You might also like
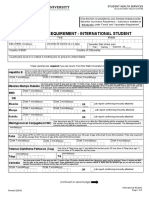
- Vaccination Requirement International Students 022019Document2 pagesVaccination Requirement International Students 022019KryzNo ratings yet
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- Immunization InstructionsDocument2 pagesImmunization InstructionsAli SadeqiNo ratings yet
- Univ of Florida ImmunisationDocument2 pagesUniv of Florida ImmunisationPavan Kumar MangipudiNo ratings yet
- Immun RecordDocument2 pagesImmun RecordNonofYaNo ratings yet
- 2024 VPD FormFINAL 16012024Document5 pages2024 VPD FormFINAL 16012024dkid9876No ratings yet
- VSLO Immunization Form 22-23Document6 pagesVSLO Immunization Form 22-23Will HNo ratings yet
- Immunization Record: Form Is Due at OrientationDocument3 pagesImmunization Record: Form Is Due at OrientationCasey JonesNo ratings yet
- FIU Immunization Documentation FormDocument2 pagesFIU Immunization Documentation FormMO MONo ratings yet
- Pre-Placement Immunization Form (June 2017) BrockDocument2 pagesPre-Placement Immunization Form (June 2017) BrockroldinpgNo ratings yet
- Form B - Other Jobs - High - V High Risk TBDocument8 pagesForm B - Other Jobs - High - V High Risk TBMorshed HumayunNo ratings yet
- Protocol SynopsisDocument5 pagesProtocol Synopsiscorina_lee_caseyNo ratings yet
- Immunization Requirement - Student Health Center - The University of UtahDocument2 pagesImmunization Requirement - Student Health Center - The University of Utahmithun916No ratings yet
- Immunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationDocument7 pagesImmunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationShubham TrivediNo ratings yet
- Memorandum: Faculty of DentistryDocument3 pagesMemorandum: Faculty of Dentistryabhinav guptaNo ratings yet
- CUB - Immunisation FormDocument2 pagesCUB - Immunisation FormArcane BeingNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloNo ratings yet
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 pagesHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikNo ratings yet
- On February 11, 2022, This Report Was Posted As An MMWR Early Release On The MMWR WebsiteDocument9 pagesOn February 11, 2022, This Report Was Posted As An MMWR Early Release On The MMWR WebsiteworksheetbookNo ratings yet
- Janssen Covid-19 Vaccine Journal Club ZwachteDocument4 pagesJanssen Covid-19 Vaccine Journal Club Zwachteapi-552486649No ratings yet
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Adult Schedule 11x17Document2 pagesAdult Schedule 11x17lcmurilloNo ratings yet
- San Diego Unified COVID-19 Vaccination RoadmapDocument17 pagesSan Diego Unified COVID-19 Vaccination RoadmapDillon DavisNo ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalNo ratings yet
- Vaccine Administration YES NO N.A. Vaccine Information Statements Are Being Provided To Every Patient, Parent, orDocument3 pagesVaccine Administration YES NO N.A. Vaccine Information Statements Are Being Provided To Every Patient, Parent, orkNo ratings yet
- Immunize Form 07282022Document3 pagesImmunize Form 07282022Bishworaj WaibaNo ratings yet
- Funeral Service-Education-Medical-RequirementsDocument4 pagesFuneral Service-Education-Medical-RequirementsalishamaeladouceurNo ratings yet
- Ivermectin JournalDocument11 pagesIvermectin JournalShahidatul Aqmal SahidinNo ratings yet
- 292-Report of Rapid Antigen Test ResultsDocument6 pages292-Report of Rapid Antigen Test ResultsNathan CHOWNo ratings yet
