Document11 pagesA Lip Exercises in Orthodontics: A Review Article: April 2022habeebNo ratings yet
- Review Article: Karoon AgrawalDocument9 pagesReview Article: Karoon Agrawalshagun singhNo ratings yet
- Pres OrtopDocument7 pagesPres OrtopDiana PredaNo ratings yet
- Penna 2014Document7 pagesPenna 2014xvfzt4vkbgNo ratings yet
- Skin Research and Technology - 2023 - Shirani - Evaluating The Results of Eyebrow Lift by Combining Methods of SubcutaneousDocument7 pagesSkin Research and Technology - 2023 - Shirani - Evaluating The Results of Eyebrow Lift by Combining Methods of Subcutaneousmariaeduardadeoliveiracoelho1No ratings yet
- Lindsay 2010Document2 pagesLindsay 2010Stelescu AndrasNo ratings yet
- Quality of Life Assessment of Patients Utilizing Orbital Implant Supported ProsthesesDocument6 pagesQuality of Life Assessment of Patients Utilizing Orbital Implant Supported ProsthesesBagis Emre GulNo ratings yet
- Treatment of Gummy Smile of Multifactorial Etiology: A Case ReportDocument16 pagesTreatment of Gummy Smile of Multifactorial Etiology: A Case ReportMed-Amine TouloutNo ratings yet
- Cleft Lip & Palate SurgeryDocument5 pagesCleft Lip & Palate SurgeryShoaib A. KaziNo ratings yet
- Gox 9 E3957Document8 pagesGox 9 E3957lorena gurdzNo ratings yet
- Effectiveness of Brushing Teeth in Patients With Reduced Oral Hygiene by Laypeople: A Randomized, Controlled StudyDocument12 pagesEffectiveness of Brushing Teeth in Patients With Reduced Oral Hygiene by Laypeople: A Randomized, Controlled StudyMarco Antonio García LunaNo ratings yet
- Nose Tip Elongation and Elevation: A Novel Filler Injection TechniqueDocument17 pagesNose Tip Elongation and Elevation: A Novel Filler Injection TechniqueJuan AvonNo ratings yet
- 221-Article Manuscript-403-1-10-20171006Document6 pages221-Article Manuscript-403-1-10-20171006Aji Prasetyo UtomoNo ratings yet
- Medoral 27 E257Document8 pagesMedoral 27 E257vanessa_werbickyNo ratings yet
- Plastic Surgery Combined With Orthodontic and Orthognathic ProceduresDocument3 pagesPlastic Surgery Combined With Orthodontic and Orthognathic ProceduresAdit VekariaNo ratings yet
- Clinical Assessment of A Combination Lip TreatmentDocument6 pagesClinical Assessment of A Combination Lip TreatmentDummy CipawNo ratings yet
- Everything Ocu Lop Last I A Make e Up PermanentDocument8 pagesEverything Ocu Lop Last I A Make e Up PermanentDaritza C. MoyanoNo ratings yet
- Clinical Considerations For Increasing Occlusal Vertical DimensionDocument9 pagesClinical Considerations For Increasing Occlusal Vertical DimensionAmar BhochhibhoyaNo ratings yet
- Procedures Performed: Surgical Treatment For Cleft Lip and Cleft PalateDocument4 pagesProcedures Performed: Surgical Treatment For Cleft Lip and Cleft PalateNars Dan DomsNo ratings yet
- 10.1007@s10006 020 00857 4Document6 pages10.1007@s10006 020 00857 4Martha Lia Castaño EcheverryNo ratings yet
- Content ServerDocument10 pagesContent ServerJose Antonio Figuroa AbadoNo ratings yet
- Urdialesglvez 2017Document11 pagesUrdialesglvez 2017Armin ArceoNo ratings yet
- Future of Laser Pediatric Dentistry PDFDocument5 pagesFuture of Laser Pediatric Dentistry PDFsnehasthaNo ratings yet
- Qoa05016 342 348Document7 pagesQoa05016 342 348Humberto CanoNo ratings yet
- LipflpbotoxDocument4 pagesLipflpbotoxAlexandra Luz StodieckNo ratings yet
- пожтяжка губ 4Document6 pagesпожтяжка губ 4Alexey SorokinNo ratings yet
