You might also like
- Rosa 2014Document6 pagesRosa 2014Michal PerkowskiNo ratings yet
- Maintenance of Gingival Form Following Implant PlacementDocument4 pagesMaintenance of Gingival Form Following Implant PlacementRomina BitaNo ratings yet
- Tunnel Access For Guided Bone Regeneration in The Maxillary AnteriorDocument6 pagesTunnel Access For Guided Bone Regeneration in The Maxillary Anteriormax100% (1)
- 10 Keys of Single Implant in Esthetic ZoneDocument15 pages10 Keys of Single Implant in Esthetic ZoneAya Ibrahim Yassin100% (1)
- A Simplified Space Regainer and Functional Space Maintainer - A Case ReportDocument3 pagesA Simplified Space Regainer and Functional Space Maintainer - A Case ReportMohd Ghaus100% (1)
- Role of Mini-Implants in OrthodonticsDocument9 pagesRole of Mini-Implants in OrthodonticsRonald WilfredNo ratings yet
- Laryngology NotesDocument296 pagesLaryngology Notesadham bani younesNo ratings yet
- 10 Tips About Aesthetic ImplantologyDocument16 pages10 Tips About Aesthetic ImplantologyMario Troncoso Andersenn0% (1)
- Art Perfil de Emergencia Implantes PDFDocument7 pagesArt Perfil de Emergencia Implantes PDFdiego alenadro trujilloNo ratings yet
- Complications of Using Retraction CordDocument4 pagesComplications of Using Retraction CordAya Ibrahim YassinNo ratings yet
- 2017 Levine Compendium 10 Keys1 PDFDocument14 pages2017 Levine Compendium 10 Keys1 PDFMohamed AliNo ratings yet
- 2016 Van DooremDocument10 pages2016 Van Dooremkatherina rozicNo ratings yet
- Jpis 42 105Document5 pagesJpis 42 105Jean Pierre Alcántara VigoNo ratings yet
- Andre Sadooun - Posicionsmento Tridimensional Do ImplanteDocument11 pagesAndre Sadooun - Posicionsmento Tridimensional Do ImplanteJefferson ThomazNo ratings yet
- Hollow Maxillary DentureDocument5 pagesHollow Maxillary DentureDeasireeNo ratings yet
- Development of Implant Soft Tissue Emergence ProfileDocument5 pagesDevelopment of Implant Soft Tissue Emergence ProfilemishNo ratings yet
- Protocol: A Restorative Protocol For Implants Replacing Adjacent Maxillary CentralDocument6 pagesProtocol: A Restorative Protocol For Implants Replacing Adjacent Maxillary CentralCuyo GarciaNo ratings yet
- Esthetic Crown Lengthening With FlaplessDocument7 pagesEsthetic Crown Lengthening With FlaplessRamona elenaNo ratings yet
- The Biotransfer Approach: The Use of An Alveolar Cast Die For The Fabrication of The Emergence Profile On Implant-Supported Interim RestorationsDocument4 pagesThe Biotransfer Approach: The Use of An Alveolar Cast Die For The Fabrication of The Emergence Profile On Implant-Supported Interim RestorationsClaudioNo ratings yet
- Document PDFDocument4 pagesDocument PDFBagis Emre GulNo ratings yet
- The Team ApproachDocument2 pagesThe Team ApproachThe SmileNo ratings yet
- Bone Ring 1Document6 pagesBone Ring 1Pradusha RevuruNo ratings yet
- Technique For Soft Tissue Modification For Pontic Reception: A Case ReportDocument4 pagesTechnique For Soft Tissue Modification For Pontic Reception: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Crown ContoursDocument6 pagesCrown ContoursCarlos PerezNo ratings yet
- Diastema Closure With Direct Composite: Architectural Gingival ContouringDocument6 pagesDiastema Closure With Direct Composite: Architectural Gingival ContouringDiego SarunNo ratings yet
- Double Jaw Immediate Load Hybrids: Case Abstract: Scott E. Keith, DDS, MsDocument3 pagesDouble Jaw Immediate Load Hybrids: Case Abstract: Scott E. Keith, DDS, MsShyam BhatNo ratings yet
- Management of Fractured Lateral Incisor by Surgical Extrusion and Its Prosthetic RehabilitationA Case ReportDocument5 pagesManagement of Fractured Lateral Incisor by Surgical Extrusion and Its Prosthetic RehabilitationA Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ilovepdf MergedDocument21 pagesIlovepdf MergedJúlia OliveiraNo ratings yet
- CCD 4 509Document3 pagesCCD 4 509gbaez.88No ratings yet
- 265-Article Text-1516-2-10-20200110 PDFDocument5 pages265-Article Text-1516-2-10-20200110 PDFmarwaNo ratings yet