- Immunization Form For Students 2019-20 FINAL 2Document2 pagesImmunization Form For Students 2019-20 FINAL 2Rex ChanNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- Adult Schedule 6x4 5Document2 pagesAdult Schedule 6x4 5dr_ritamNo ratings yet
- Varilrix Detail Aid DraftDocument5 pagesVarilrix Detail Aid DraftpheverishNo ratings yet
- Immunization Submission FormDocument3 pagesImmunization Submission Formdimpiu11No ratings yet
- Tuberculosis FormDocument2 pagesTuberculosis FormSura SaadNo ratings yet
- Health Information FormDocument13 pagesHealth Information FormArtero-Cavallaro PabloNo ratings yet
- 2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12Document4 pages2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12James AllenNo ratings yet
- Immunization Letter NB FORM RevisedDocument6 pagesImmunization Letter NB FORM RevisedUddhavendra Pal SinghNo ratings yet
- Immunization Record PART I: To Be Completed by The Student. Please Print or TypeDocument3 pagesImmunization Record PART I: To Be Completed by The Student. Please Print or Typeruhayl khanNo ratings yet
- PSW6 - PPHFDocument16 pagesPSW6 - PPHFanishthNo ratings yet
- Lopez-Medina 2020Document12 pagesLopez-Medina 2020Johannus Susanto WibisonoNo ratings yet
- Rhodes Immunization RecordDocument5 pagesRhodes Immunization RecordDr.P.S.N RajuNo ratings yet
- Health History and Immunization Form: University of Valley Forge - Health CenterDocument4 pagesHealth History and Immunization Form: University of Valley Forge - Health CenterBernard AmetepeNo ratings yet
- Immreq15 16Document2 pagesImmreq15 16api-234991765No ratings yet
- Biswal 2020Document11 pagesBiswal 2020Johannus Susanto WibisonoNo ratings yet
- Mumps Vaccine Performance Among University Students During A Mumps OutbreakDocument9 pagesMumps Vaccine Performance Among University Students During A Mumps OutbreakNopita Speed3No ratings yet
- Immunization Requirement Form - UpdateDocument2 pagesImmunization Requirement Form - UpdateManojkumar ANo ratings yet
- Fact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2Document3 pagesFact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2marie-eve guyNo ratings yet
- Instructions For Completion of UA Immunization FormDocument4 pagesInstructions For Completion of UA Immunization FormJ StockmanNo ratings yet
- An Important FormDocument3 pagesAn Important FormRachel ColeNo ratings yet
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloNo ratings yet
- Vaccine Timing CDCDocument40 pagesVaccine Timing CDCanindita.prasidha.parameswariNo ratings yet
- Nejmoa 2115869Document11 pagesNejmoa 2115869carb0ne14rNo ratings yet
- Journal of Infectious DiseaseDocument6 pagesJournal of Infectious DiseaseSoham SarangiNo ratings yet
- COVID-19 Vaccine Comparison: Issue BriefDocument4 pagesCOVID-19 Vaccine Comparison: Issue BriefJimmy FebrianNo ratings yet
- (FORM) Medical Report AllDocument2 pages(FORM) Medical Report AllIndah AcphNo ratings yet
- 01CIM 01 - Clinical Pathway Managing TB CasesDocument10 pages01CIM 01 - Clinical Pathway Managing TB Casesyin sNo ratings yet
- Dengue Vaccines - Hindra I. SatariDocument33 pagesDengue Vaccines - Hindra I. SatarirodearniNo ratings yet
- Thomas 1992Document9 pagesThomas 1992ditaNo ratings yet