- Pre-Prosthetic Periodontal Surgery To Enhance Patient's Esthetic Need: Case SeriesDocument7 pagesPre-Prosthetic Periodontal Surgery To Enhance Patient's Esthetic Need: Case SeriesSergio Losada AmayaNo ratings yet
- Content ServerDocument7 pagesContent ServerGreisy Saym Cruz FelixNo ratings yet
- Wound Care Debra Uk 2012Document42 pagesWound Care Debra Uk 2012Livia GrigoreNo ratings yet
- Endolaser Treatment of Aesthetic Disorders ClinicaDocument13 pagesEndolaser Treatment of Aesthetic Disorders ClinicaErik BrooksNo ratings yet
- Medicina Basada en Evidencia. Paladar HendidoDocument5 pagesMedicina Basada en Evidencia. Paladar HendidoDanisse RoaNo ratings yet
- Full-Mouth Rehabilitation of Worn Dentition by HobDocument9 pagesFull-Mouth Rehabilitation of Worn Dentition by Hobdea swastikaNo ratings yet
- Death Penalty 1Document4 pagesDeath Penalty 1Samantha SantiagoNo ratings yet
- (23007451 - Special Matrices) Best Linear Unbiased Estimation For Varying Probability With and Without Replacement SamplingDocument14 pages(23007451 - Special Matrices) Best Linear Unbiased Estimation For Varying Probability With and Without Replacement Samplingjedielso salesNo ratings yet
- Industrial Waste SurweyDocument34 pagesIndustrial Waste SurweyOmaya TariqNo ratings yet
- IOT Based Accident Detection and PreventionDocument6 pagesIOT Based Accident Detection and PreventionShivani PatilNo ratings yet
- Introduction To Community Based ProgramDocument6 pagesIntroduction To Community Based ProgramSenpai Aris AriasNo ratings yet
- Tonetti Et Al-2018-Journal of Periodontology TDocument14 pagesTonetti Et Al-2018-Journal of Periodontology TJonathan Meza MauricioNo ratings yet
- Topic 3 - Crisis Management PolicyDocument10 pagesTopic 3 - Crisis Management PolicyArjay JulianNo ratings yet
- Diare Oktober 3Document2 pagesDiare Oktober 3anggaNo ratings yet
- S2 V150C 3Document2 pagesS2 V150C 3Raden ArdyNo ratings yet
- Review of Urban Drainage, 4th Edition, by David Butler, Christopher James Digman, Christos Makropoulos, and John W. DaviesDocument1 pageReview of Urban Drainage, 4th Edition, by David Butler, Christopher James Digman, Christos Makropoulos, and John W. DaviesJhon Edison Bravo Buitrago100% (1)
- IfatDocument19 pagesIfatTehseenQouserNo ratings yet
- Electrochemical CellDocument9 pagesElectrochemical CellchethanNo ratings yet
- BIOC1020 Course Document - Outline - SSCDocument4 pagesBIOC1020 Course Document - Outline - SSCbrownjudeaaNo ratings yet
- Disinfectants Meeting British Standard As of 23 July 2012Document3 pagesDisinfectants Meeting British Standard As of 23 July 2012karen_meadows2782No ratings yet
- Real Time Respiration Rate Measurement Using Temperature SensorDocument3 pagesReal Time Respiration Rate Measurement Using Temperature SensorEditor IJRITCCNo ratings yet
- Sci4 ST2 Q3Document2 pagesSci4 ST2 Q3KayelNo ratings yet
- Tarea 3 de Ingles IIDocument6 pagesTarea 3 de Ingles IINelly SalcedoNo ratings yet
- Motor Oil ENGDocument64 pagesMotor Oil ENGNicolai BelocosovNo ratings yet
- SOAL-EBS-2 BASING-X-2012-sentosaDocument4 pagesSOAL-EBS-2 BASING-X-2012-sentosaAnthon KurniadiNo ratings yet
- Sarnacol 2142S PDS Sika SarnafilDocument3 pagesSarnacol 2142S PDS Sika SarnafilKRISHNA PRASATH SNo ratings yet
- Sernet Data Sheet PDFDocument2 pagesSernet Data Sheet PDFisctomaslopezNo ratings yet