- A Tooth-Stabilized Surgical Template For AlveolectomyDocument3 pagesA Tooth-Stabilized Surgical Template For Alveolectomyheri asriyadiNo ratings yet
- Decoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownDocument4 pagesDecoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownJuan Carlos MeloNo ratings yet
- Distalization of Impacted Mandibular SecondDocument6 pagesDistalization of Impacted Mandibular SecondPatricia BurbanoNo ratings yet
- Mandibular Molar Protraction With Orthodontic Temporary Anchorage Devices: A Case ReportDocument4 pagesMandibular Molar Protraction With Orthodontic Temporary Anchorage Devices: A Case ReportKanish AggarwalNo ratings yet
- 7 - 2020 - A Digital Intraoral Implant Scan Technique Using A Combined Healing Abutment and Scan Body SystemDocument4 pages7 - 2020 - A Digital Intraoral Implant Scan Technique Using A Combined Healing Abutment and Scan Body SystemVõHoàngThủyTiênNo ratings yet
- Protocol For Indirect Restoration Intraoral Scanning Under Dental Dam Isolation A Dental TechniqueDocument5 pagesProtocol For Indirect Restoration Intraoral Scanning Under Dental Dam Isolation A Dental Techniquefloressam2000No ratings yet
- Full Mouth Rehabilitation With One Piece Implants - A Case ReportDocument3 pagesFull Mouth Rehabilitation With One Piece Implants - A Case ReportSalem Fathi BermawiNo ratings yet
- AsdfaDocument4 pagesAsdfaFree PizzaNo ratings yet
- 6.prd 20 1 Grunder 2Document8 pages6.prd 20 1 Grunder 2Sebastián BernalNo ratings yet
- Evaluation of Interarch Space For ImplanDocument4 pagesEvaluation of Interarch Space For Implanwaf51No ratings yet
- Digital Immediate Denture: A Clinical ReportDocument4 pagesDigital Immediate Denture: A Clinical ReportdeviNo ratings yet
- The Bio-Col TechniqueDocument9 pagesThe Bio-Col TechniquewnelsenNo ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument10 pagesThe International Journal of Periodontics & Restorative DentistryGerard GonzalezNo ratings yet
- 1 s2.0 S0377529115300626 MainDocument6 pages1 s2.0 S0377529115300626 MainNémethBálintNo ratings yet
- The Gray Zone Around Dental Implants - Keys To Esthetic SuccessDocument20 pagesThe Gray Zone Around Dental Implants - Keys To Esthetic SuccessZardasht NajmadineNo ratings yet
- 2004 GamborenaDocument14 pages2004 GamborenamarcelodentNo ratings yet
- Admin, Anita Poster Full Text (Revisi 1)Document5 pagesAdmin, Anita Poster Full Text (Revisi 1)prostodonsiaNo ratings yet
- Tilted Implants For A Mandibular Hybrid Prosthesis: James A. Rivers, DMD, MhsDocument4 pagesTilted Implants For A Mandibular Hybrid Prosthesis: James A. Rivers, DMD, MhsSummer HorneNo ratings yet
- Fulltext - Jda v5 Id1107Document3 pagesFulltext - Jda v5 Id1107Sahana RangarajanNo ratings yet
- Immediate Dentoalveolar RestorationDocument8 pagesImmediate Dentoalveolar RestorationДмитрий ЦененкоNo ratings yet
- Apiko 3Document4 pagesApiko 3Asri DamayantiNo ratings yet
- Fiber FRC Cutom MadeDocument4 pagesFiber FRC Cutom MadesulistiyaNo ratings yet
- 2 - 2023 - Novel Technique For Placement of Immediate Implant in Mandibular RegionDocument5 pages2 - 2023 - Novel Technique For Placement of Immediate Implant in Mandibular RegionVõHoàngThủyTiênNo ratings yet
- A New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueDocument4 pagesA New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueKarin Noga VerhagenNo ratings yet
- Restoring Smile by Esthetic Intraradiular Tooth Reinforcement and Metal Free Crown: A Case ReportDocument3 pagesRestoring Smile by Esthetic Intraradiular Tooth Reinforcement and Metal Free Crown: A Case ReportAmadeaNo ratings yet
- Tasaka DKK 2022Document6 pagesTasaka DKK 2022Krysa AquilaNo ratings yet
- 371-Article Text-1509-3-10-20210710Document6 pages371-Article Text-1509-3-10-20210710Fransiski HoNo ratings yet
- Telescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaDocument5 pagesTelescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaRani PutriNo ratings yet
- Conservative Mangement of Tilted AbutmentsDocument3 pagesConservative Mangement of Tilted Abutmentsrayavarapu sunilNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- 7 implant 到 IAN 距離Document6 pages7 implant 到 IAN 距離iamkyantsaiNo ratings yet