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- The Influence of English Language in CinemaDocument5 pagesThe Influence of English Language in CinemaLuna GoghNo ratings yet
- NP 3127 MT 3 Adaptive 439Document8 pagesNP 3127 MT 3 Adaptive 439Juan J SaizNo ratings yet
- PaperDocument17 pagesPaperNgoc Nguyen100% (1)
- Airspan ASMAX Product Brochure (QuantumWimax - Com)Document20 pagesAirspan ASMAX Product Brochure (QuantumWimax - Com)Ari Zoldan100% (1)
- Long-Term Impact and Sustainability of LIFE NatureDocument60 pagesLong-Term Impact and Sustainability of LIFE NatureEU LIFE ProgrammeNo ratings yet
- 0 Syllabus IoT Introduction Spring 2021Document25 pages0 Syllabus IoT Introduction Spring 2021Kỳ KhôiNo ratings yet
- Ques 1Document15 pagesQues 1Monisha ChaturvediNo ratings yet
- Igcse Ict Chapter 4 To 7 NotesDocument41 pagesIgcse Ict Chapter 4 To 7 Notesasfas asf as100% (1)
- 02-Technical Specification - GENERAL TECHNICAL REQUIREMENTS (Rev 12) PDFDocument77 pages02-Technical Specification - GENERAL TECHNICAL REQUIREMENTS (Rev 12) PDFSanjay RoutNo ratings yet
- Quang L Minh-New SAT Practise Test - ExamPrintReportDocument41 pagesQuang L Minh-New SAT Practise Test - ExamPrintReportKhoa NhậtNo ratings yet
- Environmental Systems and Societies Paper 2 SL MarkschemeDocument8 pagesEnvironmental Systems and Societies Paper 2 SL MarkschemeAfra LamisaNo ratings yet
- Peusangan 1 & 2 Hepp Construction Project: P.T. PLN (Persero)Document1 pagePeusangan 1 & 2 Hepp Construction Project: P.T. PLN (Persero)Jonri SitompulNo ratings yet
- PB1.3 CH1 Using NumbersDocument22 pagesPB1.3 CH1 Using NumbersGadgetGlitchKillNo ratings yet
- SS1 2ND Term Animal Husbandry E-NoteDocument23 pagesSS1 2ND Term Animal Husbandry E-Notekanajoseph2009No ratings yet
- Marketing Strategy Business PlanDocument50 pagesMarketing Strategy Business PlanShreyash PattewarNo ratings yet
- MCQSDocument6 pagesMCQSkhuzaima9100% (2)
- E-Learning SystemDocument82 pagesE-Learning SystemAbe BerhieNo ratings yet
- Hydraulic Units UP50: Issue: 11.2019Document80 pagesHydraulic Units UP50: Issue: 11.2019fabio coalaNo ratings yet
- Duties o SSE OHEDocument640 pagesDuties o SSE OHEAnonymous yizPBqNo ratings yet
- Walter J. Matweychuk, PH.DDocument3 pagesWalter J. Matweychuk, PH.DVenica AllenNo ratings yet
- Sripada Srivallabha Charitamrutam PDFDocument593 pagesSripada Srivallabha Charitamrutam PDFdimitriNo ratings yet
- EOC MC Problems Chapters 9 12 No AnswersDocument8 pagesEOC MC Problems Chapters 9 12 No AnswersTrisha Anne ClataroNo ratings yet
- Substation GroundingDocument24 pagesSubstation Groundingmmhaq1975No ratings yet
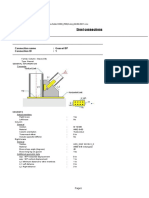
- Steel Connections: Detailed ReportDocument7 pagesSteel Connections: Detailed Reportgv Sathishkumar KumarNo ratings yet
- Ims656 Chapter 6-1 Isd Operational - Tech MGTDocument24 pagesIms656 Chapter 6-1 Isd Operational - Tech MGTMuhammad Amirull AdlanNo ratings yet
- Abs07 - 32.768 KHZ - : Applications: FeaturesDocument3 pagesAbs07 - 32.768 KHZ - : Applications: FeaturesHongdang DinhNo ratings yet
- Cardiac ReportDocument71 pagesCardiac ReportManoj KumarNo ratings yet
- Capital Structure-Sample Proposal 4Document34 pagesCapital Structure-Sample Proposal 4Ajay MagarNo ratings yet
- 17 4 Probability - Tree DiagramsDocument5 pages17 4 Probability - Tree Diagramsapi-299265916No ratings yet
- ENGR451 Notes 1 Winter 2019 PDFDocument158 pagesENGR451 Notes 1 Winter 2019 PDFWeixian LanNo ratings yet