- Yukna1976 Junctional EpitheliumDocument9 pagesYukna1976 Junctional EpitheliumiamkyantsaiNo ratings yet
- 牙周傷口癒合wikesj1990Document6 pages牙周傷口癒合wikesj1990iamkyantsaiNo ratings yet
- 表觀遺傳與農業發展(下)Document3 pages表觀遺傳與農業發展(下)iamkyantsaiNo ratings yet
- Surgery - 2020 With CorrectionDocument74 pagesSurgery - 2020 With CorrectionUmar JameelNo ratings yet
- Pengkajian Luka Bates JensenDocument6 pagesPengkajian Luka Bates JensenocsitaocsitulNo ratings yet
- Banco de Preguntas ReabilitacionDocument19 pagesBanco de Preguntas ReabilitacionVanessa AlcantaraNo ratings yet
- JRAM Volume 3 Issue 1 Pages 67-74Document8 pagesJRAM Volume 3 Issue 1 Pages 67-74Rehab BassamNo ratings yet
- Lumus Staff MRI QuestionnaireDocument1 pageLumus Staff MRI Questionnairejwidja12345No ratings yet
- The Obstetric Gynaecologis - 2023 - Davies - The Clinical Applications of Interventional Radiological Techniques inDocument30 pagesThe Obstetric Gynaecologis - 2023 - Davies - The Clinical Applications of Interventional Radiological Techniques inPrernaNo ratings yet
- Flower of Service: Information Payment ConsultationDocument4 pagesFlower of Service: Information Payment ConsultationPranidhya JoshiNo ratings yet
- DR Luca Vricella Interview Transcript 1Document19 pagesDR Luca Vricella Interview Transcript 1api-690757487No ratings yet
- ChitrabDocument119 pagesChitrabANKISETTI BHARATHKUMARNo ratings yet
- Change in Crown-to-Implant Ratio of Implants Placed in Grafted and Nongrafted Posterior Maxillary Sites: A 5-Year Prospective Randomized StudyDocument6 pagesChange in Crown-to-Implant Ratio of Implants Placed in Grafted and Nongrafted Posterior Maxillary Sites: A 5-Year Prospective Randomized StudyValeria CrespoNo ratings yet
- 1333-How To Stroke Wrinkles Right Out of Your FaceDocument5 pages1333-How To Stroke Wrinkles Right Out of Your FaceTinuola WritingNo ratings yet
- Coek - Info Barratt Boyes Cardiac Surgery 3rd EdDocument2 pagesCoek - Info Barratt Boyes Cardiac Surgery 3rd EdAhmet ŞimşekNo ratings yet
- CUTASEPTDocument4 pagesCUTASEPTAlvin Ferdinand Ace CastroNo ratings yet
- Vacuum Assisted ClosureDocument5 pagesVacuum Assisted ClosurerodtobingNo ratings yet
- (JOP) JUNG 2008 - Histologic Observation of Soft Tissue Acquired From TuberosityDocument7 pages(JOP) JUNG 2008 - Histologic Observation of Soft Tissue Acquired From TuberositydrjonduNo ratings yet
- A Report On Clinical Rotation January 2023Document14 pagesA Report On Clinical Rotation January 2023charles juma100% (1)
- Tog 12642Document9 pagesTog 12642saeed hasan saeedNo ratings yet
- Anaesthesia For BPTDocument38 pagesAnaesthesia For BPTBijeta ThapaNo ratings yet
- Anterior Open Bite Correction by Le Fort I or Bilateral Sagittal Split OsteotomyDocument18 pagesAnterior Open Bite Correction by Le Fort I or Bilateral Sagittal Split Osteotomyloren camila Daza GomezNo ratings yet
- Jaga Harkit TerakhirDocument10 pagesJaga Harkit TerakhirRONY PERMANANo ratings yet
- Treatment of Hyperprolactinemia A.7Document4 pagesTreatment of Hyperprolactinemia A.7Leyni fanny guerrero limaNo ratings yet
- Orthopaedics and Orthopaedic Nursing RNDocument70 pagesOrthopaedics and Orthopaedic Nursing RNFaith LwabilaNo ratings yet
- Result SaraDocument19 pagesResult SaraMalek BalaNo ratings yet
- Suture Patterns 2022Document45 pagesSuture Patterns 2022axel pqNo ratings yet
- Seminar: Treatment Planning in Orthodontic PatientsDocument105 pagesSeminar: Treatment Planning in Orthodontic PatientsVishal SharmaNo ratings yet
- Ochondra Ca 411Document66 pagesOchondra Ca 411joyrena ochondraNo ratings yet
- Pendahuluan Mastikasi: Suatu Pola TetapDocument28 pagesPendahuluan Mastikasi: Suatu Pola TetapBirgitaCaresaNo ratings yet
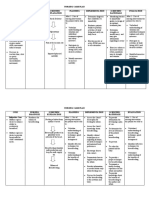
- Nursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective CuesDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective Cues24 PAULINO ALDRIN MUJARNo ratings yet
- Thesis On CT ScanDocument5 pagesThesis On CT ScanLiz Adams100% (2)